Article Text

Abstract
Background Long-term complications and high costs of cerebral palsy (CP) as well as inconsistency in data related to this disease reveal the need for extensive planning to obtain accurate and complete data for the effective management of patients.
Objective The present study reviews the information architecture of CP information system.
Method The relevant articles published from early 1988 to 31 July 2018 were extracted through searching PubMed, Scopus, Cochran, Web of Science and Embase databases conducted independently by two researchers.
Results A total of 39 articles on CP information system were reviewed. Hospitals, rehabilitation centres and outpatient clinics were found to be the main organisations in charge of generating CP data. Each CP database used several data sources, with hospitals serving as the most important sources of information and the main generators of data. The main CP datasets were categorised into four groups of demographic data, diagnosis, motor function and visual impairment. The majority of data standards were related to the use of the International Classification of Functioning, Disability and Health and the Gross Motor Function Classification System. Finally, accuracy, completeness and consistency were the criteria employed in data quality control.
Conclusion Developing a robust CP information system requires deploying the principles of information architecture when developing the system, as these can improve data structure and content of CP system, as well as data quality and data sharing.
- Cerebral Palsy
- Information Architecture
- Information System
- Data sources
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cerebral palsy (CP) refers to a complex and multidimensional group of non-progressive but stable disorders in movement and posture experienced as a result of a neural lesion in the course of brain development (during the fetal period, birth, infancy and childhood).1 These disorders can affect all aspects of children’s development throughout their life.2 CP is often accompanied by seizures, speech abnormalities, verbal problems, vision disorders, reduced alertness, cognitive and behavioural disorders, sensory and perception problems, communication disorders, epilepsy and musculoskeletal problems.3 The symptoms of CP vary from one person to another and may change over time. Some individuals with CP may also be affected by other diseases, such as specific learning disorders and delayed development.4
Despite the advances in diagnostic technologies and detection of risk factors before and after birth, the average prevalence of CP has been reported as 2.11 per 1000 live births across the world.5 In developed countries, 2–2.5 infants per 1000 are born with CP. Moreover, the statistics indicate that CP affects more women than men and is more prevalent in whites than in blacks.6 It causes many economic problems and imposes heavy costs on patients, their families, the healthcare system and society.7 For instance, the average annual cost per CP patient has been reported to be $A43 431 in Australia and US$50 000 in the USA.8 9
The long-term and permanent complications as well as the high percentage of direct costs incurred for families reveal the need for extensive planning for the better management of this disease through obtaining up-to-date and efficient information.10 A key problem with CP is the spread and inconsistency of the related data and the lack of an integrated information system.9 11 An integrated CP information system is necessary as it can help improving disease control, identifying the most appropriate care plan and facilitating patient follow-ups through easy access to information. In addition, this system can lead to a more accurate identification of the prevalence, incidence and burden of the disease as well as the number of health centres, equipment and facilities required to provide services to these patients, thereby helping prioritise the national requirements for implementing future prevention, control and treatment programmes and activities.12
There have been different healthcare information systems for facilitating healthcare delivery.13 14 Besides these information systems that could help gathering, processing, storing and sharing data related to patient care,14 15 there are also registries that can help managing specific and extracted data mainly used by researchers and clinicians for outcome evaluation, patient follow-up and research.16 17 Information systems are regarded as information sources for an electronic health records system. This system only generates a summary of care data for different episode of care, while the detailed data are kept in the main information systems.18 19
Developing a well-designed CP information system integrated with other information systems requires applying the principles of information system architecture in practice.12 Information architecture, as a key aspect of information system architecture,20 21 is defined as a plan encompassing models, rules and policies that draw various data and are in charge of their collection, storage and retrieval, while also using and exchanging them across systems.22 With respect to CP information system, the information architecture provides a general view of the information that should exist in the system and can create a concrete foundation for data acquisition and sharing23 involving different groups including neurologists, neurosurgeons, occupational therapists and physiotherapists.17
Given the high prevalence of CP and the direct and indirect costs imposed on the healthcare system and society, the development of information architecture and its components such as databases and patient registry is essential for the proper management of costs, provision of services and treatment of patients with CP. Consequently, this study aimed to obtain a better understanding of CP information system and to determine the information architecture requirements, including organisations involved in data management, data sources and data bases, data elements, data standards, data sharing and data quality measures.
Methods
The process of searching and selecting articles is presented in figure 1. All relevant articles published from early 1988 to 31 July 2018 were extracted through a search in PubMed, Scopus, Cochrane, Web of Science and Embase databases. Research suggested using a combination of relevant databases for adequate and efficient coverage.24 25 All articles with the keywords CP, classification system, information system, registry, surveillance system, register, data set, data source and database in their title, abstract, MeSH (Medical Subject Headings) and Emtree were reviewed using AND/OR operators.

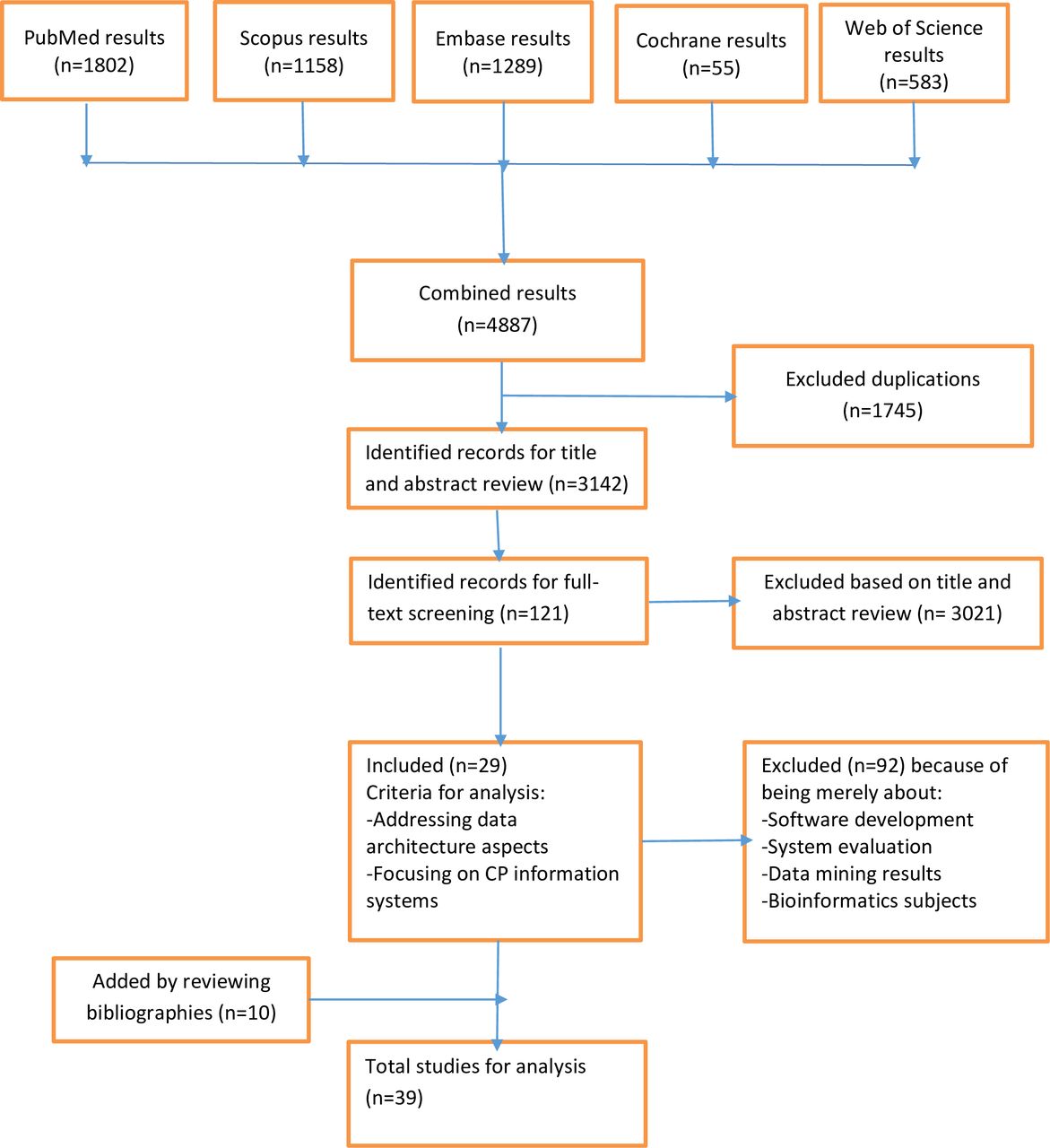{kind=link}
The process of paper selection. CP, cerebral palsy.
Data extraction
All articles related to CP were retrieved, and a list of their abstracts was prepared. Each article was reviewed independently by two authors (MA and RR), and the reason for both of them rejecting an article was given. In case of a disagreement, the article was further checked by other two authors (KE and AK). The required data were extracted using a predeveloped checklist, including research time, place, population, organisations involved in the production, data usage and monitoring, data sources and databases, data collection, data standards, data processing, data sharing and data quality.
Inclusion and exclusion criteria
All English publications with a focus on CP information systems addressing information architecture aspects, such as data elements, data sources and data sharing in different stages of system development, were included. All studies that merely focused on the design and evaluation of specific information system or data architecture with no focus on CP were excluded.
Study selection
A total of 4887 articles were extracted. These articles were initially input in EndNote and, 1745 duplications were removed. The review of titles and abstracts led to the exclusion of 3021 irrelevant articles, and after reviewing their full texts, a further 92 articles were excluded as not addressing the CP information architecture. Finally, 29 articles entered the study for a careful review. In the supplemental search, references provided in articles were also examined, and 10 more articles were included. As a result, a total of 39 articles were included in this review.
Results
A total of 39 articles on the components of CP information system architecture were reviewed, of which 13 had been conducted in Europe,23 26–37 10 in the USA,38–47 6 in Australia,48–53 7 in Asia1 12 54–58 and 3 in Africa.59–61
The results of the reviewed articles were classified in six groups, including organisations involved in the management of data, data sources, databases, datasets, data elements, data standards, data sharing and data quality (table 1).
Data architecture components
Organisations involved in data generation, adoption and governance
According to previous studies, organisations involved in the generation, adoption and governance of CP data are divided into three main groups: (1) organisations generating data, (2) organisations using data and (3) organisations coordinating and monitoring data (table 2). However, some of these organisations may belong to more than one group. The main organisations generating CP data include hospitals, rehabilitation centres and outpatient clinics.12 30 36
Organisations involved in data generation, adoption and governance
The most important organisations using data include rehabilitation research centres, CP associations and international, non-governmental and insurance organisations using the data generated in a variety of ways.27 29–31 33 35 36 38 39 41 50 51 53 55 56 59 60
The third group is responsible for enforcing rules and standards as well as monitoring data generation, processing, storage and use activities to ensure the safe and secure use of data. Examples of such organisations include the Surveillance of Cerebral Palsy in Europe (SCPE), Autism and Developmental Disabilities Monitoring (ADDM) in the USA and Australian Cerebral Palsy Register (ACPR).26 29 42
Databases and data sources
Databases are employed for the collection, processing and distribution of data in the form of information, or the management of information related to the incidence of diseases.62 63 The Korean Database of Cerebral Palsy (KDCP) is an example of such a database, aiming to create a national database for patients with CP across Asia. KDCP includes two databases: KDCP1 for people aged <4 years and KDCP2 for those aged four or above. KDCP comprises four data sources, including diagnosis and history, related problems, management and results.57 Another example is databases on intellectual disability in Europe, aiming to study the feasibility of creating a framework for monitoring and undertaking collaborative research on intellectual disability at the European level based on the existing databases of children with this disability. The characteristics of five existing European intellectual disability databases from four countries (Iceland, Latvia, Ireland and two in France) were discussed on the basis of ideal criteria set by a working group on childhood intellectual disability as part of the SCPE Network. The data sources of this database include medical records in hospitals, medical-social institutions, psychiatric centres (private and public sectors), doctors, psychiatrists, paediatricians and other professionals working in the health services.36
Irrespective of database design levels, each CP database uses several data sources, a summary of which is presented in table 3. The most important sources of obtaining data are hospitals as the main generators of CP clinical and epidemiological data. In addition, these databases may receive data from rehabilitation centres, research centres and associations. In some systems, patients or their relatives are able to input data related to the trend of the disease, the patients’ quality of life and other issues.
Identified common data sources in CP information system and registration networks
Datasets and data elements
Of the 39 articles reviewed, 20 (51.28%) had addressed datasets and their related elements. Dataset is the main and standard set of the required data elements, designed and employed to collect and report standard information nationwide.64 The CP data elements are generated and registered by four specialist groups in their routine clinical visits or surgical interventions. These four groups include non-surgeon physicians (paediatric growth specialists, neurologists and rehabilitation specialists), orthopaedic surgeons, neurology surgeons, occupational therapists and physiotherapists.65 The CP dataset includes the patients’ demographic information, types of CP, service providing centres, the patients’ medication and medical history, family history and records before and after birth. A summary of datasets is given in table 4.
The main categories of common data elements in CP registration and information system
Data standards
Twenty articles (51.28%) cited various international classifications of diseases, including ICD-10, International Classification of Functioning, Disability and Health (ICF), ICE-CY, Gross Motor Function Classification System (GMFCS) and Manual Ability Classification System (MACS), utilised for standardising datasets related to CP.1 23 27 28 36–41 43 44 46 49 50 54 57–59 61 The majority of cases were related to the use of ICF and GMFCS. The most commonly used standards are presented in table 5.
The most commonly used data standards
Data sharing
Fifteen studies indicated data sharing among different bodies (38.46%). The most important sharing data axes were: (1) data sharing among various organisations such as rehabilitation centres, CP associations, clinics and national CP databases, cited in 11 articles (28.2%) including the highest number of cases26 27 30 40 44 50 54 55 59–61; (2) data exchange of registry with data bases or registries indicated in nine articles26 27 30 40 41 50 53 55 59–61; (3) data sharing among universities, research centres and clinics, cited in seven articles26 27 40 41 50 60 61 and (4) data sharing among patients and their relatives with CP registries, cited in six articles (15.38%).40 44 46 53 54 59
Data quality control
The necessity of controlling the quality of data generated in the information systems was highlighted in 10 articles (25.64%).26 27 33 36 37 44 50 53 54 58 In seven articles (17.94%), the data producers were in charge of data quality control. Moreover, in five articles (12.82%), data coordinators and governors took this responsibility; in five articles (12.82%), the quality control committees or departments were involved in intersectorial cooperation; and in five articles (12.82%), a network of independent experts was involved in data quality control, for example, the review of the generated data based on predetermined criteria. A summary of the most common quality control measures is given in table 6. The majority of articles (eight articles, 20.51%) were on the control of the data entered by the patients or their relatives as well as data input by various medical specialists based on other sources. Furthermore, accuracy, completeness and consistency were the criteria applied for data quality control.
Data quality control procedures
Discussion
Attention to CP and awareness of the management problems of this disease have significantly increased over the last two decades.66 The first extensive network of care programmes for patients with CP entitled SCPE was established in Europe in 1998. Afterwards, the network of ADDM was formed in the United States in 2002, followed by the ACPR. These countries were considered as the pioneers in registering, setting standards and developing the network infrastructures for CP patients.50
In the present study, organisations involved in CP data management were classified into data generators, data users and coordinators. The CP clinics, hospitals and research centres are the main type of data generators, and these can be governmental or non-governmental. Ongoing monitoring and funding by monitoring organisations can significantly improve the performance of data generators. Research centres and scientific associations can use the quality data produced by the first group to generate a variety of data.
The governing organisations can also use these data indirectly (through research centres and academic associations) or directly to set the relevant policies.26 36 41 59 60
One of the problems identified in the present study was the existence of parallel data generating and collecting organisations. Occasionally, in addition to the national registries, other organisations, such as research centres, clinics and hospitals, may have their own databases. Developing an integrated national information network for CP, as seen in the USA and some European countries, is a key solution. In this national network, data duplication in various databases is avoided as the governing organisations apply control and coordination at different levels.26 27 41 42 50 54
It was found that there are a variety of data sources for CP information systems, causing difficulties in data organisation. One approach for reducing or eliminating this problem seems to be the transmission of data to a central database according to a specific and consistent pattern by various data sources such as hospitals, registries, clinics, research centres and biobanks.26 31 37 38 52 54
With respect to standards, WHO has presented an, ICF) to provide a common framework and language.23 Studies have demonstrated that the application of data standards increases compatibility, decreases data repetition and improves data sharing and collection efficiency.50
Data sharing at different levels is another key aspect of information architecture. A main type of data exchange can be seen between research centres or care settings and a CP database. Given that the majority of bodies involved in data interaction are data generators and data users, the communication with CP database is often reciprocal and, by providing clinical, epidemiological and research data via the database, they can receive meaningful data, such as the relationship between CP phenotype and genotype. Another type of data exchange can be the reciprocal data sharing between a database or central registry and other specialised databases or registries. These databases are usually in a network model, where the central database acts as a hub, so that stakeholders can access the required supplementary information.60 For data sharing, the data exchange standards, such as HL7, play a crucial role and provide a robust foundation for the integration of information systems.67
Another essential requirement for setting up CP information system architecture is maintaining data quality, which is a key for reporting purposes. The use of classification systems and data sharing standards can improve information system efficiency only when the collected data are of required quality. Applying measures such as data accuracy, data completeness and data consistency could help to maintain data quality. The aforementioned measures have been suggested as the key metrics for checking the quality of data in a number of studies.26 27 36 37 44 50 53 54 58 In addition, ongoing user training should be taken into consideration to make sure that checking the data quality is conducted appropriately and in line with instructions set.29 37
Conclusions
Deployment of information architecture principles when designing and developing an information system for CP could provide a coherent information context, thus facilitating data collection, organisation and sharing among different centres. This system could ultimately improve the provision of services, facilitate research and decrease the direct and indirect costs imposed on the health system and society.
Acknowledgments
This study was part of a PhD project conducted at Shahid Beheshti University of Medical Sciences in Iran.
References
Footnotes
Contributors All authors contributed to the conception and design of the work. MA drafted the manuscript, performed data collection and conducted the analysis in collaboration with RR. RR analysed the data in collaboration with MA and revised the manuscript critically. KE contributed to the interpretation of data and revised the manuscript critically. AK revised the manuscript critically. All authors approved the final version of the submitted manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.