Article Text

Abstract
Objectives Lupron 11.25 mg has both a narrow indication and a high cost compared to other Lupron presentations. Prior to our study initiation there was no clear distinction between presentations when ordering within the health-system’s Electronic Health Record (EHR). This resulted in inappropriate product selection, payment and billing errors that negatively impact our healthcare system. To reinforce prior education efforts, a new approach was considered leveraging the EHR with information to steer prescribers to the proper Lupron presentation based on indication. This study aimed to reduce off-label prescribing for Lupron 11.25 mg (NDC 00074-3663-03) by 25% by 02/28/2022 without negatively impacting the insurance collection rate.
Methods Baseline Lupron 11.25 mg adult kit administrations one year prior to intervention and off-label prescribing was found to account for 22.7% of administrations. In December 2021 intervention order questions were added to Lupron 11.25 mg in the EHR. One and two-month data was obtained after implementing order questions within the EHR. Lupron 11.25 mg administrations were classified into one of four categories to determine impact on off-label prescribing.
Results In the one- and two-month post-implementation periods off-label prescribing was 0% and 15.3% respectively, a reduction of 22.7% to and 7.4% respectively from the baseline assessment. There were no clinical denials found in either post-implementation reporting period.
Conclusion This report adds to the body of evidence that leveraging the EHR can lead to healthcare savings and illustrates how patient and healthcare system burden can be reduced by prompting thought and direction when a medication has indication specific dose requirements.
- Clinical Pharmacy Information Systems
- Decision Support Systems, Clinical
- Evidence-Based Medicine
- Medical Order Entry Systems
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Clinical Pharmacy Information Systems
- Decision Support Systems, Clinical
- Evidence-Based Medicine
- Medical Order Entry Systems
At our health system, several cases of high-cost administrative denials for Lupron Depot (Lupron) 11.25 mg kit for intramuscular injection occurred. Providers were educated on the proper strength for the desired indication but off-label prescribing, and subsequent denials persisted. Lupron 11.25 mg has both a narrow indication and a high cost compared with other Lupron presentations, yet prior to our study initiation, there was no clear distinction between presentations when ordering within the health system’s electronic health record (EHR). Resultantly, providers often selected the inappropriate presentation, leading to payment and billing errors that negatively impact both our healthcare system and patients. Recognising individualised education does not have a profound impact across a multistate health system and desire to prevent selection of Lupron 11.25 mg further upstream, a new approach was considered leveraging the EHR with information to steer prescribers to the proper Lupron presentation based on indication.
Healthcare providers strive to strike a balance between quality and cost-effective care. Complicated insurance policies and flawed EHR systems can lead to cost-ineffective care negatively impacting healthcare systems, providers and patients. In 2001, a national database review of medications prescribed and associated diagnoses found that 21% of prescriptions were written for an off-label indication.1 Survey data performed in the outpatient setting for paediatrics have found even higher incidences of off-label prescribing ranging from 67% to 96%.2
Lupron 11.25 mg has a narrow Food and Drug Administration (FDA) indication of endometriosis and uterine fibroids and its wholesale acquisition cost is US$3398 per dose.3 4 Lupron carries off-label endorsement for the treatment of gender dysphoria, fertility preservation, ovarian and prostate cancer, premenstrual syndrome and more.3 Many insurance companies will reimburse for off-label uses so long as they are endorsed by a national compendia guideline or listed in Micromedex DRUGDEX (Micromedex) as a non-FDA class I, IIa or IIb indication; it is prudent to consider prior authorisation (PA) before administration particularly when prescribing for off-label uses. The time-consuming steps to obtain PA and appeal insurance denials is necessary, costly and time-consuming.5
Complicated and poor EHR system design coupled with high expectations of provider performance may contribute to errors in prescription ordering.6 By implementing a set of order questions based on both approved and Micromedex endorsed off-label uses, this study aimed to reduce off-label prescribing for Lupron 11.25 mg (NDC 00074-3663-03) by 25% by 28 February 2022 without negatively impacting the insurance collection rate. We expected to improve patient experience by reducing unexpected billing and payment amounts for which patients are responsible.
Baseline Lupron 11.25 mg adult kit administrations among patients were tracked for 1 year prior to intervention. In December 2021, additional provider education and intervention order questions were added to Lupron 11.25 mg in the EHR. One and 2-month data were obtained after implementing order questions within the EHR. Lupron 11.25 mg administrations were classified into one of four categories: off-label, on-label, non-FDA approved class I or non-FDA approved class IIb indications, and insurance collection rates were tracked. We tracked all administrations and payer types but excluded self-pay collection ratios from insurance collection rates. Insurance collection rates were assessed internally comparing 1 January 2021–30 April 2021 to 1 January 2022–30 April 2022.
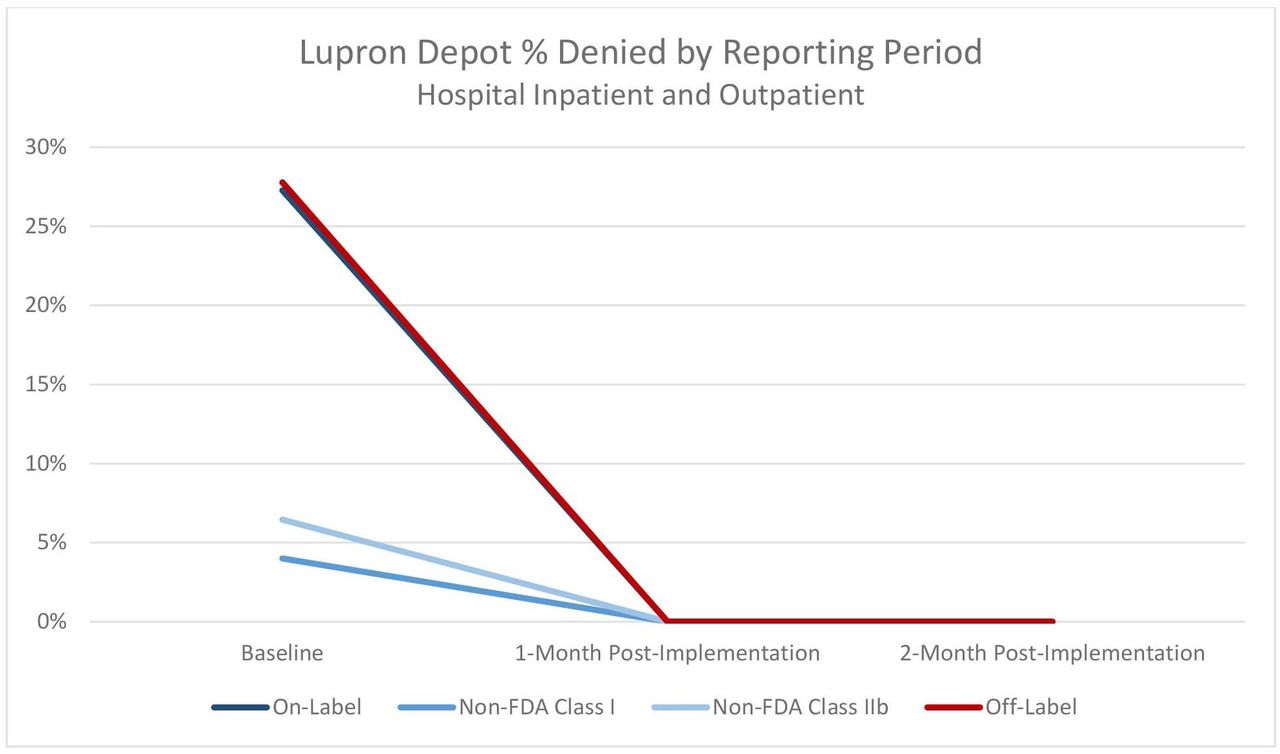
At baseline, there were 220 medication administrations for Lupron 11.25 mg including 50 off-label administrations billed with risk of underpayment compared with 49 on-label, 27 non-FDA approved class I, and 94 non-FDA approved class IIb administrations (figure 1). Off-label prescription use was 23% of the total administrations with a corresponding 28% denial rate (figure 2).

Lupron Depot 11.25 mg Adult Kit Uses by classificationa–c. aBaseline; 1 September 2020–31 August 2021. b1-month postimplementation: 1 January 2022–31 January 2022. c2-month postimplementation: 1 February 2022–28 February 2022. FDA, Food and Drug Administration.

{kind=link}
{kind=link}
Lupron Depot 11.25 mg Adult Kit Percentage Denied Claims by Reporting Perioda–c. aBaseline: 1 September 2020–31 August 2021. b1-month postimplementation: 1 January 2022–31 January 2022. c2-month postimplementation: 1 February 2022–28 February 2022. FDA, Food and Drug Administration.
The 1-month postintervention revealed 36 Lupron 11.25 mg administrations across the health-system. Of those 36 administrations, the following were assessed: 0 off-label administrations, 14 on-label administrations, 13 non-FDA class I administrations and 9 non-FDA class IIb administrations (figure 1). There were no denials due to clinical indication reported in the 1-month postintervention assessment (figure 2).
The 2-month postintervention revealed 13 Lupron 11.25 mg administrations across the health system. Of those 13 administrations, the following were assessed: two off-label administrations, eight on-label administrations, one non-FDA class I administrations and two non-FDA class IIb administrations (figure 1). Off-label prescription use was 15%, administered in the inpatient setting, but did not result in denial of the claim due to clinical indication (figure 2).
Through provider education and leveraging the EHR to guide prescribers on FDA-approved indications, National Comprehensive Cancer Network guideline supported uses and ensuring an additional selection option to cover off-label use when PA has been obtained, we reduced off-label prescribing without adversely impacting the insurance collection rate. This adds to the body of evidence that leveraging tools within the EHR can result in healthcare savings.7 8 Furthermore, this report illustrates how patient and healthcare system burden can be reduced by prompting thought and direction when a medication has indication specific dose requirements. Limitations existed in the ability to educate all prescribers across the health system, which may have influenced study results.
Ethics statements
Patient consent for publication
Footnotes
Twitter @JensenChelsee1
Contributors We appreciate support and collaboration from our pharmacy informatics colleagues at Mayo Clinic on pursing this initiative including Cheryl Olson PharmD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.