Article Text

Statistics from Altmetric.com
Leaders: Unleashing the power of e-Health requires the right evidence base
The two leading articles in this issue of Informatics in Primary Care describe the importance of creating the right evidence base if we are to Unleash the Power of e-Health. Policy needs to promote well-thought-out developments that are evidence based, have the right theoretical underpinnings and are carefully modelled to see where and how they might fit into the (very human) process of health care delivery and most importantly affect health outcomes.
To inform this debate, we need to be clear about what we mean by e-Health and the evidence base, their origins and definitions (Boxes 1 and 2).
e-Health origins and definition
e-Health: e-Health was a term coined in 1999 out of the realisation that ‘telemedicine’ (technologies that delivered medicine at a distance) was too isolated a concept and that any use of technology had to be better integrated with other information technologies and into health systems.1 Definitions of e-Health have since then sometimes been more Internet centred; for example:
e-Health refers to the organisation and delivery of health services and information using the Internet and related technologies.2
Others take a more health management focus, for example the World Health Organisation definition:
e-Health is the transfer of health resources and health care by electronic means. It encompasses three main areas:
The delivery of health information, for health professionals and health consumers, through the Internet and telecommunications.
Using the power of IT and e-commerce to improve public health services, e.g. through the education and training of health workers.
The use of e-commerce and e-business practices in health systems management.3
e-Health combined with patient access to evidence and their records has the potential to empower patient choice.4
Evidence-based medicine origins, characteristics and grading evidence
Evidence-based medicine: Evidence-based medicine and practice requires greater emphasis on research. One of the first people to think about the importance of evidence from randomised controlled trials was Archie Cochrane, after whom the Cochrane Collaboration was named back in 1972.5 Some 20 years later, there were international calls to move to more evidence-based practice:
Evidence-based medicine de-emphasises intuition, unsystematic clinical experience and pathophysiologic rationale as sufficient grounds for clinical decision making and stresses the examination of evidence from clinical research.
Evidence-based medicine requires new skills of the physician, including efficient literature searching and the application of formal rules of evidence evaluating the clinical literature.6
A key element of an evidence-based approach is to use the best evidence available.
The grading of recommendations assessment, development and evaluation has become a widely accepted approach to judging the strength of evidence of recommendations base on it.
Exploiting the information revolution – should have a better evidence base
The first leading article in this issue critiques the level of evidence used in the document: Exploit the information revolution.7 Whilst the author, editor and the overwhelming majority of our readers are strongly in favour of exploiting e-Health, we would like to see decisions made on the best evidence and a stronger theoretical and evaluation framework in place. This would give this approach the greatest chance of success. In his leading article, Scott talks about this report as a ‘National experiment’.
It is possible that the lessons from the last national programme – enunciated in the pages of this journal as the Hayes principles – may be overlooked.8,9 Good science and good management would suggest that taking greater account of the evidence, relevant theory, modelling, piloting, and rigorous evaluation are vital for success.
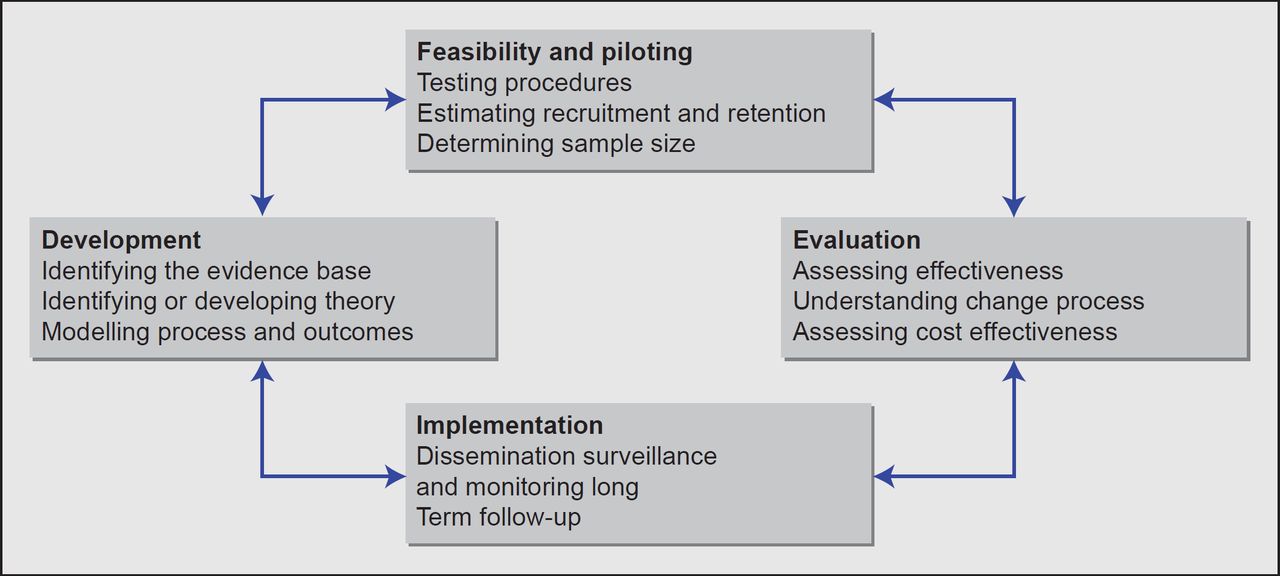
Scott could have gone further and called for the adoption of the Medical Research Council (MRC) framework for the development and evaluation of complex interventions to be used as a model of how ‘Exploit the information revolution’ might have been better written. Changes resulting from the exploitation of the information revolution are likely to be complex. The MRC framework (Figure 1) sets out the theory-based elements that need to be applied to both development and evaluation.10,11

{kind=link}
The delivery of health care is mediated by organisational and individual behaviour, so using models grounded in sound psychological theories of behaviour is helpful in understanding how existing interventions produce their effects and in designing future interventions, including better harnessing of informatics.
Managing multi-morbidity: a grand challenge for informatics
Co-morbidity is common and the ageing population in the developed world has more and more long-term conditions. Most clinicians manage these patients by applying the guidelines for each single condition. Minimally disruptive medicine (MDM) is suggested as an antidote. In MDM, efforts are made to minimise the load of multiple chronic disease management programmes on the patient. However, currently, there is an intellectual gap – we do not have an evidencebase as to which single disease guideline to drop. With most chronic disease management taking place in primary care, computerised medical records (CMR) provide major opportunities to develop an evidence base as to how best to manage multi-morbidity. This is a grand challenge for practitioners, researchers and CMR manufacturers. It is time for the informatics community to think beyond the database of single disease guidelines and prompts generated from them.12
The power of e-Health and having the right information at the right time
Mastellos et al, in their evaluation of the North West London Integrated Care Pilot, report that most of the time they do not have the right information in hand to manage care.13 Less than a third (29%) of practitioners felt they had access to the information they needed to provide safe care. A challenge in managing multi-morbidity is having access to the right data to support care.
Disparities are important in many areas of medicine and Mikles and Mielenz remind us in their paper that there is a digital divide in the use of messaging between a health care provider and patients.14 Non-White people and lower socioeconomic status was associated with lower use of messaging. This needs to be carefully considered at a time when providing patients online access to their records is considered an important element of harnessing the information revolution;15,16 it is certainly not intended to widen disparities. Hewitt-Taylor then discusses the potential risks associated with Internet access and debates the role of health care professionals in trying to minimise associated risks.17
Clinical informatics: fatigue, child maltreatment and more accurate case identification in diabetes
The final three papers in this issue explore different aspects of clinical informatics: patients who present with fatigue, how to record child maltreatment concerns and how case finding in diabetes needs to be adapted to the structure of the clinical record.
Nicholson et al. report from Canada that patients with fatigue can be identified from primary care records and that these patients attend far more consultations and are investigated and referred more than a comparator group in primary care.18 Case finding could be followed up by intervention targeted to meet these patients’ needs.
McGovern et al. report how promoting a simple coding strategy resulted in improvements in the coding and hence the potential to monitor from CMRs children GPs (general practitioners) considered the cause for maltreatment-related concern.19
Finally, your editor writes about the difference in record structure and hence the approach to case finding between problem-orientated medical records (POMR) and those which do not force strict problem orientation. We call the latter episode orientated medical records (EOMR)! Using diabetes as an exemplar, we demonstrate how there are record-design-driven differences in coding practice and hence different strategies are needed for case finding.20 This work followed observations made in detailed multi-channel video observation of different computer systems.21,22 POMR systems mean there was much better linage of consultations/office visits with key problems, whereas in EOMR systems, there was much more use of near synonyms and variation in coding.
Footnote: Journal of innovation in health informatics
After 20 years as Informatics in Primary Care the journal is changing its name. With health care becoming more integrated, it is an appropriate time to change. The new name is the Journal of Innovation in Health Informatics. The rationale for the new name is that it reflects the key elements of the discipline of health informatics.23