Article Text

Abstract
Background A critical need exists for effective electronic tools that facilitate multidisciplinary care for complex patients in patient-centered medical homes.
Objective To identify the essential components of a primary care (PC) based electronic care plan (ECP) tool that facilitates coordination of care for complex patients.
Methods Three focus groups and nine semi-structured interviews were conducted at an academic PC practice in order to identify the ideal components of an ECP.
Results Critical components of an ECP identified included: 1) patient background information, including patient demographics, care team member designation and key patient contacts, 2) user- and patient-centric task management functionalities, 3) a summary of a patient’s care needs linked to the responsible member of the care team and 4) integration with the electronic medical record. We then designed an ECP mockup incorporating these components.
Conclusion Our investigation identified key principles that healthcare software developers can integrate into PC and patient-centered ECP tools.
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Effective coordination of patient care by a multidisciplinary team is a key goal of the patient-centered medical home (PCMH).1 Care coordination is particularly important for complex patients, or those with multiple comorbidities and social support needs. However, care coordination is often hampered by disjointed communication and lack of a supportive documentation infrastructure. Care planning has been proposed as a solution for improving team-based care of complex patients. An effective ECP provides an overarching blueprint centered around a patient’s needs, improves coordination among the different team members (TMs) caring for a patient, establishes task accountability and supports selfmanagement goals.2,3
Despite recognition of care planning’s potential, information technology (IT) tools that effectively facilitate this process are not regularly available within current PC IT systems. Additionally, although small studies have demonstrated the benefit of EMR-based ECP tools,4 in practice, ECPs are not typically used in the ambulatory setting and significant ambiguity exists regarding what constitutes care planning.3 Where longitudinal ECPs exist, they are often not standardized or interdisciplinary in nature and are variably found in electronic format.5 And while care planning and coordination are of significant interest to commercial vendors, commercial tools are more commonly used for data aggregation and identification of high-risk populations and overdue interventions rather than for workflow coordination or communication enhancement capabilities.6
In order to be effective, IT tools should be designed to fit the needs of on-the-ground users. We thus conducted a qualitative study to identify the characteristics of a tool that would facilitate electronic, team-based care planning for medically and socially complex patients.
Methods
Our qualitative study consisted of three focus groups followed by nine semi-structured interviews. These were conducted at the Jen Center for Primary Care, an academic internal medicine practice at Brigham and Women’s Hospital that provides care to 19,000 patients. One-third of its diverse population derives from the hospital’s underserved urban surroundings, a similar fraction receives public insurance and 13% is non-English speaking. Six thousand of the practice’s patients have diabetes and many suffer from multiple chronic diseases. 20% of the Jen Center’s patients are over the age of 65.
The Jen Center, which recently transitioned to team-based care, employs 42 faculty physicians and 64 residents. Its 57 other staff members consist of nurse practitioners (NPs), physician assistants, registered nurses, pharmacist technicians, licensed practical nurses (LPNs), medical assistants (MAs), secretaries, social workers (SWs), pharmacists and care coordination nurses. Our study was exempt from Institutional Review Board approval due to its quality improvement focus.
Focus groups consisted of 17 self-selected staff members (two SWs, two primary care physicians (PCPs), two secretaries, five nurses, a pharmacist technician, an NP, a practice manager, a resident, an LPN and an MA) who met three times for one hour over the course of six months. Focus groups garnered staff opinions about the general scope and appearance of an ECP, key team-based care components of an ECP, and potential ECP features of interest. They were led by author CW. A preliminary ECP mock-up was designed based on themes derived from focus groups.
Individual, semi-structured, 18-question interviews were subsequently conducted with nine TMs (three nurses, a resident, two SWs, a PCP, a pharmacist, and a secretary). All interviewees were uncompensated volunteers who were ensured of confidentiality and given an opportunity to decline participation without repercussion. Six had participated in focus groups. In addition to being asked to describe potential benefits and drawbacks of an ECP, participants were asked to prioritize several specific ECP features on a 1–5 scale, detail additional useful ECP components, and to provide feedback on the ECP mock-up.
Deidentified data from focus groups and interviews were electronically transcribed by authors ST and LR. Data were explored via content analysis. ST reviewed interview transcripts to code commonly mentioned phrases and preference patterns. Codes were transformed into themes that identified key components of an ECP; themes were revised as additional data became available. LR independently reviewed the coding process and analyses were compared for discrepancies.
We subsequently iterated and finalized the ECP mockup based on interview findings.
Results
Focus groups
The three focus groups conducted over six months helped identify components of team-based care that an ECP could facilitate, how an ECP interface should broadly look, potential ECP features of interest and how an ECP might fit into existing workflows and electronic systems. ST and LR translated a rough sketch of an ECP generated from focus groups into graphical software.
Semi-structured interviews
Semi-structured, individual interviews revealed that TMs prioritized an ECP’s ability to:
Provide a real-time summary of a patient’s comprehensive care needs and responsible TMs. This could not only include medical needs such as diabetes and hypertension but also social issues such as food insecurity and substance abuse. TMs wanted to see designated point people for each task, i.e. which endocrinologist, NP and PCP were collaborating on a patient’s diabetes and which SW was responsible for connecting them with food assistance.
Display a patient’s most pertinent background information. TMs emphasized that it was critical for ECPs to display: a patient’s care team, addresses, day program, best contact, visiting nurse, healthcare proxy/guardian, PCP, living situation, disability, insurance information and interpreter needs. A brief paragraph detailing patients’ support systems, how their work affects their health and other information not readily obvious from structured EMR entries could also be included here.
Facilitate task assignment and referrals among TMs. This feature would allow tasks under each area of need to be specifically delegated to a care TM, with targeted notifications arising from each assignment made.
Help keep track of tasks, both by user and patient. TMs requested that the ECP interface be able to 1) generate individualized lists that displayed each TM’s tasks for all of their patients with ECPs and 2) display all outstanding tasks for individual patients.
Minimize duplicative work or documentation. Information entered in other parts of the EMR or in alternate electronic systems should be drawn into the ECP, so as to reduce reentry time.
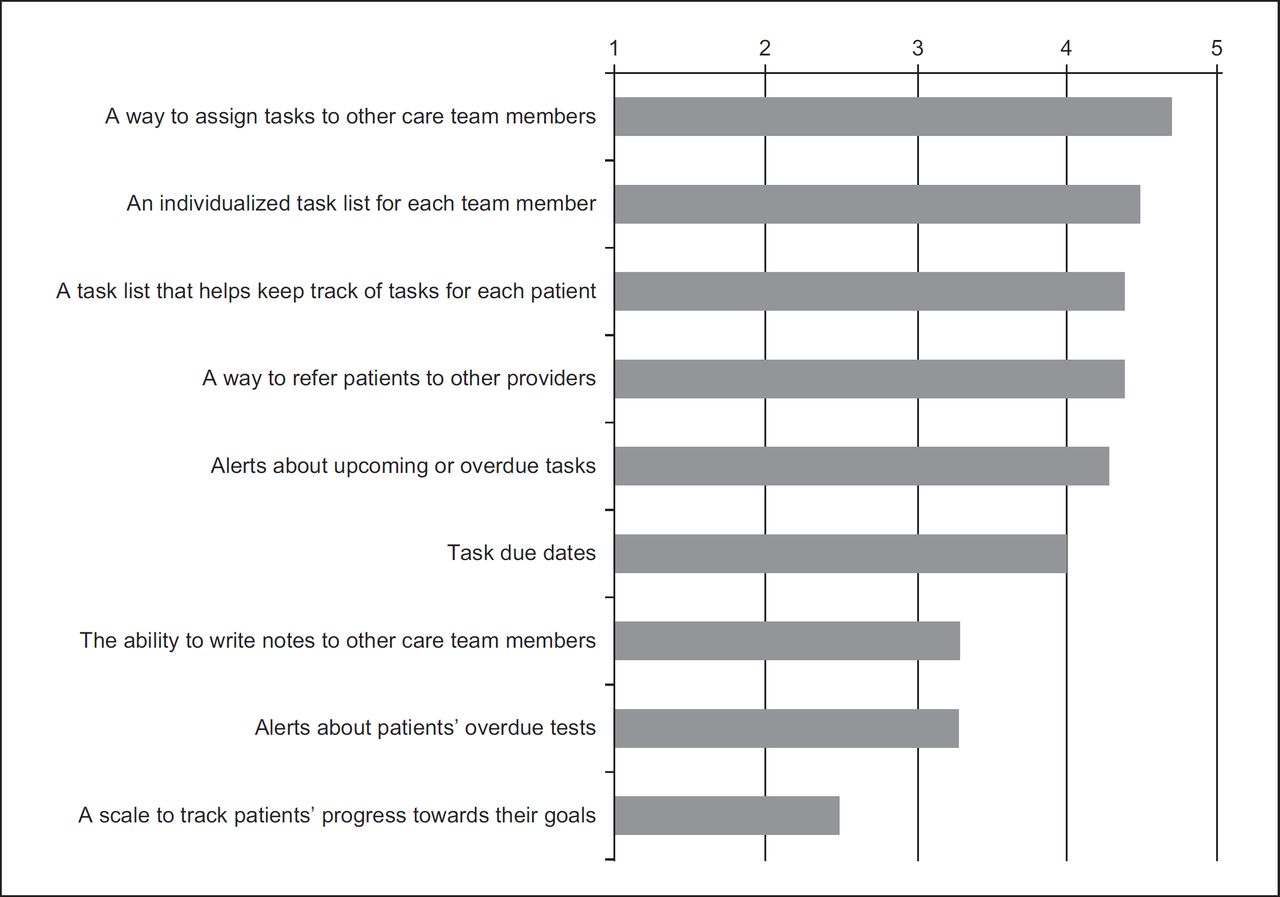
Figure 1 depicts TM’s ratings of the importance of several ECP components that were introduced via focus groups but whose relative priority was clarified during interviews.

TMs also preferred that the ECP have: 1) collapsible headings so they could deal only with sections relevant to them; 2) autopopulated goals for common diseases with the ability to add custom goals; 3) information autopopulated from the EMR, such as demographics and labs; 4) an archived history of completed goals and tasks; 5) a tally of how many times a patient had not showed for an appointment and been to the ER within the last six months and year and 6) prompts for pending and upcoming tasks.
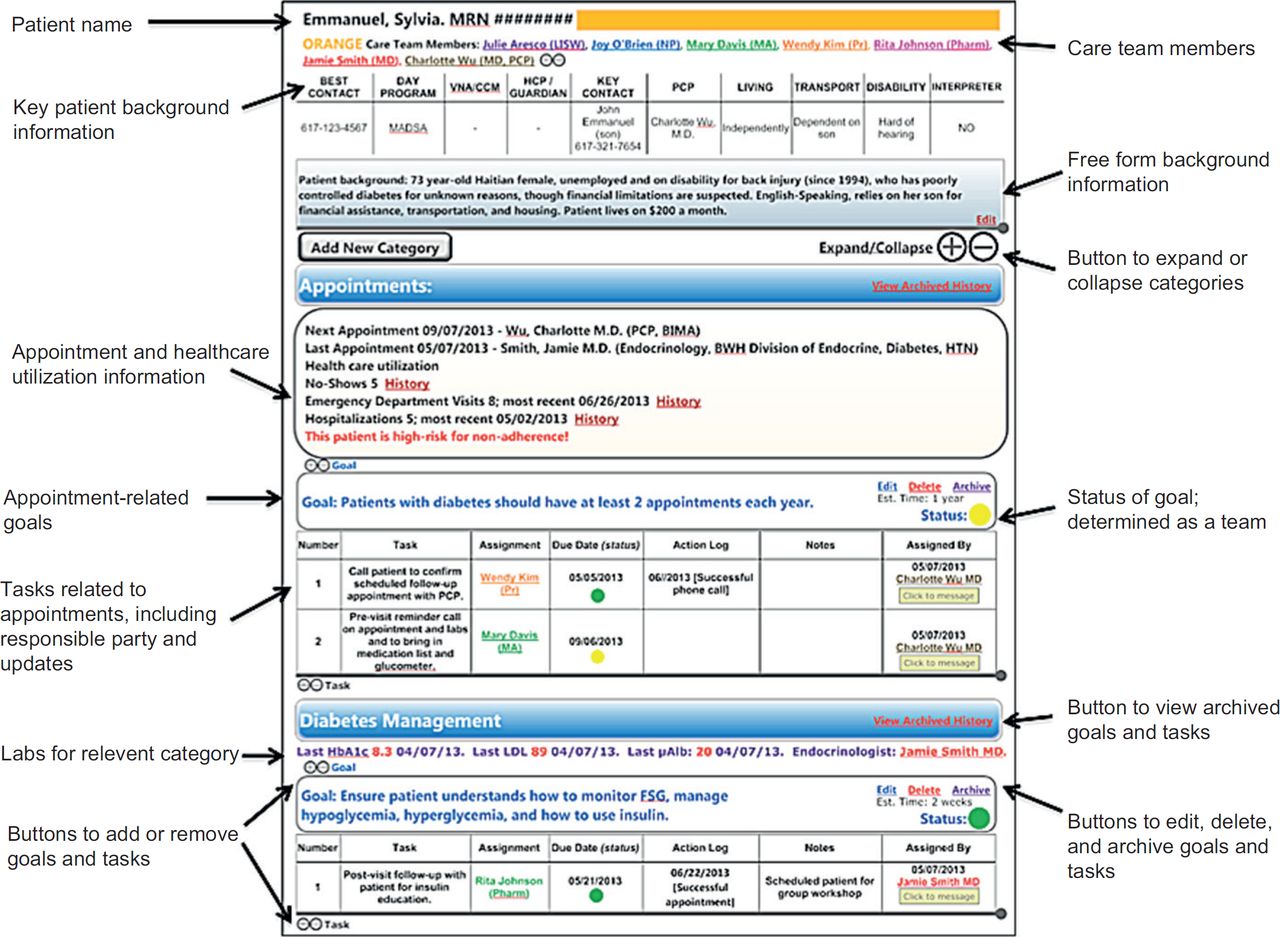
Figure 2 depicts a mockup of an ECP interface with the aforementioned components incorporated. Initially generated after focus group completion, this mockup’s design was iteratively modified as TMs provided feedback on the interface and detailed feature priorities emerged during interviews.
{kind=link}
{kind=link}
TMs predicted that an ECP would provide a standardized form of communication around a shared patient and facilitate increased transparency. It would help facilitate team-work by clarifying others’ roles and responsibilities, create accountability around referrals, reduce duplication of work and enhance intra-team communication. They also expected decreased time spent searching for patient information. Interviewees expressed hesitance about lack of clarity around who was accountable for managing and updating the ECP and about potential duplication of documentation and workflows.
Discussion
In a qualitative study, we identified core requirements for a novel PC-focused ECP tool. Our proposed interface, shown in Figure 2, helps define a patient’s care team and facilitates access to background information about shared, complex patients. The identified design components have the potential to engage all TMs while facilitating shared clinical goals for a patient, effective task assignment, and accountability.
Our findings have wide applicability in the PC, chronic disease and health IT realms. Despite the centrality of multidisciplinary, coordinated care for complex patients in the PCMH, no currently available electronic tools effectively facilitate this goal. Moreover, ambiguity exists regarding the format of an optimal ECP tool.3 By identifying criteria for an ECP tool aimed specifically at teams taking care of complex patients, we have laid the groundwork for PCMHs and healthcare IT developers to design targeted ECPs or build upon existing products without the burden of an extensive exploratory phase. We have also identified key issues to consider in ECP implementation, including the importance of clarifying ECP task accountability, avoiding duplication of work and integrating ECPs into EMRs that are part of daily workflows.
Our study’s strengths include the multidisciplinary nature of our qualitative analysis, our derivation of quantitative information about ECP feature preferences and our study of a clinic with complicated workflows. Limitations include the relatively small interview sample size, lack of patient input into the tool’s design and our focus on one academic, urban clinic. Next steps include translating the ECP into an EMR via collaboration with institutional health IT developers, testing its use longitudinally and engaging patients with the tool.
Overall, we have successfully identified core design principles for an ECP through qualitative end-user interviews. Integration of the features identified into next-generation electronic tools can help achieve the care coordination that is central to 21st century accountable care and the PCMH.