Article Text

Abstract
Background Peer-to-peer health care is increasing, especially amongst people living with a long-term condition. How information is shared is, however, sometimes of concern to health care professionals.
Objective This study explored what information is being shared on health-related discussion boards and identified the approaches people used to signpost their peers to information.
Methods This study was conducted using a qualitative content analysis methodology to explore information shared on discussion boards for people living with diabetes. Whilst there is debate about the best ethical lens to view research carried out on data posted on online discussion boards, the researchers chose to adopt the stance of treating this type of information as “personal health text”, a specific type of research data in its own right.
Results Qualitative content analysis and basic descriptive statistics were used to analyse the selected posts. Two major themes were identified: ‘Information Sharing from Experience’ and ‘Signposting Other Sources of Information’.
Conclusions People were actively engaging in information sharing in online discussion forums, mainly through direct signposting. The quality of the information shared was important, with reasons for recommendations being given. Much of the information sharing was based on experience, which also brought in information from external sources such as health care professionals and other acknowledged experts in the field.
With the rise in peer-to-peer support networks, the nature of health knowledge and expertise needs to be redefined. People online are combining external information with their own personal experiences and sharing that for others to take and develop as they wish.
- diabetes
- eHealth
- information
- internet
- participatory health care
- self-care
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
The ubiquitous use of the Internet throughout society has had consequential implications in the field of health care. Statistics from the Pew Research Centre suggest that 87% of American adults use the Internet and 72% of those people use it to look for health information.1 ‘Peer-to-peer health care’ (defined as patients and caregivers sharing information with each other)2 has always existed at a community level, with people seeking health information from their family and friends. However, the emergence and functionality of the Internet has enabled this sphere of influence to extend beyond these traditional boundaries and has permitted these conversations to be both archived and to be extended to a wider audience.3 For many patients and caregivers, the Internet now represents a significant source of support and information.
In the early days of the World Wide Web, much research focused on how ‘safe’ the health information available was and despite repeated concerns, low levels of reported harm were found.4 With the growth in social media, research aims were shifted to examine how people were using Internet discussion boards5 with the finding that interaction with peers was important to individuals with a health condition.6, 7 Although value was placed on the knowledge that others living with the same condition could bring, people were also aware of the necessity of evaluating the information being shared.8 The recent work of Hamm et al.9 reinforced that social media was widely used by both patients and caregivers, with a variety of platforms and discussion boards being used to provide this support.
By 2011, 18% of Internet users were found to be seeking out people who might have similar health concerns to theirs.3 When this was focused upon people living with a long-term condition (LTC), this proportion increased with almost a quarter (23%) of individuals saying they use the Internet to seek out peers.3 In addition, sizeable numbers (26%) of Internet users have read other peoples’ experience of health or medical issues.3 Online discussion boards are supporting the public in this process of sharing their health experiences and nearly every condition has its own discussion board.10,11 Despite this move to patients not only using but also creating online information, much research in the field is still paternalistic. In 2009, it was noted that researchers ‘continue to view the role of health professionals as “providers and protectors”, able to control, or in some way “regulate” the types and amount of information that patients…should or could access’.12
There has, however, been very little exploration of the health information shared between people using discussion boards online and how users of these areas direct others to information sources that could be useful in supporting individual’s self-management strategies. This study took a qualitative approach to explore what information is being shared on these discussion boards and to identify the methods used to signpost their peers to information.
METHODS
This study was conducted by developing an approach that has previously been used to explore activity on online health discussion boards.13 Four active discussion boards for people living with diabetes were chosen for inclusion. These boards were deemed to be ‘active’ boards, as they had regularly had postings on the days preceding data collection. Diabetes was chosen as the condition of choice because of the number of active boards available to select the study cohort from. The focus of this study was not on diabetes specifically, but on the activities of people living with an LTC. The boards selected were all moderated by members of the community rather than by health care professionals. As focus of the study was peer-to-peer activities, it was felt that the presence of health care professionals had the potential to change people’s behaviours.
A snapshot approach was adopted for this study and posts between 1 April 2014 and 7 April 2014 were included. Threads and responses to posts on these threads that the researchers deemed to contain relevant data (see the inclusion/exclusion criteria below) were copied verbatim from the boards into Microsoft Word by a member of the research team (OHA).
Whilst there is debate about the right ethical lens to view research carried out on data posted on online discussion boards, the researchers chose to adopt the stance proposed by Bond et al.14 of treating this type of information as “personal health text”, a specific type of research data in its own right. Ethical approval for this study was granted by Bournemouth University, England.
Inclusion/exclusion criteria
Posts from each of the four boards were included if:
- The initial post was dated between 1 April 2014 and 7 April 2014 (the collection week);
- They were discussing information related to self-management of diabetes, including (but not limited to) health, medication, living with diabetes condition, the social effects of diabetesand diabetes-related equipment.
In some instances, the responses of these threads continued beyond the collection week, in which case all of the threads that started in the collection week were included.
Posts were excluded if:
- They were deemed to be sharing personal information not related to health care (e.g. ‘my dog had to go to the vet today’);
- The post date was within the collection week but they were associated with threads started before the collection week;
- They were generic posts sent by moderators to all new posters when they introduced themselves;
- They were related to prediabetes, gestational diabetes, soapboax/success stories, events and fundraising, child/teen and parental issues in diabetes, driving, off topic, other health conditions and diabetes, and mind, body and spirit.
Data analysis
Qualitative content analysis, a recognised method for analysing information of this nature15 and basic descriptive statistics were used to analyse the data. Data were evaluated manually rather than electronically by both members of the research team (CSB and OHA), because of the frequent use of abbreviations and “web speak” on these discussion boards. Inductive analysis was used, with each posting coded according to its meaning. Following the attributing of codes to the postings, those posts with similar codes were combined into subcategories and categories were derived from this. Both researchers verified a sample (N = 5) of the other’s postings to ensure consistency. The depth of analysis was further consolidated by the researchers comparing codes and categories to provide an additional perspective and ensure that nothing was missed. Any differences in coding were discussed between the researchers and agreement reached.
Where appropriate, quotes were extracted to support categories. In keeping with the recommendation from previous research about protocols when presenting ‘personal health text’,14 these quotes are presented as ‘aggregated quotations’ to preserve anonymity. These quotes were initially aggregated by CSB, using two or three original quotes to produce each aggregated quote. These aggregated quotes were then verified by OHA to confirm that they accurately reflected the essence of the original authors.
RESULTS
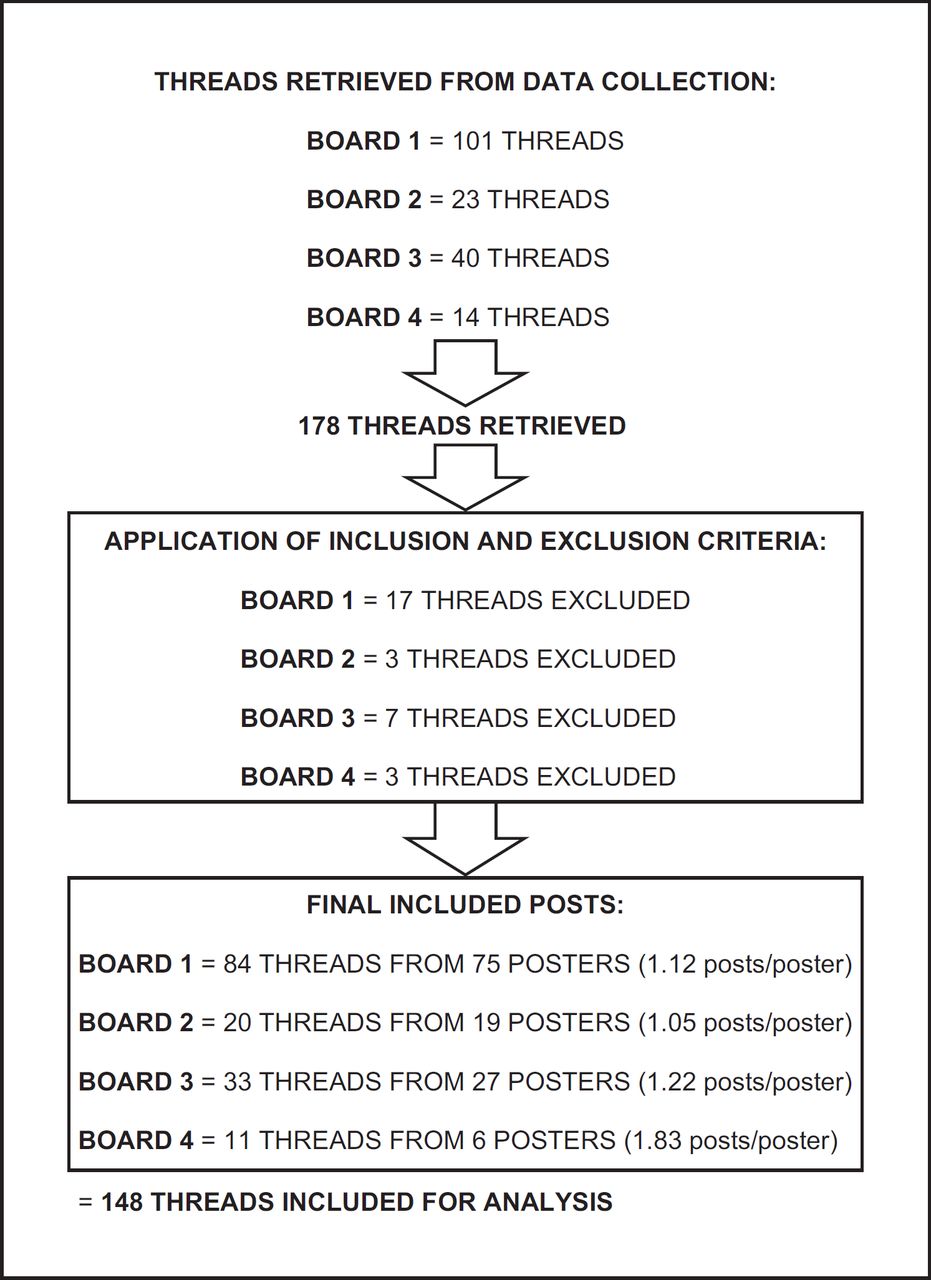
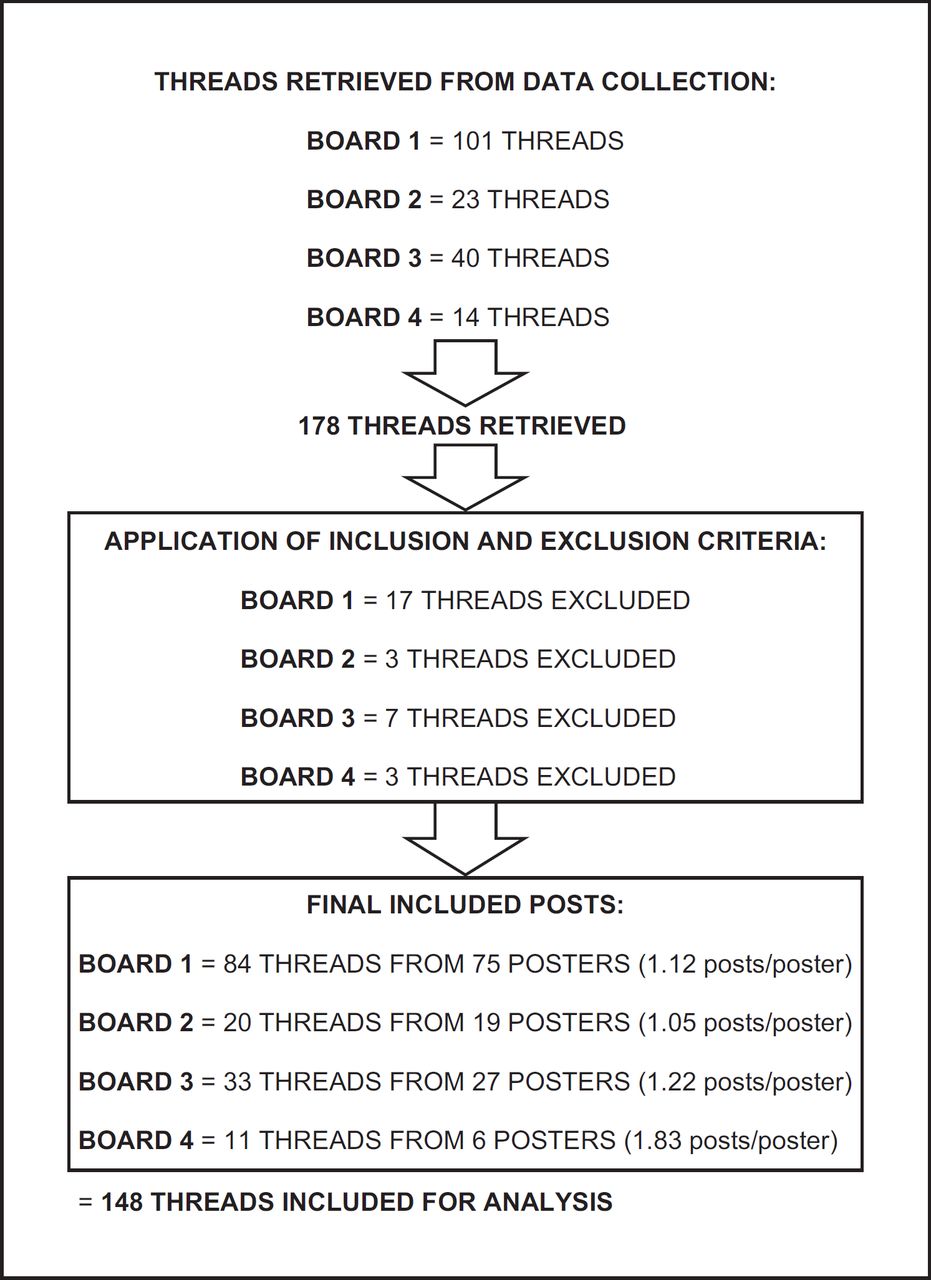
From the four boards identified, 178 threads were retrieved for analysis (see Figure 1). Following screening of these threads by one of the research teams (OHA), 30 threads were excluded resulting in 148 threads eligible for analysis. Figure 1 highlights the number of unique posters per board, with the average number of posts per poster ranging from 1.05 (Board #2) to 1.83 (Board #4).
{kind=link}
The themes identified fell into two major themes: ‘sharing information from experience’ and ‘signposting other sources of information’. The application of themes was not exclusive, with some threads containing multiple subthemes. The example post in the quote below shows subthemes of ‘diagnosis’, ‘nutrition and dietary’ and ‘referral to an external website’:
‘Other health conditions, or just not sleeping well, can cause tiredness as well, so it might not be the diabetes, however sorting out the diet might also help. When I eat breakfast plain greek yogurt can be perked up with cinnamon. Have a look at [web address] it’s very helpful’
The type of information shared is shown in Table 1. From the 148 included threads, 234 were allocated to themes in total (an average of 1.58 themes per post). In our study, 127 people contributed in total and individual discussions had an average of 1.31 contributions per thread.
‘Your mileage may vary’ is a term used to mean that diabetes affects everyone differently and what works for one individual (e.g. an insulin regime) may not work for another and may not even work for the same person if circumstances change.
In presenting these results, the method of using compound quotes10 has been adopted to ensure that the anonymity of posters has been protected.
Sharing information from experience
Nutritional and dietary
Sharing information about dietary approaches that had been successful in response to peoples’ posts about their problems was a common feature:
‘I have mainly protein for breakfast (boiled egg for example) you could see if that helps you at all’
Other people shared suggestions for making living with diabetes more fun:
‘If you like chocolate sponge then try just having a spoonful as a treat’
Diagnosis
Information shared about diagnosis included sharing what had first made people think they might have a problem and the details of the diagnosis:
‘I had some abscesses and was getting tired all the time, was a bit worried so went to the pharmacy for a blood test’
‘You could be a LADA / T1.5 you need to get your GP to check your anti-GAD levels, don’t let them make assumptions that your type 2’
Self-management
The importance of testing and tips on how to work effectively with blood glucose readings to promote effective self-management was emphasised by many posters:
‘A blood glucose monitor is essential. They’re generally pretty accurate and give a good indication of how foods affect your levels’
‘I check my blood before meals and 4 hours after having my meal as well as the 2 hours after that the DNS says’
Advice about unexpected readings and potential causes were also frequently shared:
‘Compare readings and double check if a single reading looks way off what you expected it to be’
‘My levels always shoot up if I’ve picked up a bug’
Health care interactions
Information about dealing with HCPs included the right HCP to see and dealing with problems in the patient/HCP relationship:
‘It could be a cataract, I really think you should go and see your optician’
‘I’ve always been happy with the nurses I’ve seen, but if you’re not happy you should ask to see a different one, it’s so important to have one you get on with’
The need to understanding the information given and question advice was also discussed:
‘Your reading of x.x is under the level the current guidelines recommend statins should be started at so I really don’t think you need them’
‘The nurse was quite anti my plans to try a low carb diet, but I think it would work for me, any tips on how to handle it with her?’
Medication
Information was shared about different types of medication available, possible side effects and future possibilities:
‘Metformin’s good, and Gliclazide may also help a bit but I expect you will need to add insulin to them over the coming years’
‘I’m not really coping very well. Like many people I was put on Metformin, but its given me a load of problems and I am struggling a bit with the side effects, I know other people on it say they’ve had the same problems’
Living with diabetes
People shared various experiences about living with diabetes, including acceptance and integrating it into their lives:
‘I know my sugars are affected by stress, so I try to make positive changes to my lifestyle to help’
‘I’m getting to know if my sugars are too low or to too high just by how I feel. We all have off days and just have to get on with them in the best way we can’
Signposting other information
One way of sharing information was to recommend other resources. The types of information signposted were varied and included links to detailed explanations of diagnostic tests, medication information, research papers, online shops where test strips could be bought for people not supplied by their health care system and advice about low carbohydrate diets. Most links were to external websites; however, links within the same forum (or its hosting website), YouTube, blogs and apps were also shared.
Most referrals included some information about why the resource was being suggested:
‘There is a video on YouTube by a Dr XX - A Canadian doctor with late onset T1, who’s a very active exerciser, you might find his tips about keeping insulin use to a minimum useful (YOUTUBE video link)’
‘This gives very complete explanation of [the medicine] it includes the side effects as well as the benefits [website link]’
‘This site has lots of good information, but for information about blood sugars I recommend Blood Sugar 101, its easy to use, you can find all the essential information from the front page’
QUALITY
Most information shared was non-judgemental, with some posters using an accepted phrase on such forums of ‘your mileage may vary’ (meaning that what works for one individual may not work for another). Some posters also emphasised that they were not doctors and therefore could not offer medical advice. Others agreed (or disagreed) with previous posts in the thread:
‘I second the suggestions of substituting almonds for chocolate. They also release energy more slowly so it’s less likely that you’ll spike then dive’
Whilst some posters did signpost research papers, the problem that this research was not free to access was acknowledged. The lack of consensus amongst researchers was also raised:
‘If you look you can find research that shows low carb diets are a disaster, but you can also find an equally long list that suggests they’re fine. You need to looks at different sources, and ask questions of the information you find’
DISCUSSION
Even with a medical condition as common as diabetes, traditional family and community support networks are unlikely to provide an individual with many peers who have similar experiences. Those individuals that do have these support networks may well share the same health care professionals as those in their networks, thus limiting the range of professional resources and opinions to draw upon. In contrast, the Internet opens up similar networks that have a global reach, bringing a breadth of experiences and resources to the access of an individual with diabetes.
The type of expertise that ‘patients’ can have has been discussed in the context of the ‘Expert Patient programme’, initially developed in the USA and rolled out in the UK at the start of this millennium.16 The UK Department of Health (2001) identifies the expertise and knowledge attributed to patients and professionals (Table 2), with health care professionals expected to have responsibility for the ‘medical’ management of the condition and patients for the ‘social’ aspects of living with a chronic condition. This study has reinforced these areas of expertise and knowledge from the patient’s perspective, as they were shown to be cognisant in all of the areas highlighted in Table 2.
As shown in Table 1, the type of information shared by posters in this study was split evenly between information about effectively living with diabetes and the management of the condition (including medicines and the relationship with health care professionals). This is in keeping with the work of Quinn et al.,17 who found a similar pattern in a study analysing posts made by people living with common cancers. In their study, over half (52.4%) of posts were medical in nature; however, these authors categorised online interaction by the topic of the post rather than classifying the nature of the interaction.
The use of ‘networked collaborative filtering processes’ or aggregators (e.g. RSS readers) was found to be a useful technology in 2008;18 however, the people in our study were not making use of these aggregating-style services. Posters generally responded to other posters, signposting them directly towards information on other websites, or other areas of the forum site that they thought would be useful. Smartphone apps for diabetes have been the subject of attention in the scientific literature,19–21 and so it could have been expected that more than just the one user in this study would highlight these as a source of information. Although smartphone apps for diabetes are valuable for self-tracking, it may be that at present they are not viewed as information sources in their own right for individuals with diabetes.
Of relevance to this study is recent work,22 which explored how a new and controversial topic was discussed on a forum for people living with multiple sclerosis. This focused on posters who had shared a minimum of five hyperlinks, and the findings were that the majority of links were to social media platforms including YouTube, Facebook and blogs. This contrasts with the findings of the present study, where the most common links were to other areas of the same site or external websites. Some websites in our study were similar in nature to blogs however and were produced by a single person with experience of diabetes, rather than a professional website (for example WebMD).
A further finding of this study was that reference to evidence-based research information was infrequently seen (mirroring the finding of Sudau et al.),22 although some posters and the websites that they signposted did promote an evidence-based approach. Other posters in our study, whilst not signposting research-based information, shared information gleaned from their own health care professionals. This enabled them to collate and disseminate a unique combination of experience and medical knowledge. This is similar to the findings of a study by Schaffer and colleagues,23 who explored mothers of children with genetic conditions, and found that they used the Internet (especially peer-to-peer resources) and ‘sought out biomedical knowledge that they interpreted through the lens of their own child’s experiences’.
The authors wish to acknowledge several limitations of this study. The insights and themes that were identified were specific to diabetes only, and potentially differing patterns towards information sharing may have emerged if discussion boards on alternative conditions were explored. The limited time frame used provided a snapshot of discussions that were occurring on the discussion boards, but this may have varied if a longer/shorter window of data collection was employed. In addition, the types of information sharing witnessed in this study were specific to discussion boards where there was no limit on the numbers of characters used (unlike Twitter) and where textual data was the focus. Analysis into other methods of patient interactions (e.g. through Facebook, Instagram or other social media) may have yielded alternative results to those in this study. Future research should consider utilising other platforms used by patients to discuss health conditions (e.g. Twitter and Facebook) and exploring a wider range of conditions.
CONCLUSIONS
People living with diabetes are actively engaging in peer-to-peer health care through their information sharing activities. This is mainly through direct signposting to information. The use of aggregators did not feature as a method adopted.
The quality of the information shared was important for posters, many offering some accompanying reason for their recommendation. Whilst there was limited direct sharing of research-based information, much of the information sharing from experience brought in information from external sources such as health care professionals and other acknowledged experts in the field.
With the rise in peer-to-peer support networks, the nature of health knowledge and expertise needs to be redefined. People that inhabit these online domains are using information in ways that academics, researchers and health care professionals cannot, by combining this information with their own personal experiences and sharing that for others to take and develop as they wish.
References
Footnotes
CONFLICTS OF INTEREST Neither of the authors on this paper (CSB and OHA) reports any conflict of interest.