Article Text

Abstract
Background Ankylosing spondylitis (AS) is a chronic inflammatory condition characterised by spinal arthritis and exercise is often recommended to reduce the symptoms and improve mobility. However, very little evidence exists for the value of exercise in AS.
Objectives Firstly, this pilot study aimed to evaluate an eHealth tool, the AS Observer, specifically designed to monitor symptoms, quality of life and physical activity in AS, in terms of patient experience and suitability in generating data for epidemiological studies. Secondly, it also investigated the collected data to determine if physical activity benefited individuals with AS.
Methods The AS Observer was designed to enable weekly monitoring of AS symptoms and exercise using a web based platform. Participants with AS (n = 223) were recruited to use the AS observer. They provided baseline data and completed online weekly data entry for 12 weeks (e.g. Bath Ankylosing Spondylitis Activity Index (BASDAI), howRu, International Physical Activity Questionnaire (IPAQ)). Panel data analysis with fixed effects models investigated associations between variables. Activity type data and exit questionnaires were subjected to qualitative thematic analysis.
Results In general, the AS Observer was well received and considered useful by participants, with 66% providing a positive response. The collected data suggested that IPAQ is inversely associated with total BASDAI, stiffness, tenderness and pain, but not fatigue. Stratified analysis demonstrated differential associations between BASDAI, IPAQ and howRU based on sex, HLA-B27 status and disease duration. Approximately half of the participants frequently did therapy and three-quarters undertook at least some vigorous activity ranging from formal exercise to recreation and (house) work. Despite some technical challenges, tool evaluation suggested that the AS Observer was a useful self-monitoring tool for participants.
Conclusion This pilot study demonstrated that increased exercise intensity and duration were associated with an improved BASDAI symptom score in a cohort of participants with AS. Furthermore, it provided further evidence of the value of using eHealth tools for clinical purposes and data collection for research, inclusive of the development of treatment pathways and disease management strategies.
- Ankylosing spondylitis
- AS Observer
- BASDAI
- eHealth tool
- physical activity
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS), which is the prototype of the seronegative spondyloarthropies, is an inflammatory condition characterised by spinal arthritis and associated conditions such as uveitits and Crohn’s disease.1 The prevalence of AS is reported as 0.24% in Europe2 and 0.27% in the UK. AS is a chronic inflammatory condition with a heavy burden of disease3 that includes sacroiliitis, spinal fusion, peripheral arthritis and a range of extra-articular manifestations,4 ultimately leading to impacts upon mobility, societal functioning, mental health and elevated mortality.5 Understanding of AS aetiology and pathogenesis is still limited. However, hereditary polygenic characteristics have been recognised, most notably the association with Human Leukocyte Antigen gene (HLA-B27),6 which is often used within diagnosis criteria.7
Exercise and physiotherapy are commonly used in managing AS to maintain spinal mobility, reduce pain and support mental health. Studies have shown a positive correlation between the amount of exercise and improvement of symptoms, spinal movement, flexibility and strength during individual and supervised exercise programmes (including physiotherapy) for a duration of between two and six months.8,9 However, a recent systematic review undertaken to support recommendations for the management of AS noted that despite these positive findings ‘the small numbers of participants, the heterogeneity of the interventions and outcome measures, and deficiency in reporting data result in wide intervals and lack of strong evidence’, 10 eHealth, which is the use of information and communication technologies to investigate health, may provide solutions to address concerns raised by the systematic review. Mobile phone applications and websites are increasingly being utilised to allow patients to monitor their condition and other aspects of their lives on a daily basis, thus generating large longitudinal datasets for analysis and therefore improving our understanding of particular conditions. The availability of self-assessment technology is increasing and as eHealth accessibility is improving, prevention, treatment and health maintenance is becoming personalised and patient tailored.11 Studies show that there has been an upward trend in using the internet for health-related purposes12 and that small studies with a direct focus improve the efficacy and accuracy of clinical support for long-term conditions.13
This pilot study aimed to determine whether the AS Observer (https://asobserver.wordpress.com/home/), a specially developed online tool, was suitable to monitor the symptoms, health-related quality of life and physical activity of participants with AS. The study also utilised the data collected to investigate whether physical activity influenced the symptoms and quality of life of individuals with AS.
Methods
The online AS Observer tool, a web-based participant engagement interface, was developed in collaboration with myClinicalOutcomes Ltd (mCO; http://www.myclinicaloutcomes.com). The mCO system is designed to support real-life clinical workflows by collecting core clinical metrics at timely intervals along the diagnosis and treatment pathway, displaying this data on tailored patient and clinician interfaces.14 This was modified to produce the AS Observer module, with the clinician interface replaced with a researcher dashboard enabling the research team to login and investigate some basic summary statistics during the 12-week data collection phase.
Participants meeting the inclusion criteria (aged 18+, diagnosed with AS, U.K. resident and with computer access) were invited to participate via email (with assistance from the National Ankylosing Spondylitis Society; NASS) and social media (e.g. AS forums). They were directed to the project website (https://asobserver.wordpress.com/home/) where information on project goals, ethical information and how to participate was available.
Registration and baseline data
At registration, consenting participants were allocated a unique identifier code and baseline data (e.g. sex, date of birth, year of diagnosis, body mass index (BMI), smoking status (never, former and current), disease severity proxies (i.e. HLA-B27 status, frequency of attendance at rheumatology clinic and current medications) and comorbidities (using Department of Health standardised question set) were collected15 using the patient interface of the mCO system (Figure 1).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Weekly question set
Data was collected for 12 weeks from 15 September to 7 December 2014. Weekly email reminders were sent to participants requesting them to fill out three assessments on the patient interface. These assessments included the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) as a measure of current disease activity (Figure 2),16 healthrelated quality of life was monitored via howRu (http://www.r-outcomes.com; four components: pain or discomfort, feeling low or worried, limited in what you can do and require help from others) and physical activity via the validated short form of the International Physical Activity Questionnaire (IPAQ; http://www.ipaq.ki.se/ipaq.htm), which assesses physical activity frequency, intensity and duration. The howRu questions have better readability statistics and a similar overall performance when based on a single point in time compared with the longer SF1217 and EQ-5D.18 Additionally, an open text question was added to the IPAQ to capture the different activity types patients were undertaking.
Total Metabolic Equivalent of Task (MET) minutes of exercise per week variable (which was subsequently log transformed) and IPAQ categories (low, moderate or high intensity exercise) were calculated following the IPAQ scoring protocols. 19 A binary vigorous activity variable was also derived looking at participants who had done more than 1 hour of vigorous activity per week.20
Tool evaluation
To facilitate evaluation of the eHealth tool any comments on the website or contact with the help desk were recorded. Additionally, all participants including those withdrawing before the end of the study received a set of exit questions to ascertain the validity and usability of the AS observer (Table S1). The answers to these questions were investigated using qualitative techniques. Coding frameworks were developed by utilising thematic analysis with an inductive content analysis approach on manifest content. This consisted of rounds of data familiarisation, open coding, theme construction, abstraction and interpretation21 and allowed identification of similarities in data and the development of thematic patterns.22 Where appropriate, counts were performed on the number of participants whose responses aligned with each code.
Statistical analysis – physical activity and AS
All statistical analysis utilised a panel data analysis approach and the ‘xt’ suite of functions in Stata V13.1. Descriptive statistics were generated for demographic characteristics of participants. Associations between categorical demographic characteristics and total mean BASDAI score (0–10) were ascertained using regression analyses. Fixed effect (FE) regression models investigated associations between BASDAI (and its individual components, i.e. fatigue, pain, stiffness and tenderness) and physical activity measures (IPAQ – continuous and categorical, 1 hour of vigorous activity). The FE models reduce bias by removing the effect of time invariant variables (e.g. demographics). Regression models were therefore only adjusted for confounding variables that altered weekly (e.g. howRu, physical activity or BASDAI). The association between howRu and total BASDAI or physical activity were assessed using FE regression models.
Stratified analyses were performed on sex, HLA-B27 status and disease duration (0–10; 11+ years). Following qualitative analysis of activity type, some stratified analyses were performed investigating a number of themes including gardening, team sports and housework.
A sensitivity analysis was also performed investigating associations only in participants that had completed at least 6 weeks of data.
RESULTS AND DISCUSSION
In this pilot study, 223 individuals were recruited and on average this cohort was 50 years old, which had been diagnosed 17 years ago, and of those who knew their HLA-B27 status 81% were positive (Table 1). At least half of participants could be considered to have active AS requiring management (52% attended a clinic at least twice a year and 38% were using anti-TNFα therapies). The majority of participants had comorbidities (75%), including chronic back pain, sciatica or osteoporosis (45%), cardiovascular problems (43%) and stomach or bowel problems (40%). The mean BASDAI, howRu score and IPAQ MET minutes reported over the 12-week period are summarised in Table 1.
Associations between demographic characteristics and BASDAI (Table 2) were generally as expected, with significantly elevated BASDAI scores observed in those with higher BMIs and those with more frequent rheumatology clinic visits or high numbers of comorbidities.23 Medication use did not correlate with levels of disease activity, except for patients using steroids who had the highest mean BASDAI (5.20 ± 2.15).
Physical activity, BASDAI and mental health
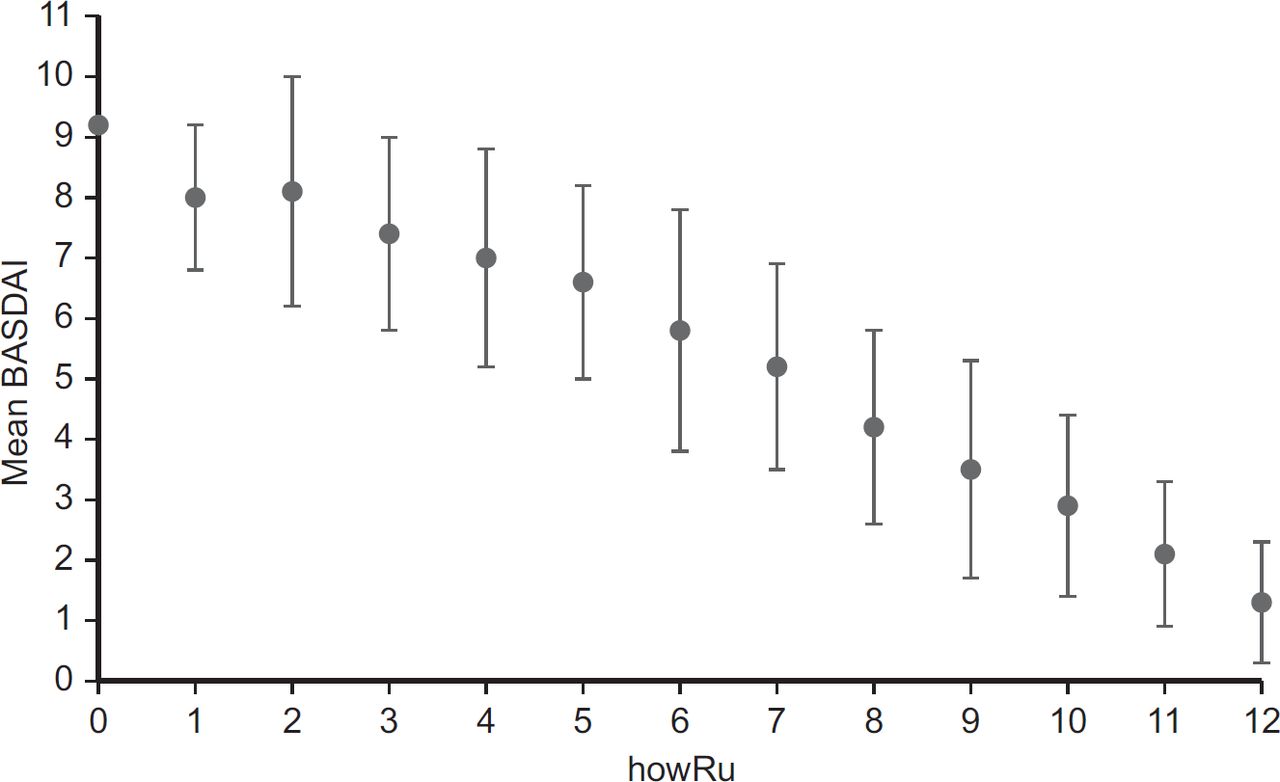
Higher physical activity levels were significantly associated with lower BASDAI even when adjusting for howRU (Table 3 and Figure 3). This supports previous studies where exercise or active lifestyles (even if formal exercise was minimal) have supported the management of AS.24 At least 1 hour of vigorous activity per week also lowered disease activity to below the clinical cutoff BASDAI 4 indicating the need for treatment review (mean BASDAI = 3.31 ± 2.07 versus 4.3 ± 2.17). Analysis of the individual components of BASDAI suggested that physical activity benefited pain, stiffness and tenderness, but not fatigue (Table 3). This contrasts with previous reports,25 where physical activity did improve fatigue levels. The association with peripheral and axial pain and activity was lost when adjusting the models for the howRU score, thus demonstrating the importance that mental health plays in the experience of pain.26
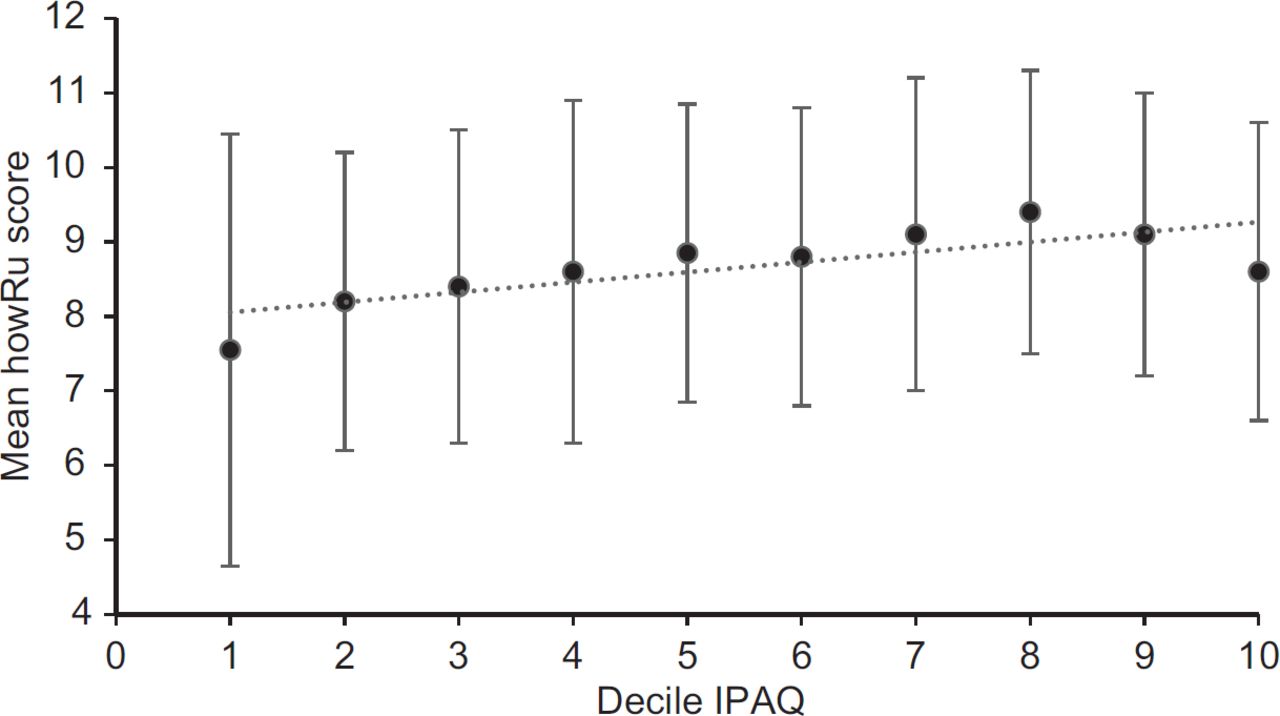
Health-related quality of life scores were very strongly inversely associated with BASDAI (Figure 4). A one-unit increase in the total howRu score was associated with a 0.56 (95%CI 0.50, 0.62, P < 0.001) reduction in the BASDAI score. Increased physical activity was associated with improved overall quality of life (Figure 5) and less pain, even when adjusted for BASDAI (Table 4). This fits with previous research where quality of life was found to very strongly associate with self-reported disease activity,27 and physical activity was noted to improve mental health.26 These findings may indicate that undertaking physical activity even during periods of higher disease activity is beneficial especially for quality of life.
Interestingly, physical activity did not affect the feeling of dependency (Table 4). This may be due to the longer term effects of living with AS, including concerns around the future,28 impacting an individual’s perception of their independence regardless of whether their view of how capable they are changes.
Types of physical activity
Qualitative data analysis on activity types resulted in the generation of a coding framework consisting of five themes, which applied across all activity intensities: exercise, recreation / hobbies, household (or work) activities, care activities, none and an ‘uncategorised’ for unsuitable listings. For each activity, intensity-level codes were generated within each theme and the range of formal exercise listed was extensive. The most frequently noted categories across moderate and vigorous levels were biking = running/walking > therapy > water-based sports > gym > land exercise classes > calisthenics > racquet games > ball games > contact sports (Table S2). Solo activities far outweighed team activities and this may reflect the variable nature of AS. Solo activities tend to require less planning and prior commitment, and therefore individuals can choose to partake depending on their daily wellness. Additionally, it may reflect feelings of confidence in abilities due to the noncompetitive nature of solo activities.28,29
Stratified analysis
Stratification of data by sex (Table 5) demonstrated that BASDAI in women was inversely associated with continuous IPAQ scores. However, this was not seen in men where more vigorous activity was required to see improvements in BASDAI. This may be partially explained by physical activity reducing symptoms that are more common in women, i.e. neck, knees and hip pain and tenderness.30 Physical activity benefitted health-related quality of life for men, with higher levels of physical activity improving howRu scores, but this association was not seen in women. This may be due to differences in the profile of AS symptoms typically seen in men and women.30
Associations between physical activity levels, BASDAI and quality of life were significant for individuals who were HLA-B27 positive (Table 5). No relationship was observed for HLA-B27 negative; however, numbers were low (28 participants). Additionally, in individuals with a disease duration of >10 years, physical activity significantly benefited quality of life, but not BASDAI. More recently, diagnosed participants doing an hour or more of vigorous activity per week associated with improved BASDAI, but negatively associated with quality of life. This may suggest that at early stages of the disease, physical activity negatively impacts the individual, possibly via the interaction of pain and mental health. Furthermore, individuals recording vigorous or moderated gardening (n = 98 versus no vigorous or moderate gardening n = 125) as one of their more frequent activities had higher average log IPAQ scores (7.91 ± 0.93 versus 7.59 ± 0.99) and lower disease activity (BASDAI = 3.59 ± 2.1 versus 4.18 ± 2.0).
Tool evaluation
Participant experience of using the AS Observer tool was generally positive, with the large majority (66 %) expressing intent to continue using it, either for the purposes of self- monitoring tool, active disease management (e.g. identifying triggers), to raise awareness of their own condition or as a motivator to undertake physical activity.
Withdrawal and completion rates
Only three participants chose to withdraw from the study before completion and these were all due to technical issues (including only having access to a phone, not a computer and failure of the site to load on particular browsers). The large majority of participants did not complete data entry every week with an average completion rate of 67%, i.e. 8 of 12 weeks (42% completed ≤ half, 55% completed 7–9 of 12 data entries, and only 3% completed 11 or 12). This fits with previous eHealth studies of web-based monitoring, with adherence rates ranging between 30% and 75%.31 All participants who answered exit questions appreciated the use of reminder emails; however, technical problems prevented some reminder emails being delivered in the last few weeks (reported by 20% of participants) and likely contributed to a drop in compliance. Not receiving reminder emails (including delivery to spam folders) was the main reason given by participants for skipping reporting (44%, Table 6) and this illustrates how important the inclusion of the reminder or prompt mechanism is for effective data collection in eHealth tools.
Participant experience
Exit questionnaires obtained from those withdrawing early (n = 1) and participants at the end of study (n = 92; 41%) were tabulated and coded for each question. Aside from participants who declined to answer (n = 33), the majority intended to continuing using the tool (yes/maybe = 66%). Participants generally found the historical score function useful, enabling monitoring of their condition overtime and helping with selfmanagement approaches.
Usability
Analysis of participant views on ease of tool use, likes and dislikes resulted in the generation of eight codes (Table 7). Participants liked the ability to see plots of their BASDAI scores and would have liked more information graphics (e.g. physical activity and averages for other users) to assist in monitoring their condition. There were split opinions among the participants regarding the tool layout, reflecting personal preference. A number of participants found recording physical activity difficult (Table 7). The use of an activity list as a memory prompt or a smartphone version allowing activity recording to occur at the time was proposed by participants. Additionally, participants would have liked a mechanism to record other influencing factors such as medication changes or periodic medicine use, weather, diet, reasons for no/low activity (e.g. injury/flare up), non-AS ill health, AS associated conditions (e.g. iritis/Crohns), alternative therapies (e.g. massage) and holidays.
Some participants reported technical problems with the website (e.g. compatibility issues and screen freezing during data input), with 28 enquiries to the technical support team. It was possible to resolve 11 of these enquiries, which predominantly related to problems caused when using certain browsers. Further specific information was needed and not obtained for seven enquiries, thus preventing resolution. Further seven enquiries could not be resolved, despite the use of browser mimic software, and due to the lack of an email address, it was not possible to follow up on three enquiries.
Comments received
Comments received via the project website fell into six main themes: statements of support (n = 17), eligibility enquiries (n = 8), comments regarding periodic unavailability (n = 3), technical problems (n = 4) and participation queries regarding confidentiality and time to complete (n = 2). Several comments were also received regarding the module content, which reflected the complex nature of AS and feedback received in the exit questionnaire, namely regarding recording of additional information, e.g. medication and diet, or that data recording did not reflect the complexity of AS (e.g. no functional measurements)or the detailed nuances of exercise (n = 3).
In this pilot study, participants were not asked to modify their physical activity levels; however, participants noted that tool use (including historical scores) helped them to engage with the role of physical activity in their condition. However, there was no evidence of an overall increase of physical activity during the study duration. Therefore, tool use may have enabled participants to engage with their activity and condition, but did not necessarily serve as an effective motivator for the majority.
Strengths and weaknesses
This study was successful in collecting research data of 223 participants, who were representative of AS populations, using an eHealth tool. Whilst not all individuals responded weekly over the 12-week-period sensitivity, analyses including only participants that had completed at least 6 weeks revealed generally similar findings (Table S3).
However, user-orientated platforms present a number of challenges to data collection. The challenges include selfassessment, which is subjective by nature and can therefore lack precision and allows for a range of interpretation and therefore no standardised approach to comprehending or responding to questions or inputting data,32 even when standardised collection tools (e.g. IPAQ) are utilised. Furthermore, there is always a risk of recruitment bias. In this pilot study, NASS was instrumental in recruitment and although other recruitment approaches were used, it is likely that this cohort was dominated by NASS members, who are likely to be of middle to high socioeconomic status (who are more likely to engage in e-health/technology-based research33), consist of potentially more severe AS cases and be particularly engaged with their condition. In this pilot study, we were unable to account for potential biases due to the socioeconomic status of the participants; however, socioeconomic status should not influence the observed associations between AS severity and exercise observed here, which utilised FE models to eliminate omitted variable bias. It should also be noted that due to study duration, it was not possible to account for seasonal impacts on physical activity or symptoms and that due to the nature of the data, the direction of associations, i.e. cause and effect, could not be established.
CONCLUDING REMARKS
This pilot study was successful in its aim to develop an eHealth tool that was user friendly, participant engaging and was able to generate data suitable for epidemiological studies. The AS Observer was generally considered useful by participants, as evidenced by two-thirds of users intending to continue monitoring their condition. The pilot study highlighted the importance of using reminder/prompt systems, providing access to personal data stores for monitoring purposes, and that selfreporting physical activity was challenging. Future studies should where possible include participant tailored elements to provide the opportunity to record the impact of other influencing factors for chronic, variable conditions like AS.
Statistical analysis supported the use of physical activity in AS management to benefit overall disease activity, stiffness, tenderness and pain, but not fatigue. However, adjustment for the howRu data attenuated the associations between physical activity and both peripheral and axial pain, highlighting the importance of quality of life in this relationship. Increased BASDAI was associated with the mental health dimension of the howRu tool (Table 4) and therefore increasing physical activity may have multiple benefits either directly via reduced disease activity and/ or improved quality of life. This study suggests guidance around physical activity needs to consider patient specific factors including gender, disease duration and mental health status.
Ultimately, eHealth tools such as the AS Observer, which may have a key role to play in clinical settings in the future (e.g. self-management of chronic conditions and clinician remote monitoring of patients), also serve as a potential data source for research purposes. Although this pilot study only had a relatively small cohort (n = 223), scaling up participation in AS disease monitoring tools could provide a valuable means to collect data and facilitate research, which will ultimately benefit patients and clinicians alike by providing real-time monitoring and indicating potential treatment pathways.
Acknowledgments
The European Centre for Environment and Human Health (part of the University of Exeter Medical School) is partly supported by the European Regional Development Fund Programme 2007 to 2013 and the European Social Fund Convergence Programme for Cornwall and the Isles of Scilly. Dr Jess Tyrrell is a Diabetes Research and Wellness Foundation fellow. We acknowledge the use of howRu, which is a copyright of R-Outcomes Ltd.