Article Text

Statistics from Altmetric.com
Introduction
Burn-out, a state of mental exhaustion caused by one’s profession, is particularly acute among clinicians, especially in the USA.1–3 Oncology clinicians seem to be particularly affected.4–8 It is now acknowledged that use of electronic health record systems (EHRs), contributes to clinicians’ dissatisfaction and burn-out9–13 predominantly via the excessive requirements posed on clinicians for data entry.14 A recent special issue in the Journal of the American Medical Informatics Association included a number of papers that focused on quantitative measures of time spent on data entry and numbers of entries,15–18 all demonstrating that quantity of work is a key contributor to burn-out. In this perspective piece, we highlight and explain how there are additional mechanisms for EHRs to induce burn-out, such as the organisation of information on screen, and poor support for cognitive tasks.19 20 Specifically, EHR interface designs tend to fragment information,21 making it difficult to ‘get the full picture’ of a patient case, thus increasing the cognitive burden for tasks associated with clinical decision making.22 The lack of an effective display of a patient’s treatment as a whole may thus be one of the contributing factors of clinician burn-out.4 In our view, it is not only the quantity of EHR related work that leads to burn-out, but the quality of the work—the cognitive burden.
An exemplar case of the phenomenon of fragmentation of information about a patient treatment and the consequences for clinicians’ cognitive burden is provided by the design of EHR systems for cancer care, and more specifically the design of electronic oncology treatment regimens. These are linked, multidisciplinary, longitudinal records, not too dissimilar to electronic clinical pathways, linking preset tasks or orders over time.23–25 Systems of this kind are also used, for example, in stroke care.26 Electronic pathway functionalities are implemented across healthcare settings to standardise care and thus improve quality and safety, and are intended to support not only single clinical tasks, but a series of linked tasks by teams of clinicians managing a patient illness.23 Major integrated EHR systems such as EPIC27 or Cerner Millennium28 include functionalities of this kind, giving hospitals the possibility of linking orders along clinical guidelines. Given the longitudinal, interdependent and multidisciplinary aspect of the information involved, electronic pathways and electronic regimens pose challenges to the organisation of information and the design of information displays.
Clinical protocols and decision making in cancer care
Treatment regimens for most patients with cancer, especially in paediatrics, are complex. Medications are administered to patients over cycles, over months or years. At each cycle or dose, clinicians (re)assess the patient response to treatment and make decisions on whether and how to continue with the regimen. Medications are potentially toxic and clinical decisions involve high risk for the patient. The toxic effects of some medications manifest over a patient life-time, and result from the cumulation of multiple doses over time.
In travelling from the time of diagnosis to the end of treatment, clinical protocols provide a path, or a thread, for clinicians to follow (or deviate from). At each step, an assessment is made of both ‘where the patient is at’29 in the treatment journey—for example, how the patient is responding to treatment, how far along in the treatment they are—and how close or distant the patient treatment and trajectory are to the initial protocol path. As an oncologist in a children hospital explained to us, ‘…to synthesise a journey… at least two years, sometimes ten. … we need to maintain a thread of continuity, … not continuous together, but joined, so you can follow that particular thread… I want to see … what is the treatment the patient is getting today … in terms of where does it fall within the narrative of this patient’s treatment’.29
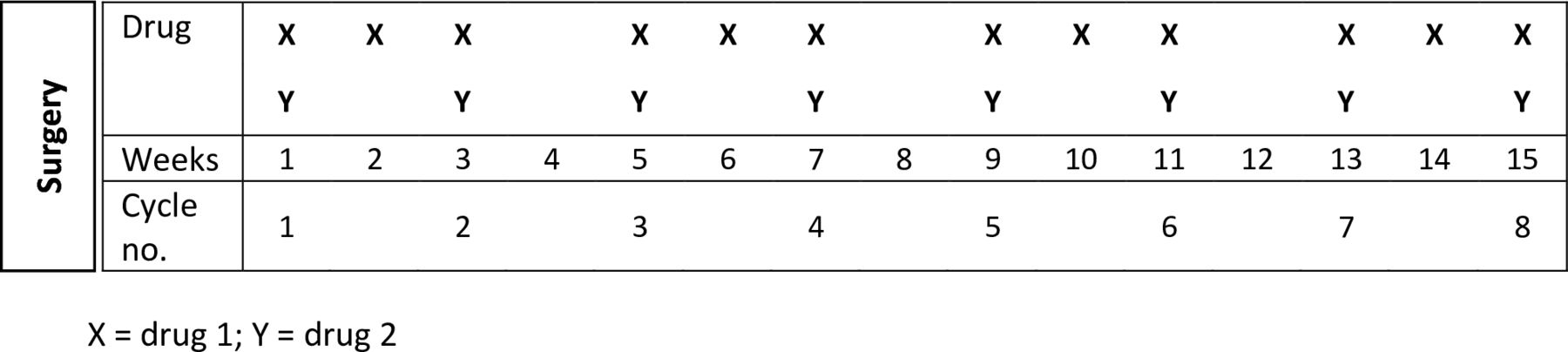
Traditionally, paper-based oncology protocols provide ‘roadmaps’ that summarise graphically the treatment over a period of time—tests, drugs and doses, distributed over a number of cycles (figure 1).
{kind=link}
Example of a chemotherapy protocol roadmap, simplified.
These paper-based versions of the roadmap can be printed and easily annotated with a patient’s actual treatment. Annotations show both what the protocol requires and any variations needed to address a patient response. For example, dose modifications, delayed doses or cycles.
From paper to electronic, from pattern recognition to computation
EHRs have been increasingly implemented and used in cancer care in the USA and other parts of the world. Their functionalities for linking orders, allow reproducing clinical protocols in electronic order sets. As human factors experts, we studied a recent implementation of an EHR for cancer care in Australia. We evaluated the implementation of one of these systems (a Cerner system) in a paediatric hospital,29 30 and carried out a (confidential) expert human factors review of a number of chemotherapy management systems for a commissioning body. In our research, we noticed how clinicians experienced difficulties with the electronic regimens’ information display, and in making sense of the patient treatment in relation to the relevant protocol. An oncologist told us, for example, how with the electronic record, ‘… it’s very hard to [see] that they haven’t got an extra dose at day 15 or they’ve missed a dose at day seven’.29 A junior physician made explicit the burn-out effect of the effort to recombine fragmented information of a patient’s history of treatment: ‘… to try and find a patient’s cumulative anthracyclines dose [in the electronic record]… [was] more exhausting than night shifts exhausting’.29
Electronic versions of the protocols ‘translate’ a treatment plan into a series of orders (events or tasks), arranged as lines of text, nested (partly visible) into cycles (aggregating lines of text). This creates a fragmentation of the regimen as a whole. Intended variations to the protocol are to be annotated in digital notes, only available when clicking on each cycle, and superseding other notes which the EHR automatically archives in the patient record. As we learnt in our research, the problem with this design is that since the notes ‘supersede each other’, any changes made to the treatment are difficult to identify and explain: ‘…someone would make a change 6 months ago to a particular dose of something, and you’d have no idea why and no idea when it happened’ (oncologist, paediatrics).29
To make sense of the information retrieved from each record, the clinician has to keep each data piece in memory and assemble a mental map of how they relate as a whole. This is a cognitive task known as ‘computation’.31
Paper-based roadmaps in oncology make immediately visible to clinicians ‘where the patient is at’ in the protocol as a whole and any deviations, easing navigation of a patient treatment. In this respect, the use of this tool is not unlike navigational tasks performed by operators in non health-related disciplines. It can be said of oncology roadmaps what has been said of US Navy ship charts32 that in roadmaps, every element of treatment (eg, a chemotherapy dose), has a specifiable ‘address’, and the relationships of all elements of treatment to the others ‘are implicitly represented’; they ‘introduce a perspective’ on the whole and on the position and ‘motion’ of the patient across the whole; ‘standing over a chart, one has a ‘bird’s eye’ view …’. Thus, ‘Having the chart […] makes this [navigation] task much easier. For example, […], displacement […] [off] track can be measured directly. The information regarding the next course is ready at hand and need only be read off the chart after the position has been plotted. […] the number of yards to the next turn [or the next dose] need not be measured; it is available by simple inspection’.32
Paper-based roadmaps support decision making through pattern recognition, while electronic protocols transform the task into computation. That is, with an EHR system, clinicians are required to compute the patient’s position on a treatment journey based on information visible across rows and screens, a cognitively demanding task, in a high-risk environment. This is the opposite of what human factors traditionally recommend for safe engineering of sociotechnical systems. For example, it is the opposite of what was reported in aeroplane cockpit design in the 1990s31 —instruments for landing were designed to transform pilots’ mental computation into pattern recognition, easing the landing task and reducing potential for errors.
While some have attempted the implementation of computerised roadmaps reproducing and enhancing the traditional paper versions,33 in our experience, EHR systems rarely provide a diagrammatic representation of encoded protocols akin to a roadmap. They provide detailed information about each cycle and dose, but this information is often fragmented; they document what has been ordered and administered to the patient, but not how close or distant from the protocol this was.
Here, we argue that the lack of effective displays of a complex treatment as a whole, in support of high risk decisions, may be one of the contributing factors of clinician burn-out in oncology.4 It is interesting to note that interventions targeting burn-out, even those targeted at the organisational rather than individual level, typically aim to enhance clinicians’ resilience—their capacity to sustain stress—through training, wellness monitoring or a reduction in working hours.2 3 6 Interventions rarely focus on improving EHR design. When EHR redesign is advocated for, it is usually in relation to alleviating the burden of clerical tasks,19 34 not improving system usability, nor converting mental computation into pattern recognition. Greater usability and less cognitive burden may be generated by incorporating functions into EHR which work on pattern recognition, rather than computation, resulting in reduced complexity, faster and less error-prone tasks, ultimately benefiting patient safety and reducing clinician burn-out. One recent example of this was an attempt to design a medication timeline for chronic disease patients, which resulted in improved physician performance on medication-related tasks when piloted.22 We recommend future work targeting clinician burn-out in oncology follow this path and focus on redesigning EHRs, using a human factors approach,35 to support complex navigation work. There is a need for research on how to design, and automatically generate, digital oncology roadmaps of a patient treatment in EHR. These roadmaps must be easy to navigate and must support pattern recognition. Research can also show whether and how lessons learnt from oncology are applicable to EHRs in other clinical contexts, where an overview of a patient’s trajectory, pathway or treatment journey is required.
Acknowledgments
We thank Bethany Van Dort (University of Sydney) for her assistance with figure 1.
References
Footnotes
Twitter @VLichtner
Contributors Both authors have contributed equally to this work.
Funding VL received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie-Skłodowska Curie grant agreement number 740 131.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.