Article Text

Abstract
The proliferation of mobile devices and emergence of interoperable ‘mHealth’ apps is accelerating development and deployment of patient-facing risk assessments in primary care. The present study describes a user-centered design and an agile development approach to creation of an app for assessing lung function as part of a randomized controlled trial for the identification of chronic obstructive lung disease in primary care. Seventeen patients recruited from a hospital-based, ambulatory family medicine clinic agreed to be videotaped while using the app, Lung Age, on a first-generation iPad prior to their provider encounter. Subsequently, participants were interviewed using a semi-structured interview guide upon exiting their medical visit. Observational data indicated that participants took advantage of the portability and flexibility of the tablet device in the exam room to engage with the Lung Age app with the option to share and discuss their results with their providers. Results from the semistructured interviews indicated that participants perceived the Lung Age app as intuitive and easy to use. These results demonstrate that tablet computers and mHealth apps can be used to deploy acceptable and useable electronic risk assessments in primary care settings. Future research focused on the impact and outcomes of patient-centered, mHealth apps for risk screening in primary care is warranted.
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Background
Health information technology (HIT) is assuming a major role in the transformation of the health care system into a more patient-centered, efficient, safe and collaborative enterprise.1,2 The Meaningful use (MU) rule for the HIT is powering the rapid adoption of a digital infrastructure of electronic medical records and patient portals in the US to support the emerging structures of the next generation of patient-centered medical homes (PCMHs) and accountable care organizations.1 Additionally, patient-facing HIT is proliferating and activating patients to become more engaged in self-care and collaborative management of their health conditions in concert with their providers.3 This combination of technology-supported providers and engaged and activated patients is particularly promising in the context of the PCMH and in promoting the effective and efficient management of chronic disease.
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic condition encountered in primary care, a major cause of morbidity and mortality worldwide, and one that substantially adversely impacts quality of life.4 A number of initiatives have been developed to address the burden of COPD with some evidence of significant progress.5,6 Despite these efforts, COPD remains an underdiagnosed and undertreated condition. Consequently, there is a need to engage patients to become more aware of their risk for COPD based on evidence-based protocols (http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html).
Evidence suggests that information that assists patients in understanding their clinical conditions has been effective in promoting patient–provider decision making, reducing decisional conflict and increasing patient adherence to their health care plan.7–9 However, given that reviewing tailored information with each patient can be costly in terms of time and resources,10 the availability of mobile, low-cost tablet computers may provide an opportunity to overcome this challenge. Tablet computers can be used to provide relevant and tailored educational information to patients, to collect patient reported data and to enable patients to view their condition-specific, health care information.
As part of a larger study to examine the translation of the GOLD Guidelines into primary care practice, we developed a patient and provider clinical decision support program, The Lung Age System. The study design and protocol for this randomized controlled trial (RCT) is described in detail elsewhere.11 In this article, we focus on the design, development and evaluation of an iPad software application to assess patient’s risk of developing COPD and to provide COPD patient education information via video. Further, we discuss examples of the challenges encountered, lessons learned, and the relevance to MU of HIT in the PCMH.
Method
Overview of main trial
The main study on which this report is based was a block, randomized design cluster trial (RCT) with a one-year intervention within 30 general, primary care practices throughout Rhode Island and southeastern Massachusetts. Our approach was based on the chronic care model,12 which provides a useful theoretical framework to understand the basis for improved quality of care outcomes in the ambulatory care setting. The major tenet of this model is that an informed, empowered patient will interact with a patient care team led by the provider to develop productive communications and actions that will result in improved health care outcomes. There is a large body of evidence that demonstrates that involving the patients’ and their families’ perspectives, preferences, priorities and understanding of the delivery of health care (patient centeredness) improves health outcomes.13–15 During phase 1 of this study from 2010 to 2011, a need assessment was conducted which evaluated barriers and facilitators to implementation of COPD guidelines into clinical practice through focus groups of primary care patients and providers. Using the formative evaluation and feedback from the focus groups, we developed, refined and pilot tested a computerized patient activation tool delivered on an iPad platform. The iPad patient activation tool was then placed in offices of primary care providers (PCPs) who were randomized to the intervention arm of the study. In phase 2, we examined the use of the patient activation tool to prompt patients to talk with their health care provider regarding their lung health and risk for COPD.
Procedure for development of the tool
Primary care patients who were English speaking were approached by study staff while waiting in the examination room at Memorial Hospital of Rhode Island to see if they would be interested in participating in a pilot study. This is a general medical clinic where providers evaluate patients for any presenting medical complaint. Patients were not selected on the basis of having a diagnosis of COPD. Patients were asked if they would be willing to use the COPD risk assessment application on an iPad and then participate in a brief interview about their experience using the iPad application. This study was approved by the Memorial Hospital of RI Institutional Review Board, and patients signed an informed consent and were informed that they would be videotaped while using the iPad in a private examination room. Video cameras installed in the ceiling of exams rooms for resident training and research were used for recording.
Usability testing data collection
A consecutive sample of 17 patients tested the iPad prior to their medical visit while waiting in the exam room. Each was interviewed upon exiting their medical visit. Then, approximately 15 minute interviews were audio recorded and conducted by one of the investigators (RG), an experienced qualitative interviewer. Patients received $20 for their participation.
An iterative and agile design process was employed in creating the iPad app. Wire frames were created and reviewed by study staff and early stage prototypes created and tested repeatedly in serial focus groups with patients. The final design was user tested with the 17 primary care patients prior to beginning the randomized clinical trial (see Figure 1 for sample screen shots).

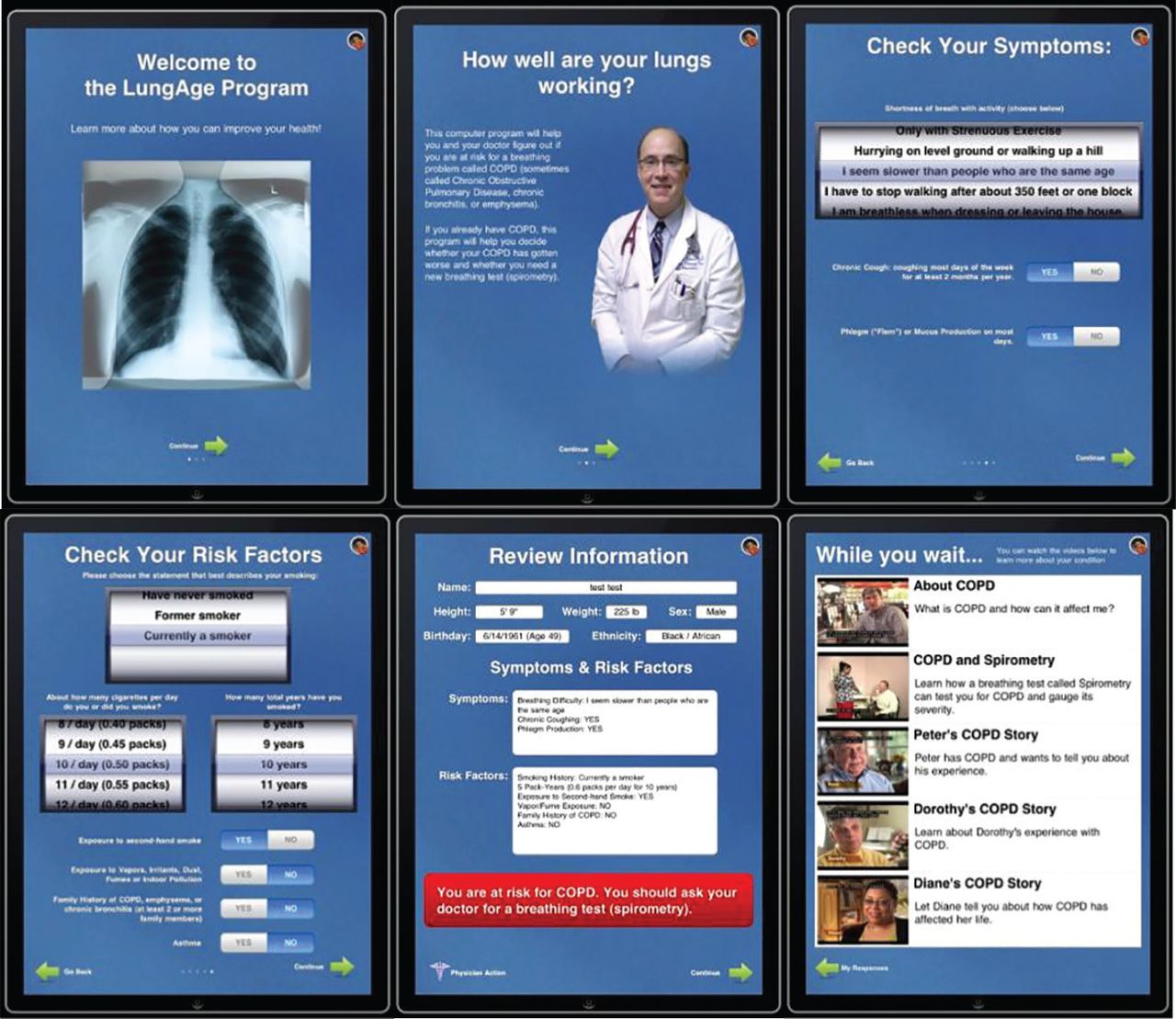{kind=link}
A research assistant explained to the patients how to use the iPad and how to complete the risk assessment embedded in the software following completion of the embedded informed consent. Participants completed a lung health survey and were encouraged to view from one to three educational videos related to COPD and spirometry (if time permitted) prior to seeing their PCP. Usability was assessed observationally by the team of investigators who reviewed the videotapes of the patients using the iPad in the examination room and by the posttest qualitative interview (See Table 1). During the interview, patients were asked questions about their overall impressions of the app, their likes and dislikes and other comments that would help us with needed design changes based on any observed obstacles that interfered with the patients completing any of the tasks.
Results
Participants were from diverse backgrounds (See Table 2).
Sixty-five percent of the participants were women; the mean age was 54 years old with an age range of 32 years to 71 years. Thirty percent had a high school education or less, 64% has at least some college education (education ranged from <9th grade to PhD), 82% were Caucasian and 70% were former/current smokers. Individuals also had different levels of experience with computers with some very knowledgeable, some owning and/or having used an iPad and others who had never used a computer.
User experiences
The average time from beginning to end of use was approximately 6 minutes (range 2 to 9 minutes). All usability concerns were first identified in the interviews and corroborated by review of the videos. All participants completed the survey on the iPad.
Observations of patients’ use of the iPad: A majority of the patients were able to complete the navigational tasks without difficulty and without additional instruction from the research assistant. Despite challenges experienced by several patients, they were also able to complete the risk assessment application. It was notable that patients assumed a variety of postures and used different approaches to holding the iPad and interacting with it. Some patients sat, while others stood and several moved from one position to another. One patient had long, acrylic nails and had to find a way to use her finger pads to navigate the application since it would not work with her nails. Another patient had two small children with her and remained engaged throughout the whole process of completing the application despite the children climbing on her and wanting her attention. A third patient had severe back pain and continually moved around the patient examination table since he could not sit due to the pain and carried the iPad with him so he could complete the questionnaire.
Topical insights that emerged from the qualitative interviews were about: 1) ease of use, 2) acceptability and feasibility, 3) patient engagement and 4) difficulty in use.
Ease of use: Most of the patients found the iPad application easy to use, gamelike, and interesting, although three patients required additional instruction prior to using the iPad. Comments included: ‘I was excited about it because I’m a ‘techno dunce’ and I hear about all this technology. But it was quite easy to use.’ ‘I thought it was cool. I don’t have a computer, so I was kind of scared at first, but it was pretty good.’ ‘I liked it. It seemed easy to scroll the pages and read it and it was big enough to read’.
Acceptability and feasibility: Patients appeared to find the iPad acceptable, engaging, and intriguing even among individuals who did not feel comfortable with technology. Comments included, ‘I don’t like electronics and get nervous even on my TV. I’m glad I did it. After I used it, I began to realize it is something good to have.’ ‘It’s quick. It’s not hard to figure out like the computer. It was very easy for me. For the first time using (an Ipad) I did really well’. ‘I found it to be very informative, and I watched the first video. It’s just much more… much easier than a paper, a piece of paper filling out. It being state of the art, I didn’t have concerns about it like even getting lost. You know, like the paper getting lost or being put into the wrong hands or, you know, privacy issues. I felt that it was more of it, was more advanced in that aspect’.
Patient Engagement: Patients were engaged and were able to complete the tasks in the iPad application despite disruptions (for example a mother with two children who were competing for her attention and a patient in severe back pain). As one patient stated, ‘For me, I used it therapeutically to get my mind off my pain. So it was nice.’ Another patient noted, ‘Much easier than filling out a piece of paper. It’s quick and easy and painless’. In terms of comprehension of the material, one patient noted, ‘I found it very informative, and I watched the first video’. Another patient also mentioned, ‘It was nice you had the videos in the end. People could watch and explain to them what it is [COPD] because I don’t think a lot of people realize what it is’.
Usability: One patient found the iPad screen hard to read unless it was at a particular angle, another patient had a problem with the buttons and several patients reported difficulty scrolling initially (not initially intuitive) and two patients found the iPad heavy. The first patient stated that ‘I don’t like that the screen wouldn’t adjust if I tilted it other ways. I was afraid to drop it. There’s no strap on it or anything too.’ Another patient felt ‘the buttons could be easier because at first I couldn’t use the button but I got it to work, you know, to continue it said either slide over it or tap. It would be nice if it was up in the corner like a turn of a page thing’. Another patient felt that what was needed was to ‘provide a mechanism for navigating through the videos. I couldn’t figure out a way to maneuver through it anyway’.
Discussion
These results demonstrate that tablet computers can be used to deploy acceptable and useable electronic risk assessment apps in general primary care settings. The patient-facing, Lung Age app on the first generation iPad was deemed feasible and perceived as intuitive and easy to use by patients undergoing screening for COPD. Observational data indicated that patients took advantage of the portability and flexibility of the tablet device in the exam room to engage with the screening application and then share and discuss their results with their provider. Our results are consistent with other published studies of patient attitudes about tablet use in the exam room.16
Applying a user-centered design and agile approach allowed the patients as the end users of the Lung Age app to be active participants in the development process and had the advantage of producing updated versions to further review in an iterative manner. This process allowed for the feedback from patients to be reviewed and incorporated into the app quickly because of short (approximately 4-week) development cycles (Sprints) between each new version released. We were able to incorporate changes and suggestions in subsequent iterations of the app based on the observations and comments from the pilot group of patients. This iterative process allowed for new changes to be tested rapidly and was a significant factor in producing an engaging, informative and patient-centered application.
Despite the overall positive reception by patients, a number of challenges and barriers to implementation within general primary care were noted. The study timeframe coincided with the rapidly evolving technology landscape, with early-stage implementation of EMR systems in many practices and the onset of several PCMH demonstration projects within the region. Technology literacy varied widely across participants and remains a barrier to universal adoption and use of technology-mediated screening approaches. Other factors may be at play as well including provider indifference and lack of incentives for shared decision making.17
Despite some difficulties that have to be overcome by some patients, the Lung Age app on the iPad illustrates the promise and potential value of patient-facing technologies that undergo rigorous user-centered design evaluations. Patients were generally highly satisfied with the iPad Lung Age app and many comments indicated the tool helped them to learn more about their condition and prepared them for making a more informed decision about spirometry testing, if recommended by their physician. Notably, the embedded videos were cited by several patients as particularly informative and helpful in understanding COPD.
The available evidence demonstrates more than a doubling in the rate of adoption of tablet computers by physicians since 2011, reaching 72% in 2013.18 Likewise, patients are increasingly being offered tablets and other mobile or ‘mHealth’ technologies to support engagement and activation. Technology-mediated applications and resources will be essential for successful patient engagement as part of evolving PCMH models and to support MU of the HIT.
There are a number of limitations that need to be addressed. The sample size is small and because of the consecutive sampling, it may not be representative of the full range of patients appropriate for lung screening in primary care. Nevertheless, despite the small sample size used for this pilot, we did reach saturation of our themes. Additionally, we only addressed the use of the iPad application with English-speaking patients and it is unclear about the ease of use and material presentation among non-English speaking patients.
Conclusion
The burgeoning growth of mobile devices and mHealth apps holds great promise for developing and deploying patient- facing technologies for risk screening in general primary care settings. The present study demonstrates that patients with varying levels of technology literacy can be engaged in screening for lung function using a tablet computer and patient-centered app. Future research focused on the impact and outcomes of patient-centered apps for risk screening in primary care is warranted.