Article Text

Abstract
Background Minimally disruptive medicine (MDM) is proposed as a method for more appropriately managing people with multiple chronic disease. Much clinical management is currently single disease focussed, with people with multimorbidity being managed according to multiple single disease guidelines. Current initiatives to improve care include education about individual conditions and creating an environment where multiple guidelines might be simultaneously supported. The patient-centred medical home (PCMH) is an example of the latter. However, educational programmes and PCMH may increase the burden on patients.
Problem The cumulative workload for patients in managing the impact of multiple disease-specific guidelines is only relatively recently recognised. There is an intellectual vacuum as to how best to manage multimorbidity and how informatics might support implementing MDM. There is currently no alternative to multiple singlecondition- specific guidelines and a lack of certainty, should the treatment burden need to be reduced, as to which guideline might be ‘dropped’.
Action The best information about multimorbidity is recorded in primary care computerised medical record (CMR) systems and in an increasing number of integrated care organisations. CMR systems have the potential to flag individuals who might be in greatest need. However, CMR systems may also provide insights into whether there are ameliorating factors that might make it easier for them to be resilient to the burden of care. Data from such CMR systems might be used to develop the evidence base about how to better manage multimorbidity.
Conclusions There is potential for these information systems to help reduce the management burden on patients and clinicians. However, substantial investment in research-driven CMR development is needed if we are to achieve this.
- chronic disease
- comorbidity
- computers
- computerised medical record systems
- data collection
- health behaviour
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
- chronic disease
- comorbidity
- computers
- computerised medical record systems
- data collection
- health behaviour
Introduction – what is Minimally Disruptive Medicine (MDM)?
The way that we manage people with multiple chronic diseases creates an enormous care burden for patients; we apply multiple single-condition clinical practice guidelines. Minimally disruptive medicine (MDM) recognises this, and seeks to work more closely with patients and help them make appropriate choices.1 Much of our evidence-based guidance is single disease specific and their implementation results in a considerable care burden for patients.2 This is particularly so where secondary care is involved because most specialities are system based. However, it is also often reflected in primary care where there may be separate but concurrent management of diabetes, chronic obstructive pulmonary disease and other conditions.
Some of the current solutions provided to support and empower patients risk making things worse if they simply add cognitive and workload burden. These often consist of diseasespecific education programmes for patients and schemes, such as the ‘patient-centred medical home (PCMH)’, which set out to ensure that every element of a patient’s disease-specific evidence care is implemented. This may partially explain why single-disease guidance, such as Diabetes Education and Self- Management for Ongoing and Newly Diagnosed, designed to improve management in diabetes, did not show an improvement in its primary outcome measure.3 Though systematic reviews of the PCMH suggest there are small benefits in patients’ experiences, these are not reflected in clinical outcomes.4
MDM recognises the importance of applying Engel’s biopsychosocial model of disease.5 Engel described how all diseases had physical, psychological and social components. This is something readily forgotten in the priority to implement single-disease-focused, evidence-based guidance. This may particularly be so where these are financially incentivised, and clinical data recording has a purpose beyond that of direct patient care.6
Engle stated, back in 1977:
“The dominant model of disease today is biomedical, and it leaves no room within its framework for the social, psychological, and behavioural dimensions of illness.”
MDM should be included in our implementation of holistic care, perhaps refocusing models like the chronic care model7 towards multimorbidity. This involves an informed, activated patient weighing up whether they can manage their current burden of self-care let alone take on additional clinical and lifestyle responsibilities.
The problem
It is unclear as to what role informatics should play in supporting the management of multimorbidity and strategies for implementing MDM. Whilst it is easy to acknowledge the challenges in managing multimorbidity, it is much harder to identify what should not be done in order to make management of multimorbidity less disruptive for patients, their carers and the clinical team involved in their care; and how informatics and information systems might support this process.
Action needed
We propose that the informatics community should be actively exploring how informatics might be transformational in supporting the management of this group of patients.
Firstly, much of the provision of care to people with multimorbidity is, in its classic sense, computer-mediated work.8 Much of the care given to people with multimorbidity takes place in primary care and internationally primary care is increasingly computerised; there is a considerable body of knowledge as to how such data might best be used for research.9 Primary care, and where available, integrated care data – which include hospital, community and social care data – should be the focus of multimorbidity research.
Secondly, we should be able to use existing systems to flag people in greatest need who require MDM.
Thirdly, we should be able to balance likely needs for MDM with potential ameliorating factors and flag the likelihood that a patient is overloaded.
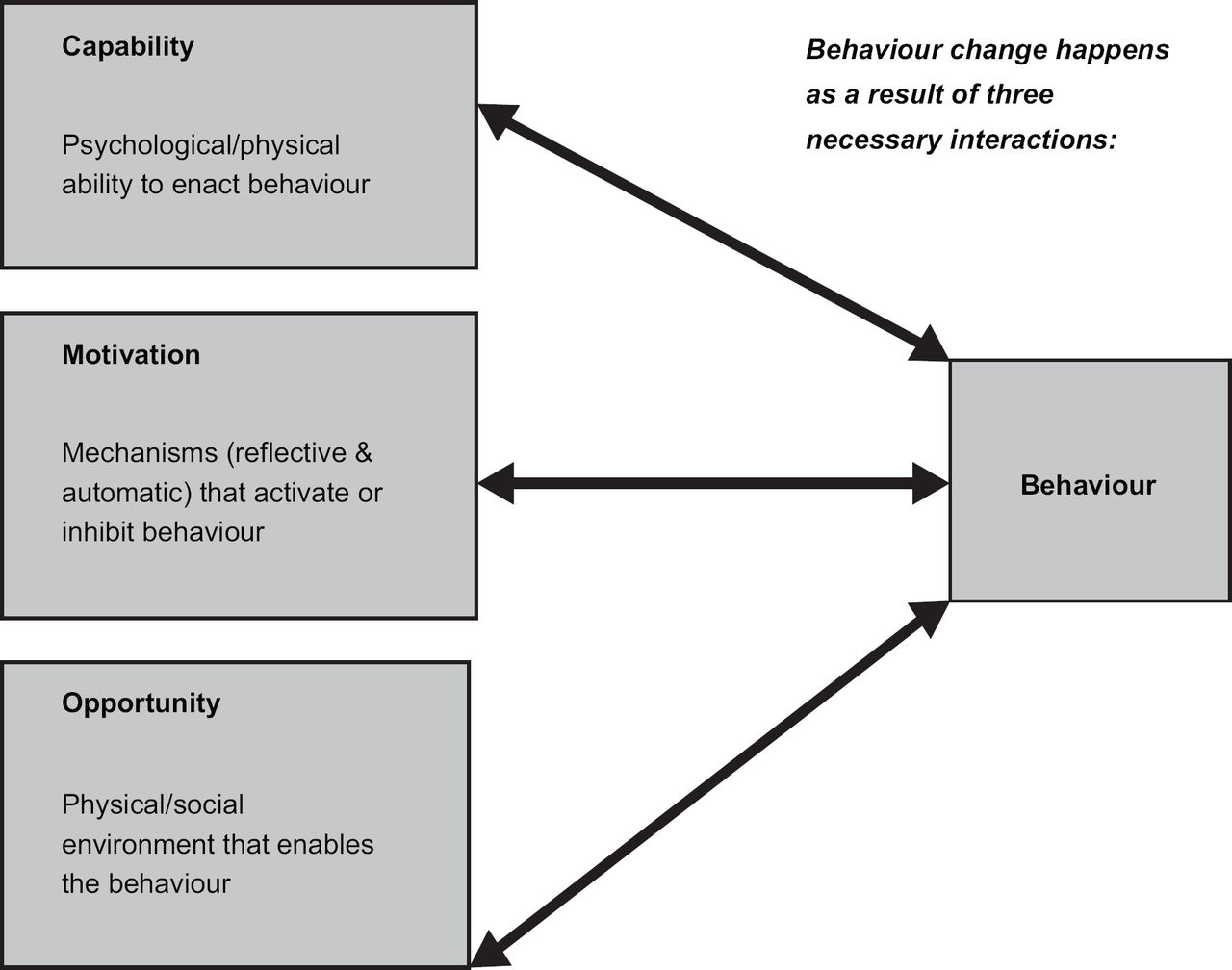
Finally, we need to recognise that we are often looking for a change in behaviour from patients and carers. Whilst the choice of behavioural change mechanisms is not something to be mandated from within the informatics community, if record systems are to improve health, then they need to be linked to an appropriate behaviour change model. We use the ‘COM-B’ model from the Behaviour Change Wheel.10 This model suggests that for behaviour change to take place, the capability to make the change is needed. Also required is the opportunity, which can be limited by physical or social circumstances, to promote change, as well as the motivation to do so (Figure 1). This is known as the COM-B model (Capability, Opportunity and Motivation, for Behaviour change). Computerised medical records (CMRs) should ideally differentiate between information collected on the behaviours themselves and the capability, opportunity and motivational factors that might determine behaviour.
What data are available in current CMR systems to identify people with comorbidities in greatest need of MDM?
The informatics community should not only be looking to flagging multimorbidity, but also thinking of what signals exist within the clinical information systems that might help identify patients who are likely to have a treatment burden, and hence in need of MDM. As yet there are no clear definitions or guidelines to identify those patients who might need less disruptive interventions. The informatics community should be ready, waiting and willing.
There may be information available that helps answer the question of MDM in routine clinical records:
Chronic disease data: Data about individual chronic diseases are well recorded in primary care records; these can be used to identify people with multiple conditions
Prescribing data: Prescribing is the highest quality data within the medical record. Prescribing data can be used in four ways, with the first three referring to predisposing circumstances and the last to behaviour:
To infer comorbidities not coded in the record.
To use the level of polypharmacy as an indicator in itself.
To assess whether prescriptions are for volumes of tablets that are likely to be placed into a daily tablet dispensing system. People provided such systems are likely to have had poor adherence to their medications.
To indicate whether the clinical record implies poor adherence (a behaviour).
A Cochrane review of the management of multimorbidity suggested that improving prescribing and medication adherence might have a positive impact on care.11
Data about common mental health problems (CMHPs): Depression and other CMHPs appear to be associated with worse outcomes.12
Risk scores/indicators: Indicators that might suggest scope for improved care or iatrogenic, primarily medication-related, problems:
Falls and fractures
Confusion and memory problems
Administrative data: Registration and administrative codes may also provide useful information:
Post code/zip code can often be linked to indices of multiple deprivations, something widely associated with disparities in health care and poor outcomes (a circumstance that impacts on an opportunity to change behaviour)
Record of non-attendance in general practice or to hospital clinics (a behaviour)
The recording of a specific carer or if there are others registered at the same address
Possible evidence of anticipatory care being provided for the patient, such as an active care plan.
There are probably other factors that might be important and need to be tested. This list represents a start and might enable models to be created that might flag the likely load on individuals and their care givers.
Ameliorating factors that might be flagged from enhanced CMR systems
Factors have been proposed that might ameliorate the burden of treatment for complex patients.13 It is possible that these might be identified, though currently only in part, from CMR systems. They could be part of the clinical assessment of a patient’s capability to manage their complex needs.
Problem-focused strategies: These include routinising self-care, enlisting support of others, planning for the future and using technology (behaviours).
Emotion-focused coping strategies: Maintaining a positive attitude, focusing on other life priorities, and spirituality or faith.
Questioning the notion of treatment burden as a function of adapting to self-care: Some people will actively question their treatment burden and compare themselves to others, and make decisions about treatment based on these perceptions.
Social care information: Social support can be informational, tangible or emotional forms of assistance (circumstances that may impact on opportunity).
Positive aspects of health care/care coordination: This includes coordination of care and beneficial relationships with providers of health care. The Cochrane review of interventions to improve the care of comorbidities flagged better organised care delivery, especially through case management or enhanced multidisciplinary teamwork.13
The challenge for informaticians is how we might flag whether behaviour change is feasible given an individual patient’s circumstances. This type of information is rarely comprehensively recorded, and some pieces of information, such as spirituality and faith, are not generally recorded for reasons including fear of these labels being used to support sectarianism. The last two items could possibly be inferred from the medical record, care plans, social care or other reports contained in the CMR.
In the context of the PCMH, some have started to think through how information systems might support this approach to holistic care.14 The information identified in this section identifies information that might be important in measuring the determinants of behaviour – capability (psychological and physical), opportunity (physical and social) and motivation (reflective and automatic), as flagged in the COM-B model (Figure 1).12 For example, the ameliorating factor of social support could be connected to social opportunity (Figure 2).

{kind=link}
{kind=link}
The new CMR system needs to be able to support more holistic management of multimorbidity and move on from providing libraries of support tools for single conditions.
Summary: What should informaticians do?
CMR systems need to be developed to support the clinical management and care planning for people with multimorbidity. Informaticians should have a leading role in the research that might enable this to be done. Our current CMR systems are often good at supporting the delivery of single-condition guidelines, and have not yet addressed the challenge of multimorbidity. The increased burden created by an ageing population with multimorbidity is unsustainable and cannot be managed as multiple single conditions.3 These patients, their carers and physicians all need a less disruptive approach.
The first step would be to develop, test and evaluate approaches that could flag people who are less likely to be able to adhere to the multiple disease programmes that they might be registered in. We would have to assess the validity of our proposed approach of balancing need with ameliorating the factors concerning capability, opportunity and motivation (Figure 2).
We also need to give an opportunity for patients to engage with their health care provider in a way that maximises their autonomy; this may need to go beyond what is currently planned for online access to medical records.15 To do this, we also need to flag to patients themselves, clinicians, and other decision makers in health and social care the opportunity, capability and motivation to change behaviour. MDM will be appropriate for many.