Article Text

Abstract
Background The implementation of telemonitoring at scale has been less successful than anticipated, often hindered by clinicians’ perceived increase in workload. One important factor has been the lack of integration of patient generated data (PGD) with the electronic medical record (EMR). Clinicians have had problems accessing PGD on telehealth systems especially in patient consultations in primary care.
Objective To design a method to produce a report of PGD that is available to clinicians through their routine EMR system.
Method We modelled a system with a use case approach using Unified Modelling Language to enable us to design a method of producing the required report. Anonymised PGD are downloaded from a third-party telehealth system to National Health Service (NHS) systems and linked to the patient record available in the hospital recording system using the patient NHS ID through an interface accessed by healthcare professionals. The telehealth data are then processed into a report using the patient record. This report summarises the readings in graphical and tabular form with an average calculated and with a recommended follow-up suggested if required. The report is then disseminated to general practitioner practices through routine document distribution pathways.
Results This addition to the telehealth system is viewed positively by clinicians. It has helped to greatly increase the number of general practices using telemonitoring to manage blood pressure in NHS Lothian.
- telehealth
- eHealth
- medical records
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Despite increasing evidence from clinical trials for the effectiveness of telemonitoring in long-term condition management, attempts to scale up its implementation have proved less successful than initially anticipated.1 One factor is resistance from clinicians because of perceived increases to workload.2,3 It is recognised that to overcome any reluctance to adopt telehealth systems it is important that the usability of the telemonitoring system is paramount and it is essential to ensure that the system will be successfully integrated into normal working patterns.4 A recurring issue has been the inability to integrate telehealth patient generated data (PGD) into the electronic medical record (EMR) of family physicians,5–7 and this has been identified as an issue that potentially determines the success and future of telehealth.8
Telehealth record data are usually stored on a separate website from the patient record, which necessitates additional security logons and, in some cases, the double entry of data which can result in lengthening of the consultation and possibly introducing data security issues.9 For telehealth systems to work smoothly, all clinicians within a practice need to access the readings summary without the requirement to access the separate telehealth website. This has not been easy to achieve because of data protection concerns about recording identifiable patient data on third-party systems and a lack of standardisation in health record systems which have prevented seamless integration of the recording systems.
THE SCALE-UP BP PROJECT
Following the success of a local randomised controlled trial,10 the Technology Enabled Care Programme11 aims to introduce telemonitoring at scale for blood pressure (BP) in Scotland. Scale-up BP is part of this programme and is implementing home monitoring of BP with telehealth in general practices in Lothian. The telehealth system used12 involves the patient texting their home BP reading to a mobile number to enable the readings to be sent by Short Message Service to a telehealth server. Patients are informed by text at the time of the reading if the BP is within target and depending on the level may be directed to contact their doctor routinely or urgently. The data are displayed on the patient’s nurse or general practitioner (GP) computer via a secure web server. Although this program summarises the readings in graphical and tabular form as well as displaying the complete set of readings, it has to be accessed through a website with a secure login and is not part of the general clinical system. This has caused difficulties in previous pilot studies of telehealth with some clinicians at a practice not being able to access the information.5,13
DEVELOPMENT OF A REPORT INTEGRATED WITH THE ELECTRONIC MEDICAL RECORD
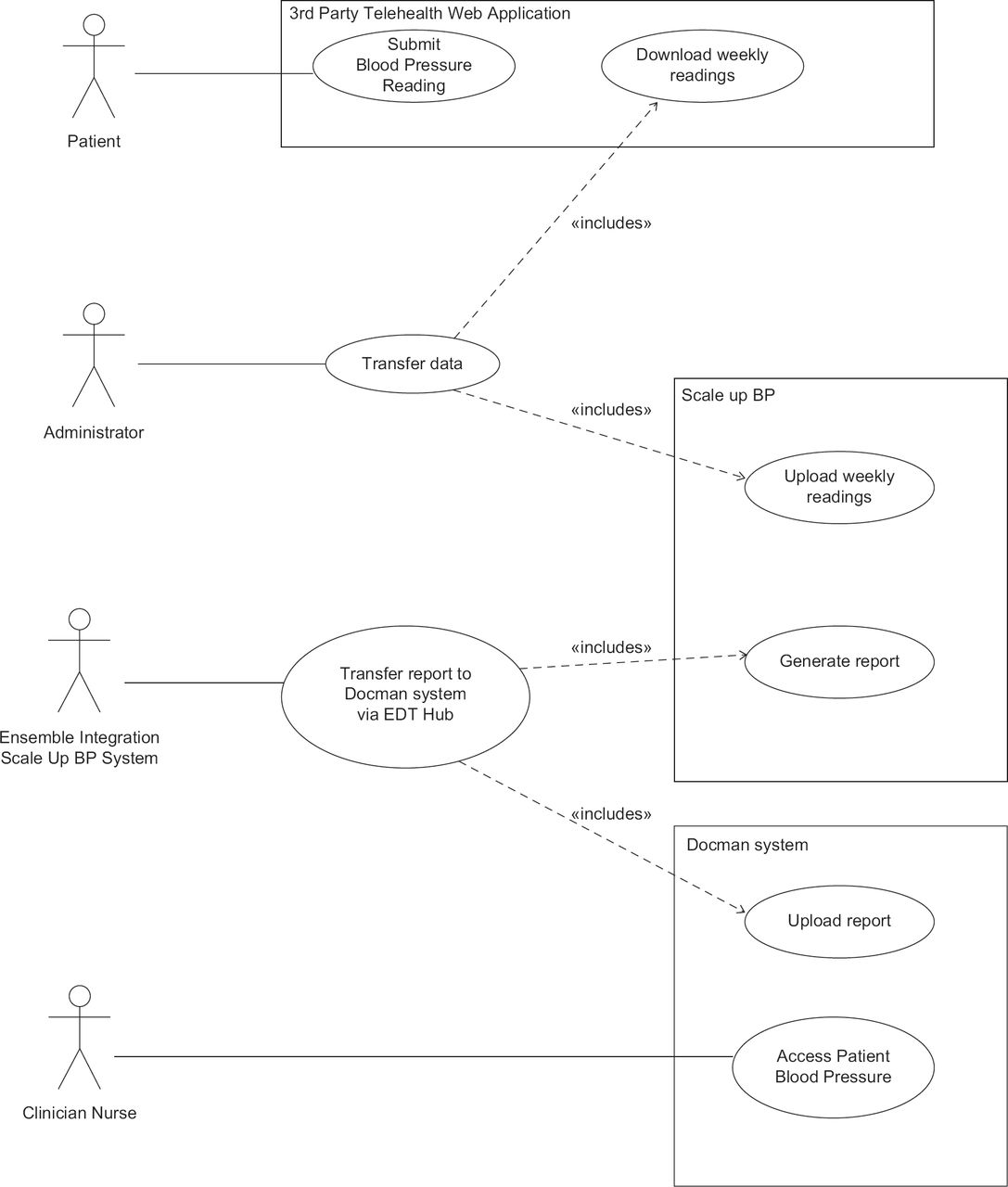
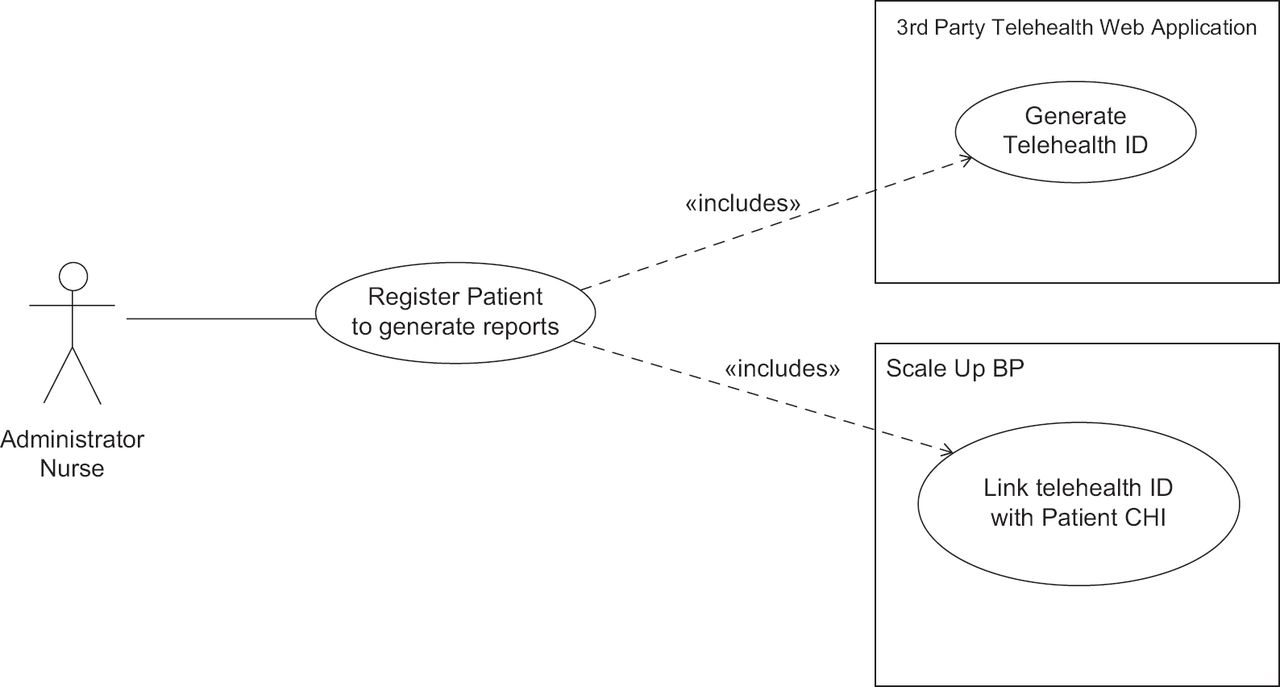
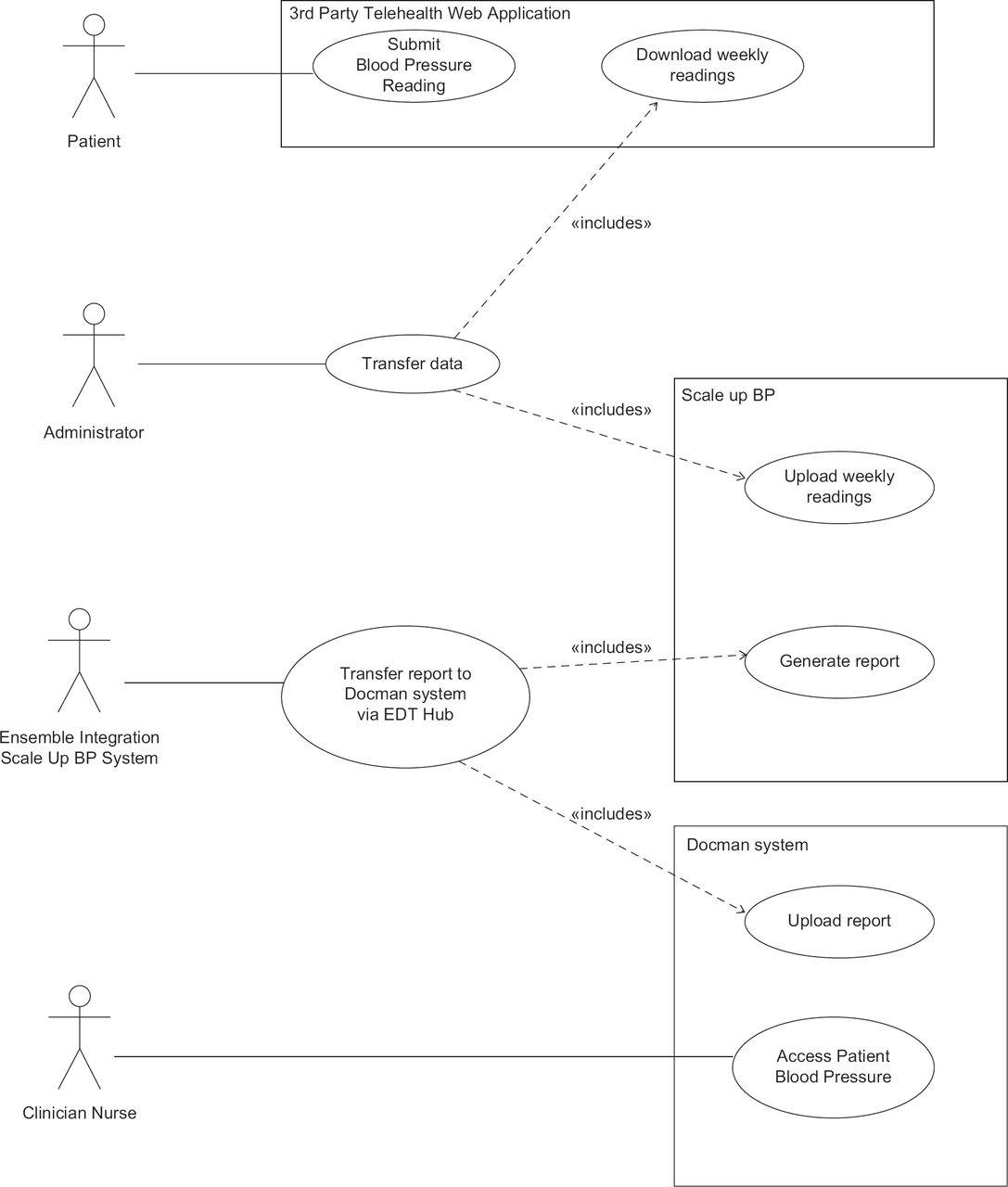
The Scale-up BP project included a proposal to establish a clinically appropriate, safe, and effective method that integrates PGD into the EMR in a summarised form. In our previous study,13 we investigated the issues of integrating telehealth data into the general practice reporting system and clinicians’ preferred format of receiving this. Clinicians wanted a system that was simple, compatible with the existing EMR system and to provide regular information summaries. Moreover, the data flows should be normalised to closely resemble existing incoming data flows and include a mechanism to feedback information to other care team members (as per usual practice routines). Graphical presentation and the use of colour were seen as helpful to summarise data over an agreed time period and indicate abnormal data parameters with access to the full dataset from the summary chart. Taking these suggestions into account, we developed a model with a use case approach using Unified Modelling Language14 that described the interaction of the key actors in the system (Figures 1 and 2). The model shows the actors involved in the process interacting with the system to complete tasks along with the functional requirements and goal (the report) giving a schematic overview of the systems required. Figure 1 shows the initial interactions needed, and Figure 2 shows the report production process. Software was developed by the Scale-up BP project team based on this model which allowed the summarisation and transmission to GP practices of patient generated BP measurements using routine information flow channels, currently used for reviewing laboratory results and hospital letters, thus avoiding the necessity for clinicians to use two logins to review the readings, one for the telehealth website and one for EMR. We decided to use a routine reporting system rather than attempting to link the PGD directly with the EMR as data directly entering the patient record in the latter way would bypass the normal reviewing mechanisms currently in place in GP practices. All incoming summary reports are reviewed by clinicians as they do for routine laboratory results and can be acted on as required.
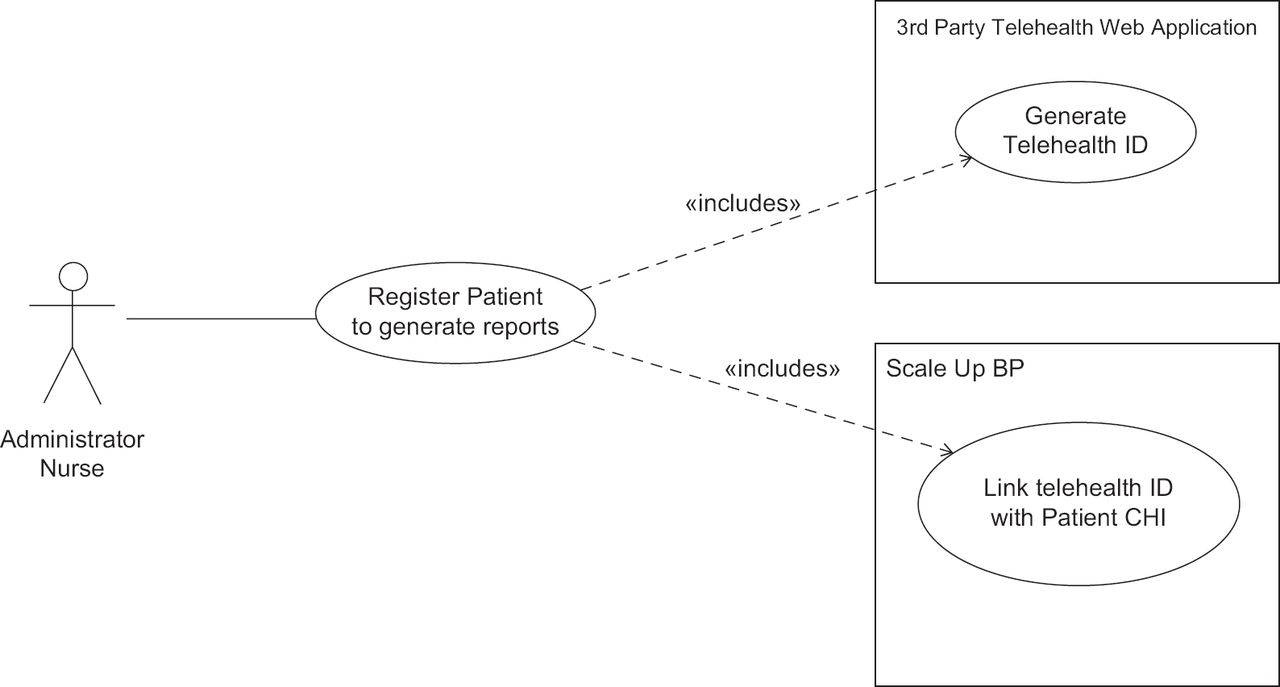
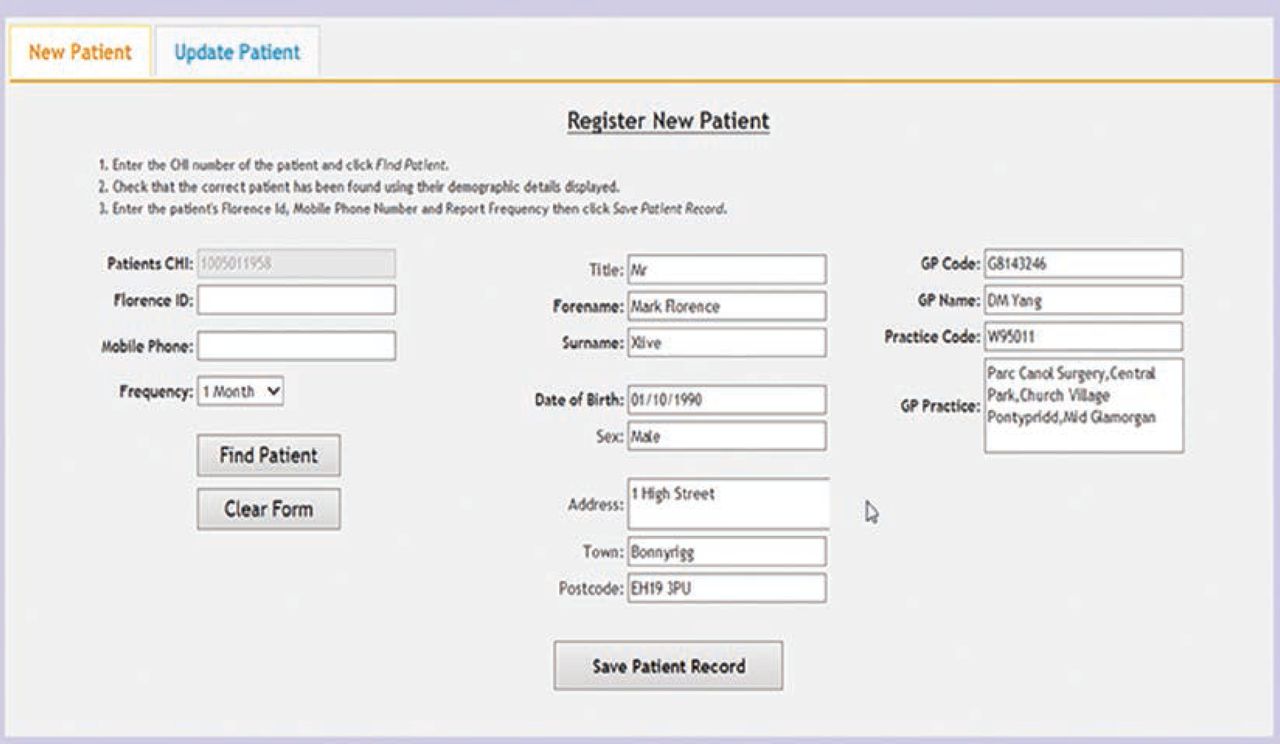
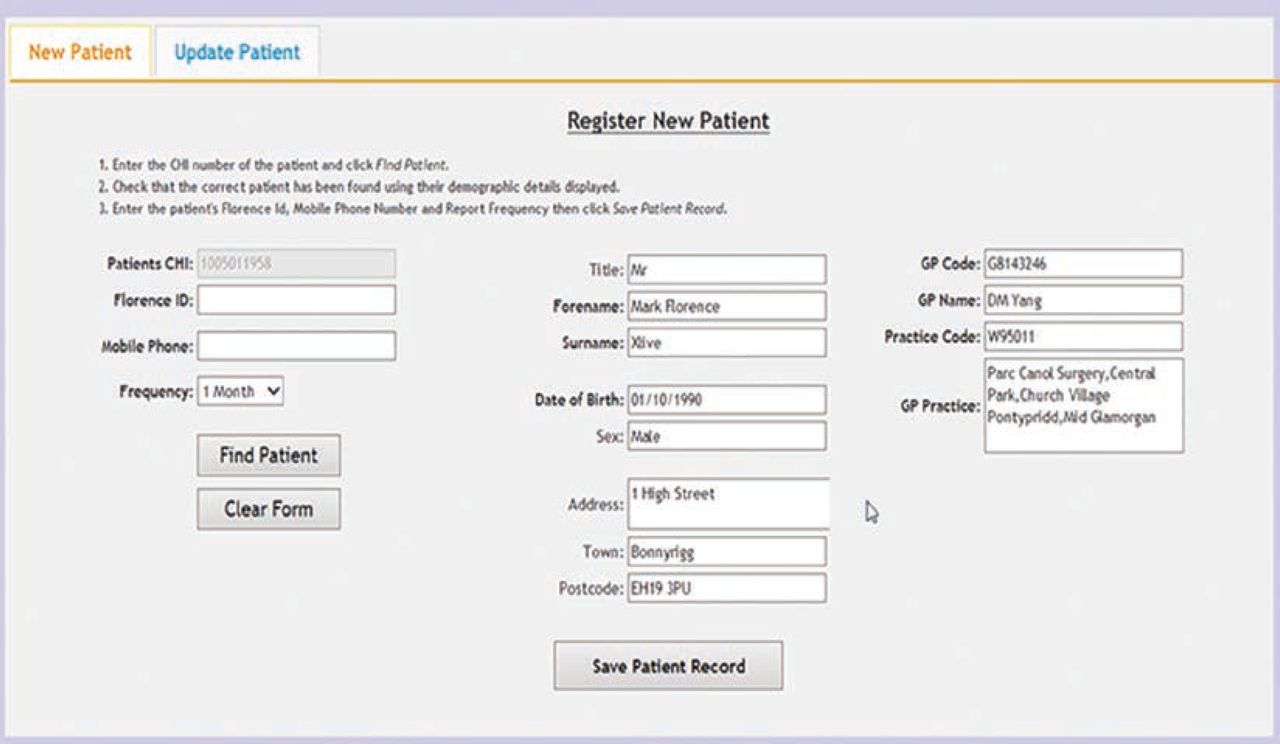
Information governance restrictions meant that it was not permitted to store the unique patient identifier, the Community Health Index (CHI) number, which is allocated to all patients in the NHS in Scotland and used for interactions in the Scottish health service, on the third-party (Florence)12 system so it was not possible to link the telehealth records to GP records directly. This problem has been overcome by developing a simple web interface within the NHS network where, at the time of registering on the telehealth system, the clinician looks up the NHS patient hospital management system (TrakCare from Intersystems)15 to select the correct patient using the CHI number. The patient’s demographic details including the GP practice are retrieved and checked. The clinician then records the unique telehealth ID assigned when the patient is registered on the telehealth system and enters whether to receive reports on a monthly, three-monthly or six-monthly basis.
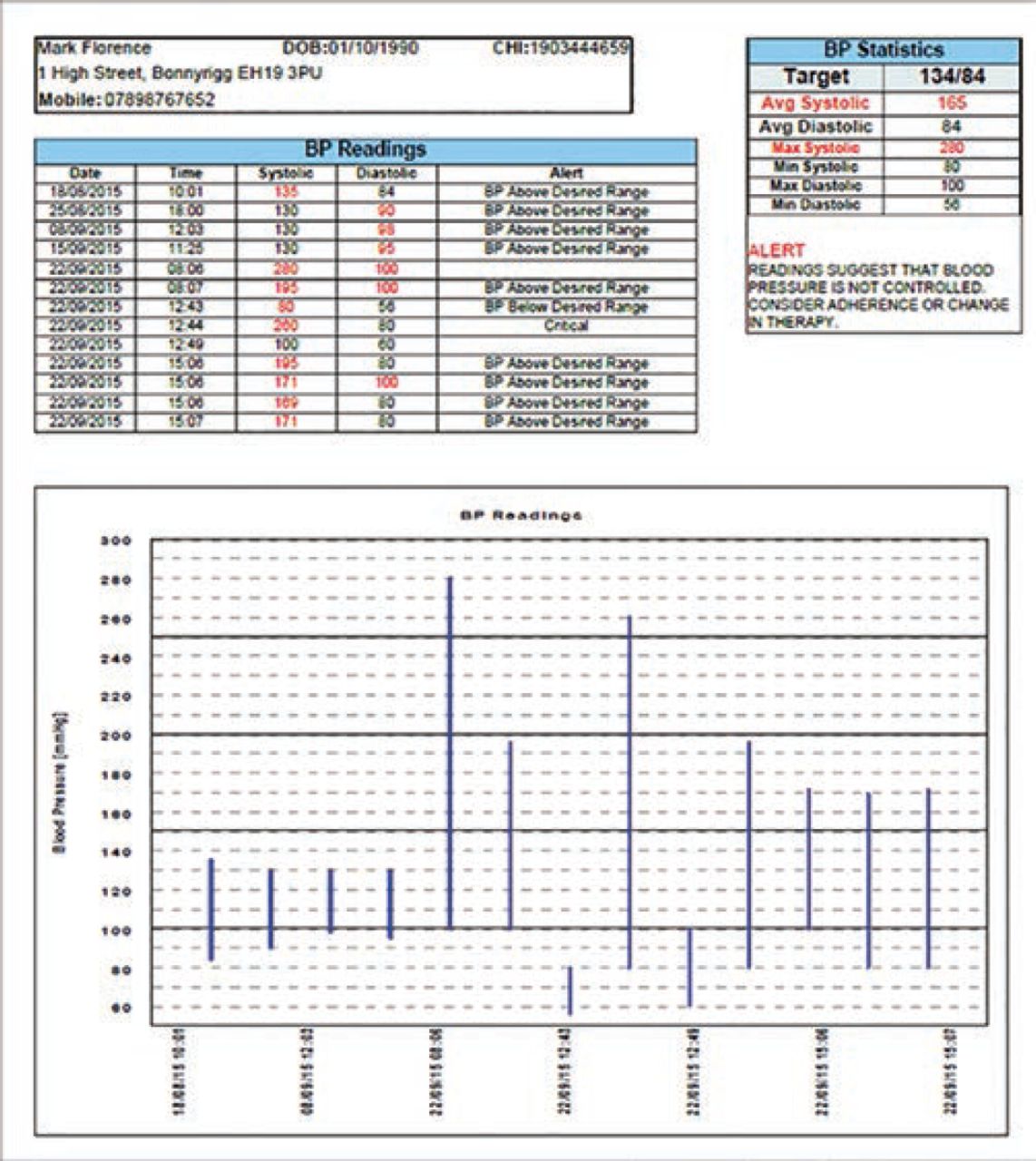
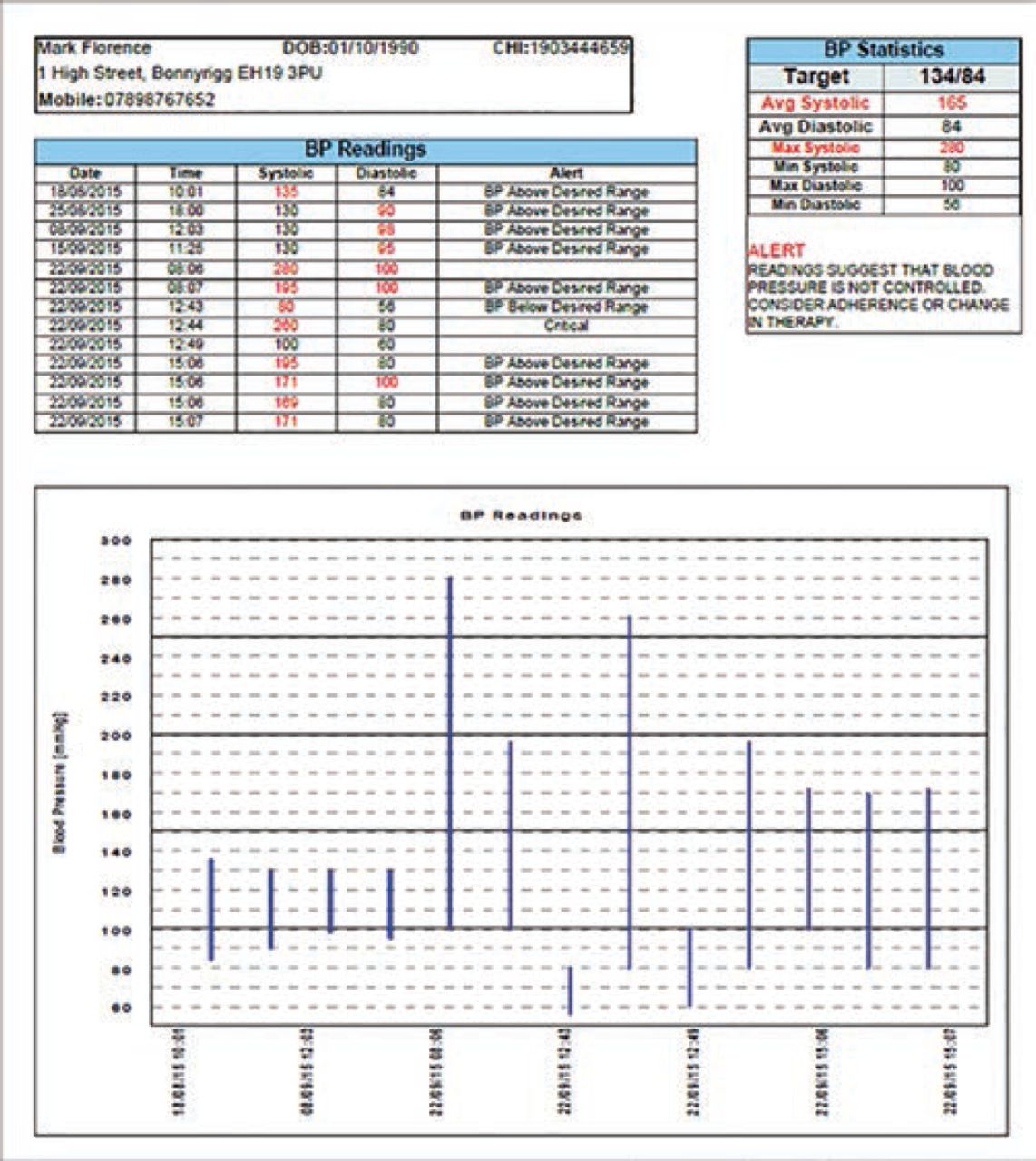
The anonymised telehealth data (with an ID only) are downloaded weekly from the third-party system to create the reports. Each record in the manual data extract is added to InterSystems Ensemble that allows for the development of new connectable applications. Scheduled tasks automate both the generation of a PDF graph and the sending of the report to the Electronic Document Transfer Hub for transmission to the GP practices using metadata that identifies the GP practice and matching it to its corresponding CHI number and reporting interval. The demographic and telehealth data for each patient are assembled into the Portable Document Format (PDF) report that displays the BP readings over the desired period graphically and in tabular form. It highlights those readings that are above or below target. The targets are set in the telehealth programme and follow national guidelines16 for people with uncomplicated high BP and lower targets for those with chronic kidney disease or diabetes mellitus. The average systolic and diastolic pressure of the last five pressures during the chosen period are displayed and are highlighted if they are above or below target and trigger a statement saying ‘Readings suggest that BP is not controlled. Consider adherence or change in therapy’ (Figure 3).
Each report is pushed out through the Docman system,17 which is the most widely used document handling system in general practice and through which all hospital letters and laboratory results are managed, into the specified GP practice where it is assimilated into the normal electronic document handling processes. The reports are sent in a staggered way so that practices are not overwhelmed with a large number of results in one day. An algorithm, based on the day of the month that the patient started to use the telehealth system, decides which reports to send.
APPLICATION
Tests using dummy data were run before the live roll out. The report-based system was tested on seven early adopter practices in the project, initially with monthly reports. Clinicians found the system easy to use and reports were received as requested. The feedback on the layout of the report was favourable; the reports summarising the readings graphically and in a table with the average calculated were found to support and enhance clinical decision making. Occasionally, a patient is not recorded on the hospital management system because they have not had contact with a hospital and, hence, no record exists. Links with the Medical Health Records Department have had to be established to resolve this issue.
Nurses request a login to the patient registration system from central NHS Lothian IT services. The link to the registration webpage is easily accessed on the commonly used intranet applications list. The nurse enters the patient’s CHI number, the patient details displayed are checked and the telehealth ID from the telehealth system is added (Figure 4). This routine task can also be completed by an administrator in the GP practice to save clinician time. The reports are handled by GP practices following standard document handling procedures; all are checked, the average transferred into the patient notes and the document is then stored in the EMR and thus the information is accessible to all clinicians at the practice.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The system has now been rolled out to all practices taking part in the scale-up BP project. The project has proven very popular with almost half of GP practices in Lothian taking part in the scheme and currently 1200 patients have been recruited.
Discussion
A system that has integrated the telehealth data directly into the EMR system has proved successful. The integrated reporting system is viewed very positively and is an important factor in persuading practices to take up the telehealth service. This method has addressed security concerns by keeping all NHS patient identifiers within the NHS. The report has also matched the suggested requirements in the Davidson paper.13 The PGD are received by practices through routine information routes ensuring that it does not overwhelm the clinician with frequent unscheduled data. A facility to review discrete data in PDF reports through the routine documentation handling process is seen as a positive attribute of our method. Real-time reception of data by clinicians is available in the telehealth system, but is not a factor that is seen as essential in a condition such as hypertension. A review of evidence for mHealth1 recommends interventions should be guided by a plausible theory of behaviour change. We have found that ensuring there are very few changes in routine behaviour within the practices by using the document reporting process, improves the implementation rate of telehealth.
The existing process could be improved if the third-party supplier provided an application program interface to allow automated retrieval of the results. There is potential to store patients’ own results in the hospital TrakCare system and add value to consultations outside the primary care setting. The system has the possibility to be extended for use with other conditions and data types. We are also negotiating links to existing patient-facing portals operated within the NHS to increase its scope.
Acknowledgments
Thanks to Arek Makarenko, Daniel Plenderleith and Mark Pearson for providing help in developing the system.