Article Text

Abstract
Objectives To develop and evaluate machine learning models to detect patients with suspected undiagnosed non-alcoholic steatohepatitis (NASH) for diagnostic screening and clinical management.
Methods In this retrospective observational non-interventional study using administrative medical claims data from 1 463 089 patients, gradient-boosted decision trees were trained to detect patients with likely NASH from an at-risk patient population with a history of obesity, type 2 diabetes mellitus, metabolic disorder or non-alcoholic fatty liver (NAFL). Models were trained to detect likely NASH in all at-risk patients or in the subset without a prior NAFL diagnosis (at-risk non-NAFL patients). Models were trained and validated using retrospective medical claims data and assessed using area under precision recall curves and receiver operating characteristic curves (AUPRCs and AUROCs).
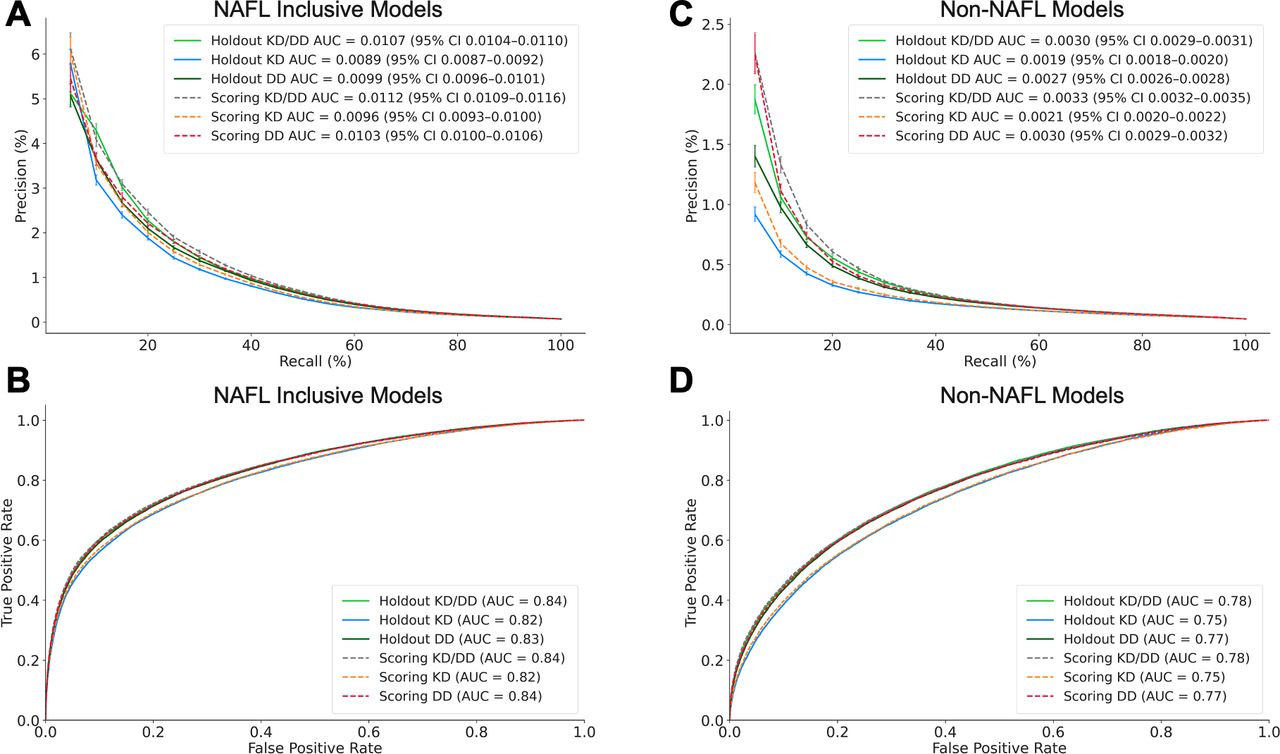
Results The 6-month incidences of NASH in claims data were 1 per 1437 at-risk patients and 1 per 2127 at-risk non-NAFL patients . The model trained to detect NASH in all at-risk patients had an AUPRC of 0.0107 (95% CI 0.0104 to 0.0110) and an AUROC of 0.84. At 10% recall, model precision was 4.3%, which is 60× above NASH incidence. The model trained to detect NASH in the non-NAFL cohort had an AUPRC of 0.0030 (95% CI 0.0029 to 0.0031) and an AUROC of 0.78. At 10% recall, model precision was 1%, which is 20× above NASH incidence.
Conclusion The low incidence of NASH in medical claims data corroborates the pattern of NASH underdiagnosis in clinical practice. Claims-based machine learning could facilitate the detection of patients with probable NASH for diagnostic testing and disease management.
- machine learning
- artificial intelligence
- BMJ Health Informatics
- data science
- medical records
Data availability statement
No data are available. All data belongs to IQVIA.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
What is already known?
Non-alcoholic steatohepatitis (NASH) is difficult to detect without an invasive liver biopsy and is underdiagnosed despite the risk of progression to cirrhosis.
Machine learning (ML) models trained on real-world data have shown promise in detecting rare or underdiagnosed diseases such as NASH.
What does this paper add?
This study extends the existing literature on ML applications in healthcare by incorporating high coverage medical claims data as a scalable strategy for detecting patients with likely NASH.
How this study might affect research, practice or policy?
This study may increase awareness of NASH underdiagnosis and under-reporting in clinical practice.
This study may serve as a basis for future research aimed at validating ML models to support NASH diagnosis in the clinical setting.
Background
Non-alcoholic fatty liver disease (NAFLD) is an umbrella term that describes two subtypes of liver disease: non-alcoholic fatty liver (NAFL) and non-alcoholic steatohepatitis (NASH).1 2 NAFL is characterised by fat accumulation (steatosis) in the liver without significant inflammation. NASH is a more severe form of NAFLD and is characterised by steatosis with inflammation and fibrosis, which can progress to cirrhosis.1 The prevalence of NAFLD in the USA is estimated to be 24%–26% of adults, of whom an estimated 20%–30% have NASH.3
The transition from simple hepatic steatosis to NASH is a crucial point in the development of severe liver disease, putting patients at higher risk for fibrosis and progression to chronic liver disease.4 Nevertheless, NASH is often underdiagnosed in clinical practice.5–7 This may be due to several factors. First, there is a lack of clear patient symptoms and reliable biomarkers to help identify NASH,8 9 and there are no universal routine screening standards.10 Second, liver biopsy is the gold standard for NASH diagnosis but is costly, invasive, complicated by sampling errors and requires a specialist to perform.4 11 Finally, despite ongoing clinical trials, there are currently no approved pharmacological treatments for NASH outside of India.12 Thus, detection of NASH remains a challenge and reliable diagnostic tools, including minimal or even non-invasive techniques, are warranted.
Machine learning (ML) with real-world data may help address the underdiagnosis of common and rare diseases. We recently demonstrated the application of ML in a retrospective case–control cohort study based on a US claims database to identify patients with undiagnosed hepatitis C virus.13 For the detection of NASH, studies have yielded encouraging results using metabolomics,14–17 electronic health records18–20 or combined clinical-claims data.21 The use case of each approach may be influenced by the chosen data type, characteristics of the model training population or the targeted application to patients with documented NAFL. Continuing to build on these efforts will further enable ML approaches to facilitate NASH detection.
This study examined supervised ML using medical claims as a non-invasive strategy to identify patients with likely NASH who might benefit from appropriate clinical follow-up such as monitoring or diagnostic screening. We used a retrospective rolling cross-sectional study design22 by taking multiple snapshots of patient prescription and medical claim histories to emulate patient data during real-world deployment while providing examples of patients with NASH for model training at different points in the patient journey prior to diagnosis. We also evaluated both knowledge-driven (‘hypothesis-driven’) and automated data-driven strategies in developing clinical predictors for NASH detection.
Methods
Data sources
Data were extracted from IQVIA’s proprietary US longitudinal prescription (LRx) and non-adjudicated medical claims (Dx) databases.13 LRx receives nearly 4 billion US prescription claims annually with coverage of 70%–90% of dispensed prescriptions from retail, mail order and long-term care channels. Dx receives over 1.35 billion US medical claims annually and covers approximately 70% of American Medical Association physicians. Dx data are derived from office-based individual professionals, ambulatory, general healthcare sites, hospitals, skilled nursing facilities and home health sites and includes patient-level diagnostic and procedural information.
All data were de-identified using an automated de-identification engine prior to being accessed by IQVIA. Both LRx and Dx data sets (hereafter referred to as LRxDx) are linked using anonymous patient tokens that support IQVIA data set interoperability and permits longitudinal linkage across patient histories. This anonymisation process is certified as Health Insurance Portability and Accountability Act compliant and Institutional Review Board exempt. IQVIA holds all requisite titles, licenses and/or rights to license this Protected Health Information for use in accordance with applicable agreements. LRxDx data spanning the study period from 1 October 2015 to 30 June 2020 were used for cohort selection and predictive feature engineering. Dx data between 1 January 2010 and 1 October 2015 were used only to exclude patients with an existing International Classification of Disease-9 (ICD-9) NASH diagnosis before study initiation. This study was conducted using the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis reporting guidelines.
Patient selection
An overview of the patient populations used for cohort identification is shown in figure 1A. Patients with a history of obesity, type 2 diabetes mellitus (T2DM), metabolic disorder or NAFL were selected to include individuals who also had precursors and risk factors for NASH.23 This has the effect of enriching the patient population to ensure that an algorithm learns a prediagnosis footprint specific to NASH rather than simply distinguishing between healthy and sick patients or between patients with highly dissimilar symptomologies. This cohort was stratified to remove patients with claims for liver cancer, liver failure or alcohol-related liver disease and other liver complications that might disqualify patients from clinical intervention for NASH. Additional eligibility criteria were presence in both LRxDx for at least 24 months, recorded sex and age from 18 to 85 years at the time of model prediction. See online supplemental table 1 for cohort stratification criteria.
Supplemental material

Cohort selection and model development. (A) Patients were identified from the general population (1) who met study stratification criteria (2). A subset of eligible patients was classified as likely to have NASH as evidenced by either a NASH diagnosis within 6 months after model prediction (3) or a diagnosis for non-alcohol-related liver fibrosis, sclerosis or cirrhosis within 6 months after model prediction and in proximity to a NAFL diagnosis (4). Eligible patients with no evidence of NASH were used as adversarial training examples, that is, patients with an overlap in symptoms, treatments and timing of resource utilisation but who were not patients with NASH. Patients with an existing NAFL claim in the previous 24 months overlapped with the patients with probable NASH population (5). Multiple time-bound cross-section were derived from the at-risk patient population (B). Cross-section 8 was reserved as a holdout set for model validation since it was sufficiently offset to prevent temporal overlap with the training set outcome window. Simulated model deployment using a prospective validation (scoring) set was performed by training on cross-sections 1–6 or on cross-sections 1–8 and using cross-section 10 as the test set. The NAFL inclusive and non-NAFL modelling cohorts used for model development (C). NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis.
Rolling cross-section study design
To develop algorithms to detect NASH at different points of the prediagnosis patient journey (e.g., 1 month prediagnosis, 3 months prediagnosis), we divided patient claims history into a rolling series of time-bounded cross-sections (i.e., rolling cross-sections (RCS)). The application of this approach to disease detection is discussed in more detail elsewhere.22 Briefly, we divided longitudinal patient claims data over the study period into 24-month lookback periods followed by a 6-month outcome window, each shifted by 3-month increments (figure 1B). The lookback period was used to apply stratification criteria and extract data for feature engineering. The most recent date in the lookback period (the index date) represents the starting time point of model prediction.
Patients with probable NASH were labelled using the earliest occurrence of two criteria:
A NASH diagnosis in the outcome window.
A diagnosis for non-alcohol-related liver fibrosis, sclerosis or cirrhosis during the outcome window with a NAFL diagnosis within the preceding 24 or subsequent 6 months. These patients were presumed undiagnosed or unrecorded NASH patients as this clustering of diagnoses is indicative of NASH1 and are therefore referred to as NASH proxy patients. These patients had no other liver diagnosis for their cirrhosis.
See online supplemental table 2 for NASH labelling criteria.
A total of 152 476 patients met the selection criteria for patient with NASH labelling. Patients who met the selection criteria during the lookback period without evidence of NASH during or before the cross-section outcome window formed an at-risk control patient pool. A total of 54 976 837 at-risk control patients were initially identified and then randomly downsampled to a ratio of one patient with NASH per five at-risk control patients per cross-section to facilitate model training resulting in 1 312 351 at-risk patients for adversarial training.
Two modelling strategies were undertaken for NASH detection. The first (figure 1C, NAFL inclusive modelling) sought to detect NASH among all at-risk patients to maximise clinical impact. We also hypothesised that patients with documented NAFL might already be suspected of NASH and that this might limit the clinical utility of algorithm-based NASH screening. We therefore investigated a second modelling approach (figure 1C, non-NAFL modelling) by excluding patient cross-sections with a NAFL diagnosis claim during the lookback period.
Feature engineering
We used two methods for feature engineering. The first, a knowledge-driven (KD) approach, applied domain expertise to curate clinical codes into medical concepts associated with NASH risk such as relevant comorbidities, symptoms, procedures and treatments. The second, a data-driven (DD) approach, extracted clinical codes that were present in the NASH or at-risk control patient cross-section lookbacks. Codes of each type, for example, diagnoses or procedures, were then selected based on the largest absolute difference in prevalence between NASH and at-risk control patients with the motivation that these codes should be discriminatory predictors. DD feature identification was performed only with training cross-sections 1–6 to avoid data leakage from future cross-sections used for model validation. Patient demographics (age and sex) were included as model predictors to complement KD/DD feature sets and were included in all modelling scenarios.
Date differences and frequencies for claim and specialty visits were calculated over each patient lookback period. Date differences were calculated as the number of days between the first and last claim for a given feature relative to the index date and the number of days between the first and last claim. Missing data were represented as zero for frequency features and as null for date difference features since null values are handled inherently by the ensemble algorithm used. See online supplemental tables 3-5 for clinical concepts used to derive model predictors.
Model selection
Gradient boosted trees24 using the XGBoost package25 were trained to discriminate between NASH and at-risk control patients. XGBoost was selected based on its previous success in benchmarking against other disease detection algorithms using claims data,13 26 its suitability over deep learning for tabular data27 and its compatibility with sparse claims data sets and scalability.25 Training cross-sections 1–6 were used for recursive feature elimination for feature selection (online supplemental figure 1) and for hyperparameter optimisation using grid search (online supplemental table 6).
Model evaluation
Models were evaluated using the area under the precision recall curve (AUPRC).28 To compensate for random downsampling of the at-risk control cohort, precision was scaled to the 6-month incidence of NASH in the at-risk patient population before downsampling, which was 1 per 1437 and 1 per 2127 patients for the NAFL inclusive and non-NAFL cohorts, respectively. Such scaling ensures that the number of false positives used to calculate precision is not underestimated and accurately reflects the incidence of NASH captured in claims data. Model precision using 95% CIs were approximated by treating each recall decile as a binomial distribution with n patients and a Bernoulli trial success probability of p. We then determined the uncertainty of p using a beta distribution with true and false positive predictions. The receiver operating characteristic curve and the corresponding area under the curve (AUROC) are given for reference. Feature importance was examined using SHAP (SHapley Additive exPlanations).29
Algorithms were compared with screenings for NASH using evidence of NAFL or T2DM in the last 2 years of a patient’s claims history (see online supplemental table 7 for qualifying clinical codes). Precision and recall of NAFL or T2DM screening were measured in NAFL inclusive and non-NAFL holdout sets. Model precision was then measured at the corresponding recall of each screening. The non-NAFL model was compared only to screening with T2DM.
Results
Study cohort
The NAFL inclusive and non-NAFL modelling cohorts displayed similar clinical profiles. T2DM was more common in patients with NASH (67.1% NASH and 56.3% at-risk and 70.4% NASH and 56.4% at-risk patients in the NAFL inclusive and non-NAFL cohorts, respectively). Obesity was common in patients with NASH and in at-risk controls regardless of NAFL history (59.8% vs 59.3%). NAFL was 10-fold more common in patients with NASH compared with at-risk controls (table 1).
Cohort statistics
Model performance
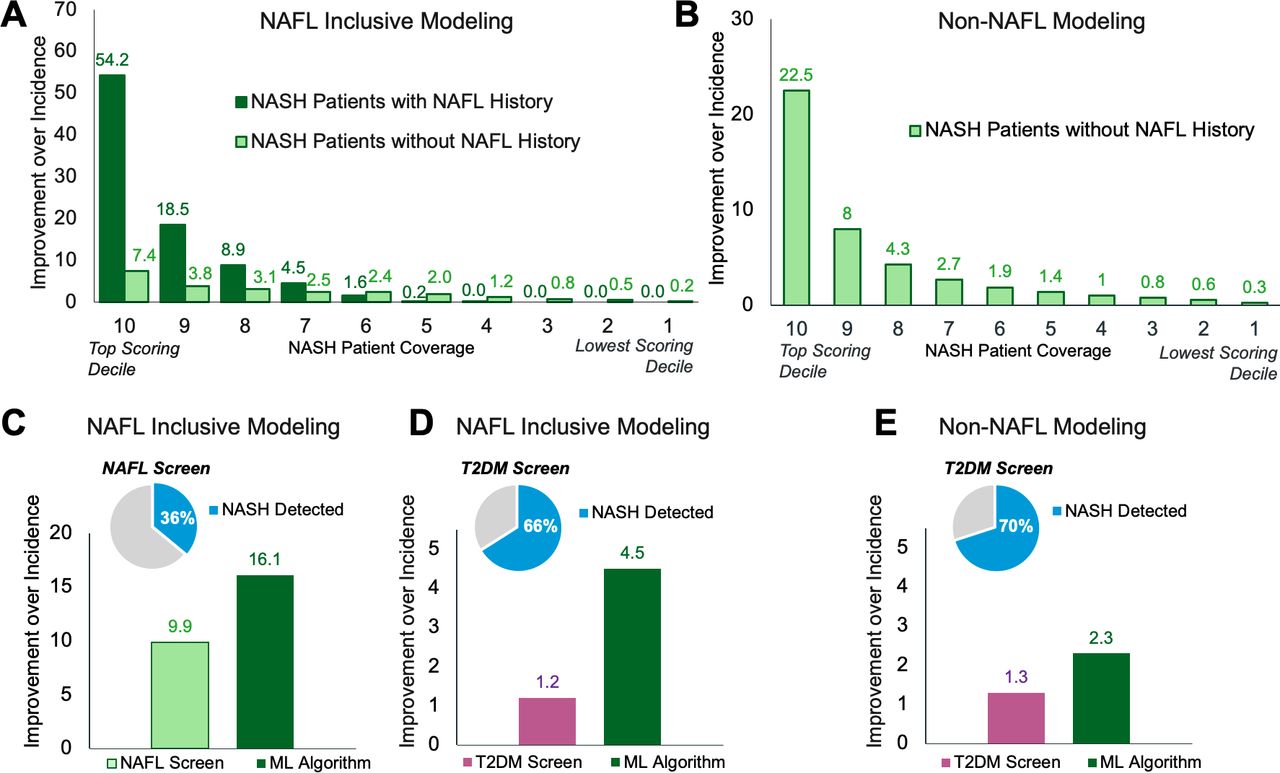
NAFL inclusive modelling detected patients with probable NASH in the at-risk holdout population with 0.0107 AUPRC (95% CI 0.0104 to 0.0110) and 0.84 AUROC (figure 2A,B). At 10% recall, the model detected patients with probable NASH with 4.3% precision (figure 2A). This represents a 60-fold improvement over the 6-month incidence of NASH, that is, if at-risk patients were randomly screened for NASH (figure 3A). Patients labelled using a NASH diagnosis or NASH proxy criteria were detected with an AUPRC of 0.0059 and 0.0051, respectively (online supplemental figure 3).
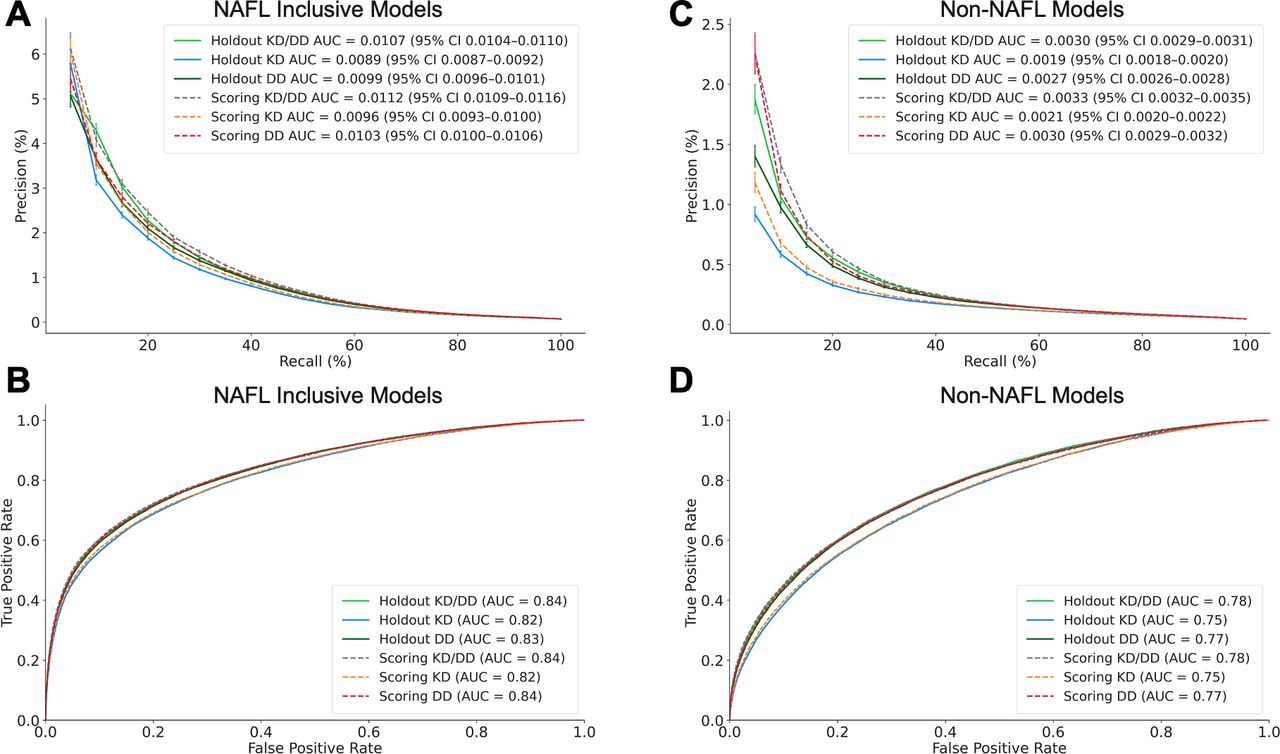
Model performance. Precision recall and receiver operating characteristic curves for model performance in detecting NASH in the NAFL inclusive (A and B) and non-NAFL (C and D) holdout and scoring validation sets. Precision is scaled to the 6-month NASH incidence observed in claims data. AUC, area under the curve; DD, data-driven; KD, knowledge-driven; NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis.
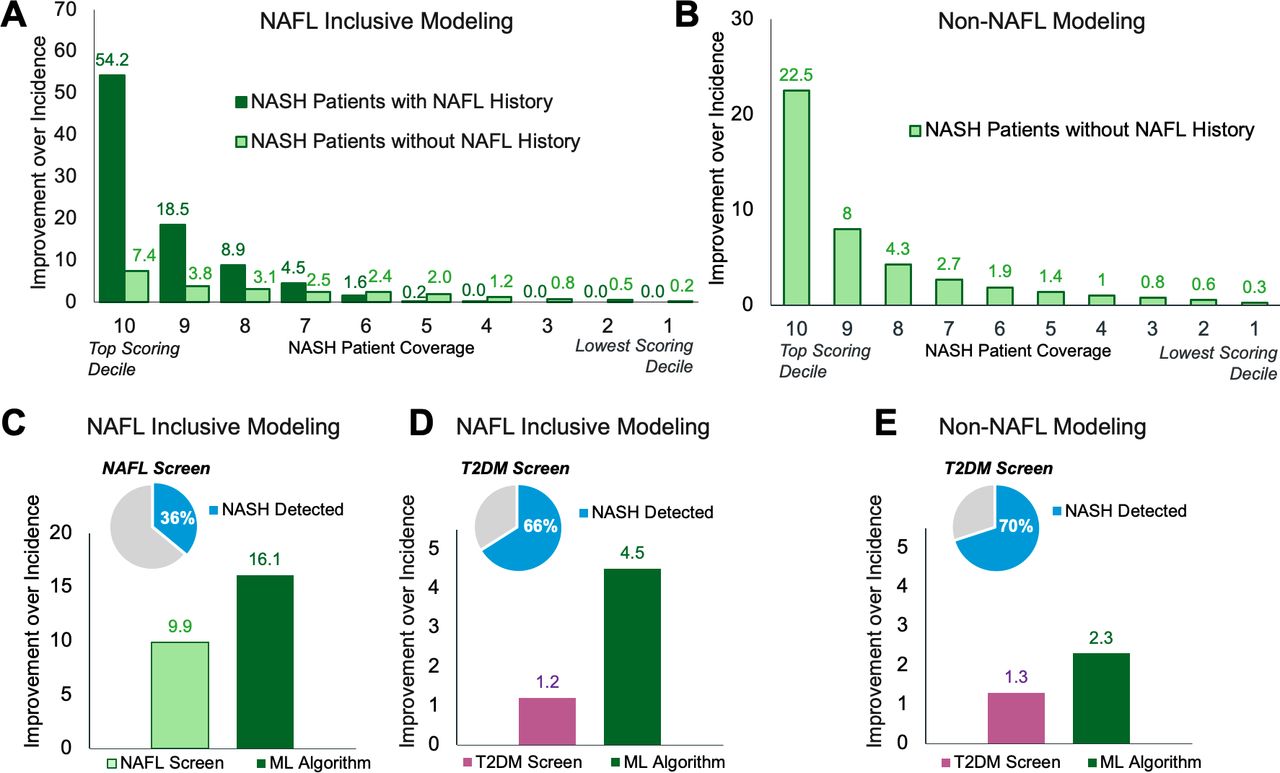
Model benchmarking. The fold improvement in model precision over the 6-month incidence of NASH observed in medical claims data and proportions within recall deciles of patients with predicted NASH with and without a NAFL diagnosis during the lookback period (A and B). Benchmark comparisons between NASH detection by ML algorithms and NASH screening using NAFL (C) or T2DM (D and E). The fold improvement over precision is calculated as the precision within each recall quantile divided by NASH incidence. ML, machine learning; NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis; T2DM, type 2 diabetes mellitus.
NAFL is a precursor of NASH; however, only 35% of patients with NASH received a NAFL diagnosis claim during their 24-month lookback period (table 1). Therefore, we developed a second model to detect patients with NASH in the non-NAFL cohort. The non-NAFL model identified patients with probable NASH with 0.0030 AUPRC (95% CI 0.0029 to 0.0031) and 0.78 AUROC (figure 2C,D). At 10% recall, this model detected patients with probable NASH with 1% precision, a 20-fold improvement over the incidence of NASH in this cohort (figure 3B). A comparable number of patients with NASH without NAFL were detected at approximately 30% recall by the NAFL inclusive model.
For both NAFL inclusive and non-NAFL cohorts, model precision and recall in the holdout set (i.e., train on cross-sections 1–6, test on 8) were comparable to that of the prospective validation set (i.e., train on cross-sections 1–8, test on 10) (figure 2A). In addition, models trained on cross-sections 1–6 and then tested on either the holdout or prospective validation set showed comparable performance (online supplemental figure 2), indicating model stability over a 6-month period.
ML surpassed the precision of NASH detection when screening at-risk patients with NAFL or T2DM claims and is presented as a fold improvement over the baseline incidence of NASH in claims data. In the NAFL inclusive cohort, NAFL screening detected 36% of likely patients with NASH with 9.9-fold precision (figure 3C), whereas the NAFL inclusive model detected the same number of patients with NASH (i.e, equivalent recall) with 16.1-fold precision (figure 3C). Screening with T2DM detected 66% of patients with likely NASH with 1.2-fold precision versus 4.5-fold precision with the NAFL inclusive model (figure 3D). In the non-NAFL cohort, T2DM screening detected 70% of patients with likely NASH with 1.3-fold precision, whereas the non-NAFL model improved precision by 2.3-fold for the same recall (figure 3E).
To evaluate the relative effectiveness of each feature engineering strategy, we compared the performance of models optimised with a mixture of KD and DD features to those optimised with one of the two feature types. Models developed with DD features performed slightly better than models developed with KD features. However, detection of NASH was maximised using the combination of KD and DD features (figure 2).
Model interpretation
To gain insight into which clinical factors drive algorithmic detection of NASH, we examined feature importance using SHAP (figure 4). As attributes (e.g., claim frequency and claim recency) may be correlated within a single feature, we ranked the top features by taking the cumulative sum of the absolute SHAP values for attributes within each feature. For the NAFL inclusive model, a prior NAFL diagnosis was the dominant clinical predictor accounting for 13% of the total contribution (figure 4A). In contrast, the top features were more evenly distributed in the non-NAFL model (figure 4B). Although trained independently, KD and DD models relied on similar clinical event types including comorbidities (T2DM), laboratory findings (abnormal liver function studies and abnormal serum enzyme levels) and diagnostic procedures (abdominal ultrasonography) (figure 4C–F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Feature Importance. SHAP values for top model features and the contribution of feature attributes, that is, claim frequency, time from first and final claim relative to the cross-section index date, time between the first and final claim occurrence and patient demographics for NAFL inclusive and non-NAFL combined KD/DD feature models (A–B), KD features models (C–D) and DD features models (E–F). SHAP values are expressed as a percentage of the total mean absolute SHAP values for models deployed on the holdout validation set. DD, data-driven; KD, knowledge-driven; NAFL, non-alcoholic fatty liver; NASH, non-alcoholic steatohepatitis; SHAP, SHapley Additive exPlanations.
Discussion
This study provides encouraging results for the use of medical claims data and ML to detect patients with likely NASH from large at-risk patient populations. Although there are no universally accepted routine screening standards for NASH,10 both NAFL and T2DM are well-recognised risk factors.2 Nonetheless, claims-based algorithms outperformed NASH screening using NAFL or T2DM history alone. In addition, algorithms detected probable NASH in at-risk patients without documented NAFL, potentially representing an overlooked NASH risk group. Approaches such as this may support more targeted screening of prevalent and underdiagnosed diseases and may be particularly valuable when diagnosis requires invasive or costly procedures or when clinical risk factors that could be used to screen patients are imprecise.
We investigated two methods that may broadly inform ML healthcare applications. First, we evaluated an automated DD approach to feature engineering for algorithmic disease detection. Model performance was greatest when KD and DD features were combined, suggesting that the two feature engineering methods make complementary contributions by integrating clinical and epidemiological knowledge with an empirically oriented process of scientific inquiry. Such automated approaches may improve knowledge discovery in real-world data while reducing the burden on clinical domain experts. Second, our RCS method can facilitate the creation of cohorts using longitudinal health data and provide opportunities to monitor healthcare market dynamics that may impact model performance.
These models represent claims-based screening tools to facilitate the identification of patients with likely NASH who may benefit from clinical follow-up (e.g., via FibroScan) and as proof of concepts for further clinical validation. Potential users of these models include providers or payers who wish to implement high volume screening for suspected NASH in an at-risk patient population. While the NAFL inclusive model is suited for broad NASH detection, the non-NAFL model may be appropriate for screening patients for NASH for whom NAFL status is not well documented or a reliable cause of medical care.
There are several limitations in this study. First, model precision is likely underestimated due to NASH underdiagnosis and under-reporting,5–7 which may inflate the false positive rate in model evaluation. Changes in clinical practice that facilitate NASH diagnosis should close the gap between observed incidence in claims and epidemiological estimates while also enabling the development of more powerful claims-based models. Second, our NASH labelling criteria do not guarantee NASH, which requires histological confirmation with a liver biopsy. The low percentage of patient cross-sections with a liver biopsy claim in this study may be due in part to limited coverage of this procedure in this data set. In addition, liver biopsy may not be performed in all cases, as a 2014 survey found that less than 25% of gastroenterologists and hepatologists routinely perform a biopsy to confirm NASH diagnosis.6 Clinical validation of these models would need to be performed on patients with liver biopsy-confirmed NASH and ideally assessed using multiple distinct medical claims data sets. Third, models were trained to detect patients with probable NASH regardless of NASH stage. Additional data types may enable stage specific NASH labelling for more targeted clinical interventions. Fourth, this study used a 6-month outcome window for NASH detection, which was chosen to allow indexing on more recent claims data. However, progressive diseases such as NASH may also benefit from longer prediction horizons to enable earlier detection. Finally, the robustness of our feature engineering strategy should be determined in subsequent sensitivity analyses using a broader range of techniques such as cost-sensitive or semi-supervised learning to address class imbalances30 as well as alternative ML algorithms and clinical targets.
Conclusions
In this study, we investigated claims-based ML as a non-invasive and scalable approach to stratify patients with probable NASH from an at-risk population for clinical follow-up. We also demonstrated automated DD feature engineering and an RCS study design in the development of disease detection algorithms. Models from this study or derivatives thereof could support more precise screening for NASH and help connect patients with available and emerging therapies.
Data availability statement
No data are available. All data belongs to IQVIA.
Ethics statements
Patient consent for publication
Ethics approval
The claims data used in this study were previously collected and statistically deidentified and are compliant with the deidentification conditions set forth in Sections 164.514 (a)-(b)1ii of the Health Insurance Portability and Accountability Act of 1996 Privacy Rule. No direct patient contact or primary collection of individual human patient data occurred. Study results were in tabular form and aggregate analyses, which omitted patient identification information. As such, the study did not require institutional review board review and approval or patient informed consent.
Acknowledgments
We are very grateful to Paranjoy Saharia, HEOR Scientific Services, IQVIA, and Rehan Ali, PhD and Benjamin North, PhD, Real World Solutions, IQVIA, for manuscript support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
OY and PL contributed equally.
Contributors Conception and design of the study and interpretation of the results: all authors. Data collection and analysis: OY, PL and BH. Original draft of the manuscript: PL. Critical revision and final review of the manuscript: all authors. PL acts as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors are employees of IQVIA.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.