Article Text

Abstract
Introduction Obsolete bleep/long-range pager equipment remains firmly embedded in the National Health Service (NHS).
Objective To introduce a secure, chart-integrated messaging system (Epic Secure Chat) in a large NHS tertiary referral centre to replace non-emergency bleeps/long-range pagers.
Methods The system was socialised in the months before go-live. Operational readiness was overseen by an implementation group with stakeholder engagement. Cutover was accompanied by a week of Secure Chat and bleeps running in parallel.
Results Engagement due to socialisation was high with usage stabilising approximately 3 months after go-live. Contact centre internal call activity fell significantly after go-live. No significant patient safety concerns were reported.
Discussion Uptake was excellent with substantial utilisation well before cutover indirectly supporting high levels of engagement. The majority of those who previously carried bleeps were content to use personal devices for messaging because of user convenience after reassurance about privacy.
Conclusion An integrated secure messaging system can replace non-emergency bleeps with beneficial impact on service.
- Electronic Health Records
- Information Technology
Data availability statement
Data sharing is not applicable as no data sets were generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
In 2019, the UK Health and Social Care Secretary announced that the National Health Service (NHS) should remove bleeps and pagers for non-emergency communication by the end of 2021.1 2 While this technology is now in costly obsolescence and pilot studies have shown efficiency saving3 using smartphone messaging, legacy equipment remains firmly embedded in the NHS. Optimal strategies for adoption have received little attention4 and barriers to adoption have been identified.5
Cambridge University Hospitals (CUH) NHS Foundation Trust has used a comprehensive Electronic Health Record (EHR, Epic Systems Corporation, Verona, Wisconsin, USA) since 2014. An information-governance compliant messaging solution (Epic Secure Chat) allows for messaging from smartphones, tablets or from within the EHR itself (desktop). The system is fully integrated with the patient chart so that messages and all read/reply times become part of the patient record. Large-scale implementation of an EHR-integrated messaging system to replace non-emergency bleeps/long-range pagers in an NHS organisation has not been previously described.
Setting
CUH is a large, tertiary referral centre in the East of England. It offers a diverse range of services with over 1100 beds and approximately 16 000 staff. A significant EHR upgrade (from Epic 2017 to the November 2020 version) was undertaken during the implementation period bringing additional Secure Chat functionality. The implementation period also coincided with a major Wi-Fi infrastructure upgrade to give full coverage across the estate.
Our aim was to replace all bleeps/pagers apart from ‘cardiac arrest’, ‘major trauma’ and ‘fire’ with Secure Chat (online supplemental S1).
Supplemental material
Methods
Secure Chat was made available at our organisation in July 2021. A go-live date in early 2022 was initially chosen due to ongoing COVID-19 pandemic disruption and to leverage additional necessary Secure Chat functionality that would only become available after an Epic version upgrade planned for November 2021.
An implementation group with executive responsibility was formed with representation from the hospital’s divisional structure to oversee the project. Socialisation was achieved by a network of ‘clinical champions’ and through regular communications including trust bulletin items, face-to-face and online question and answer events as well as information on screensavers and posters and offering at-the-elbow support in clinical settings. An etiquette guide was published to define appropriate use of different methods of communication. Our safety surveillance is described in (online supplemental S5).
Contact centre (online supplemental S2) workload was a key concern at the time of cutover since any communications difficulties would likely result in a call to an agent for help. For safety a transition period where contact centre operatives would send messages both to Secure Chat and to existing bleeps for 1 week post go-live was planned. Secure Chat would not be available during (un)planned Epic outages for which the contingency was to fall back on an internal directory of alternative contacts securely maintained by the contact centre and this was widely publicised.
Secure Chat allows for various groups to enable team and role-based messaging. Because of system limitations at the time of the original implementation, our hospital had not fully implemented a sign-in system which we could leverage for automatic group creation. Instead, we created ‘opt-in’ groups to replicate existing roles, relying on staff to opt-in (out) at the beginning (end) of their duties (online supplemental S3).
Mean comparison was with t-tests; structural breaks were examined using the Chow test. Statistical significance was taken at p<0.05.
Results
Technical
Secure Chat access was enabled for all members of staff with an Epic login. Non-clinical users, (such as contact centre agents, were not given security to view patient charts). Users who would previously have used bleeps were strongly encouraged to use their own personal devices although mobile phones (or pool phones) were provided in a relatively small number of cases where staff did not have a suitable device or were unwilling.
Workflow
For the mobile app, onboarding involved installation of a CUH-specific profile and a website was set up for this. An initial manual batch activation step was subsequently automated using Blue Prism robotic process automation software (Blue Prism group, Warrington, UK) so that registrations could be completed day and night.
The creation of opt-in groups was a major undertaking and had to be done centrally as no reliable list of baton bleep roles existed. An initial list of some 220 groups was compiled from information from clinical champions and existing bleep lists. After some local user acceptance testing, these groups were made available in December 2021. Inevitably creation, editing and deletion of groups was necessary, and this needed to be done centrally: a review process was set up to ensure consistency.
Outcomes
Adoption through socialisation in the months before go-live across all staff groups was rapid (online supplemental figure S2,S3) across all staff groups with pharmacy (and pharmacy technicians) proving to be an unexpected early adopter. The original 4 May 2022 go-live date was pushed back at a final go/no-go meeting to 8 June 2022 due to isolated specialty-specific readiness concerns. Gross total messages sent plateaued at over 600 000 by 3 months after cutover. Opt-in group maintenance peaked before go-live (online supplemental figure S4) although a significant maintenance burden occurred after the original 4 May date.
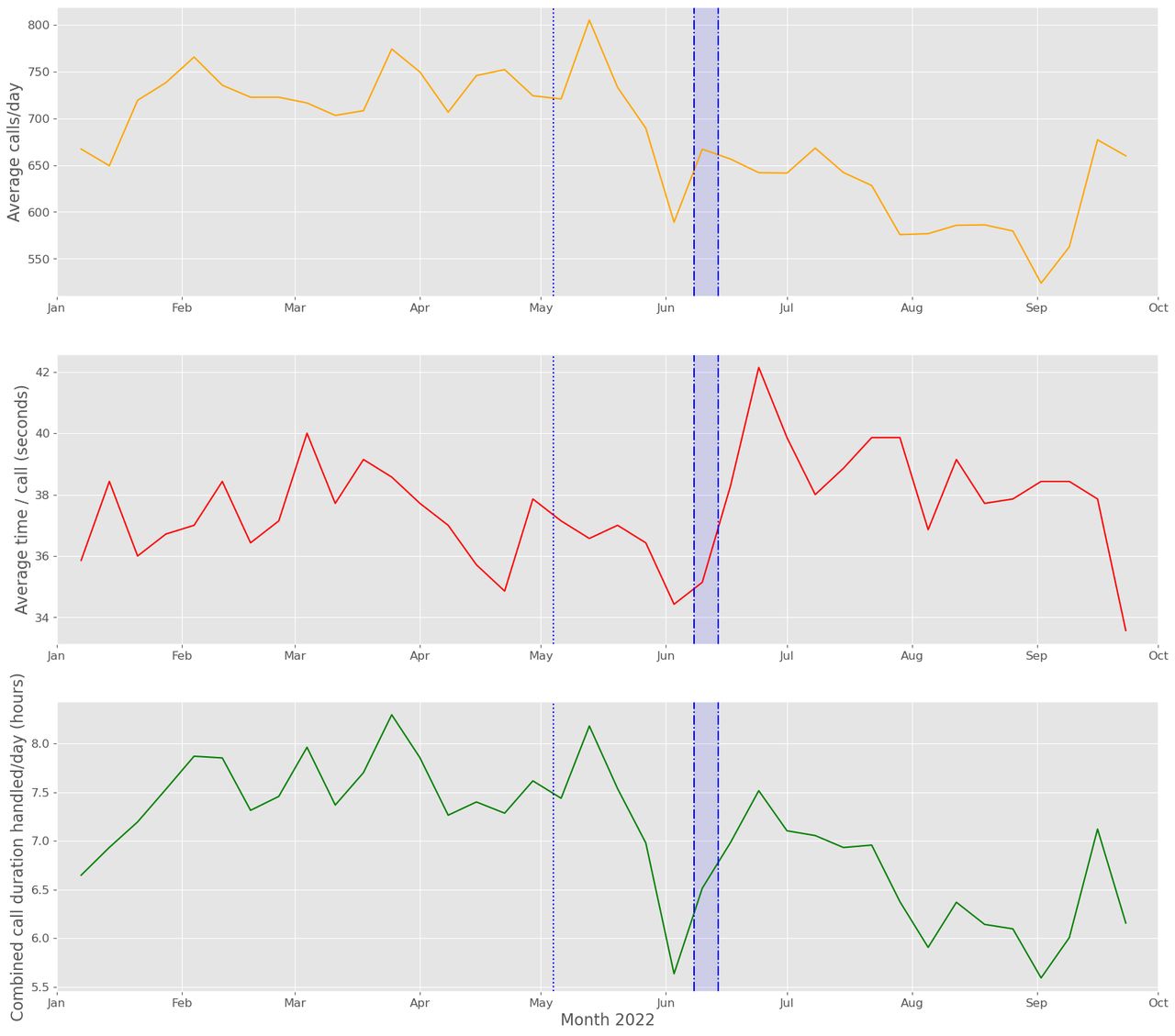
Internal call data handled by contact centre operatives is shown in figure 1. The average number of internal calls handled by contact centre operatives fell from 720 to 614 per day (p<0.0001) after implementation. While average time/call increased marginally from 37 s to 38 s (p=0.014), the total call duration per day fell overall by nearly an hour from 7.4 hours to 6.5 hours per day (p<0.0001). There was evidence of significant structural breaks for call numbers and average call time, but not for overall call time (p=0.01, 0.0003 and 0.06 respectively).
{kind=link}
Uptake and organisational impact of Secure Chat implementation. Top panel: internal calls handled per day. Middle panel: average contact centre time spent per call (seconds) Bottom panel: total call time (hours). Dotted line represents date of delayed initial go-live. Data are averaged by week to remove fluctuations from weekends.
No significant risk events attributable to the Secure Chat implementation were reported (online supplemental S5).
Discussion
We demonstrate that secure messaging can be implemented in a tertiary NHS hospital without significant incident or negatively impacting on contact centre activity. This was possible even without physically retiring the legacy system: bleep counts dropped to negligible levels (online supplemental figure S3) which is important as multiple coexisting communication methods risk overload.5
It is anticipated that the bleep system will be decommissioned in due course depending on a future resilience analysis.
While a minority of staff expressed reservations before go-live citing privacy concerns we were able to provide assurances; most were ultimately content to use their personal devices which offered convenience advantages. The largest complaint received from users concerned inappropriate use of Secure Chat for non-urgent messaging. This is a known issue3 but the etiquette guide which set out clear expectations was key central to empowering staff to challenge inappropriate messaging.
A number of short (1–2 hours) routine Epic upgrade outages have subsequently taken place (scheduled at weekends and night-time) during which time Secure Chat was not available. Concerns that the contact centre could be overwhelmed at these times have not materialised.
Conclusions
We were able to effectively replace non-emergency bleeps/long-range pagers with a messaging system integrated with the patient chart in a large NHS academic hospital by the soft approach of socialisation before cutover. Discounting the time before our EHR upgrade in November 2021, we were able to do this in 7 months with message numbers and support needs stabilising within approximately 3 months of go-live using existing infrastructure and without significant incident.
Data availability statement
Data sharing is not applicable as no data sets were generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank the CUH eHospital team and Management Executive for
support and engagement with this initiative. The authors also thank Joseph Scott, Richard Wallis, Benjamin Styllianou, Rose Cormie and Olivia Bentham for their help in obtaining implementation data.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ari.ercole
Contributors All authors were involved in the implementation of the project. AE wrote up the project with approval from all other authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None at the time of implementation however AC will be leaving the role of Director of Digital at Cambridge University Hospitals in February 2023 to take up a post with Epic Systems Corporation. (This is not a conflict of interest as per the COI form but we include it for complete transparency.)
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.