Article Text

Abstract
Background/aims To assess the outcomes of home monitoring of distortion caused by macular diseases using a smartphone-based application (app), and to examine them with hospital-based assessments of visual acuity (VA), optical coherence tomography-derived central macular thickness (CMT) and the requirement of intravitreal injection therapy.
Design Observational study with retrospective analysis of data.
Methods Participants were trained in the correct use of the app (Alleye, Oculocare, Zurich, Switzerland) in person or by using video and telephone consultations. Automated threshold-based alerts were communicated based on a traffic light system. A ‘threshold alarm’ was defined as three consecutive ‘red’ scores, and turned into a ‘persistent alarm’ if present for greater than a 7-day period. Changes of VA and CMT, and the requirement for intravitreal therapy after an alarm were examined.
Results 245 patients performing a total of 11 592 tests (mean 46.9 tests per user) were included and 85 eyes (164 alarms) examined. Mean drop in VA from baseline was −4.23 letters (95% CI: −6.24 to −2.22; p<0.001) and mean increase in CMT was 29.5 µm (95% CI: −0.08 to 59.13; p=0.051). Sixty-six eyes (78.5%) producing alarms either had a drop in VA, increase in CMT or both and 60.0% received an injection. Eyes with persistent alarms had a greater loss of VA, −4.79 letters (95% CI: −6.73 to −2.85; p<0.001) or greater increase in CMT, +87.8 µm (95% CI: 5.2 to 170.4; p=0.038).
Conclusion Smartphone-based self-tests for macular disease may serve as reliable indicators for the worsening of pathology and the need for treatment.
- COVID-19
- health care sector
- patient care
- information management
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
What is already known?
Avoidable harm may ensue from delays to ophthalmic care.
Self-testing and the remote monitoring of vision is gaining traction.
The Alleye app is accurate in detecting age-related macular degeneration.
What does this paper add?
The development of an Alleye alarm and their frequency of generation in patients with all causes of macula pathology provide a mechanism of alerting clinicians to worsening disease.
These alarms should prompt clinicians to consider expediting an in person review for patients with such pathology.
Introduction
In the ophthalmic realm, self-testing of vision enhances patient health empowerment with the added benefit of enabling the efficient use of hospital resources and improving access to treatment.
In recent years, several digital home vision tests have become available to patients with macula disease.1 Self-testing was first established in patients with age-related macular degeneration (AMD) using preferential hyperacuity perimetry on a standalone device (ForeseeHome, Notal Vision, United States), with a randomised trial demonstrating earlier detection of disease progression and lower reduction in visual acuity (VA) compared with standard care.2 Currently, there are two smartphone-based vision tests available for the remote monitoring of metamorphopsia in patients with macular pathology that are Food and Drug Administration 510(k) cleared and CE (European Conformity)—marked Class I device approved; myVisiontrack and Alleye (Oculocare, Switzerland). myVisiontrack uses a shape discrimination task examining 3° of the central visual field and the Alleye test a dot-alignment task covering 12° of the central visual field.3–5
In October 2019, the medical retina team at Moorfields Eye Hospital in South London first implemented the use of the Alleye app in patients receiving intravitreal therapy for macular disease who were undergoing extension of their treatment interval. Following the arrival of the global pandemic and the associated national lockdown in the UK from 23 March 2020, the challenge of providing a retinal therapy service in the COVID-19 era was created. At Moorfields Eye Hospital, ‘forward triage’ was used.6 Patients triaged to postponed appointments were invited to participate in remote monitoring of their vision.
In this paper, we studied the relationship between the frequency of Alleye alarms and the central macular thickness (CMT) and VA at subsequent follow-up, in addition to the need for intravitreal injection therapy following the easing of the lockdown restrictions.
Materials and methods
Patient enrolment
This study looked at patients recruited at two time periods: prior to the lockdown, from October 2019 to February 2020 and after the commencement of the lockdown in March 2020. Prior to the lockdown, patients with diabetic macular disease attending the medical retina injection clinics (in a face to face environment) were offered the option to use the Alleye application for home-monitoring of their vision and if they agreed, trained to use the app in person. Patients were advised that if an alarm was triggered, they would be contacted by the clinic team by telephone and given the option of bringing their appointment forward (shortening interval between clinic visits). Patients who did not own or have access to a smartphone were loaned a new iPod Touch (6th generation, Apple, Cupertino, California, USA) with the Alleye app pre-installed for their use. Each patient was given an anonymised identifier allowing their scores to be monitored remotely, and this remained underway until the commencement of the first UK lockdown in March 2020.
Home monitoring protocol
Following the Lockdown, patients who were triaged to ‘medium’ or ‘low’ risk and had their appointments deferred received a telephone call from the clinical team and were offered the opportunity for self-testing of their vision.6 Those who were willing to start the home monitoring were offered telephone or video training to use the app. All patients were asked to contact the clinical team by telephone if there were concerns, and were provided with an email to contact the clinical team directly with queries.
Patients’ scores were monitored weekly. A ‘threshold alarm’ was defined as three consecutive ‘red’ scores, defined as a ‘persistent alarm’ if present for a >7-day period. Patients who met this criterion of a persistent alarm were called by telephone by a clinician and asked if their vision was worse/better/unchanged. If worse, they were asked if they felt they needed an injection or that their vision was worse. If they answered in the affirmative, their appointment was expedited, within 1–2 weeks.
If once called the patient felt that their vision was unchanged or better, then they were asked to continue testing their vision using the app, and would be called again the following week if their scores remained in the ‘red’ zone. This was also the case for patients who did not answer the telephone, until they were seen face to face in the clinic. Any patients who discontinued testing following a threshold alarm being generated were also contacted by telephone.
Clinical characteristics
Baseline VA and the optical coherence tomography (OCT)-derived CMT in addition to medical retina diagnosis and laterality were recorded from the electronic medical record. Demographics were recorded in the way of age, gender and ethnicity. The first follow-up visit provided with a VA and OCT scan post threshold alarm was recorded for each patient that has had a face to face review since threshold alarm generation.
Statistical analysis
We summarised continuous variables with means and SD and dichotomous variables with percentages. We calculated changes of VA (Early Treatment of Diabetic Retinopathy Study letters) and CMT from baseline and tested differences statistically using one-sample t-tests, considering a p value <0.05 statistically significant. We plotted the occurrence of worsening of VA and CMT against the need for an injection. To assess selection patterns of enrolment before and during the lockdown, we compared clinical characteristics at baseline statistically. Analyses were performed using the Stata V.16.1 statistics software package (StataCorp)
Results
During the months of April and May 2020, 605 patients triaged as ‘low’ and ‘medium’ risk were contacted by telephone. Of these, 222 patients met the minimum VA criteria of 6/24 to participate and wished to be involved, being booked for subsequent appointments of training in the use of the application at a later date. Of these patients, 90 were onboarded via video consultation using the Attend Anywhere platform (Attend Anywhere, Victoria, Australia), and 60 were onboarded via telephone. The remainder of patients involved were recruited via technicians in virtual clinics and clinicians reviewing patients in a face to face environment, who were then contacted for a telephone training appointment at a later time. Details of the selection process are shown in the flowchart of figure 1.

Flowchart outlining patient recruitment for home monitoring of vision using the Alleye app. Patients were recruited either by telephone calls to those stratified as ‘low’ and ‘medium’ risk during the COVID-19 pandemic or in person when attending virtual clinics and face to face (F2F) clinic appointments. Following recruitment, patients were subsequently onboarded with the smartphone application via telephone or video consultation.
A total of 212 patients tested with Alleye over the first UK lockdown and performed 9938 test results, in addition to 33 patients with diabetic macular oedema, who had been using Alleye prior to the lockdown, generating 1654 test results. The baseline clinical characteristics did not differ between the two cohorts that were onboarded before and during the lockdown. The average number of tests performed per user was 46.9 tests. A threshold alarm was defined as three consecutive Alleye scores that are red on separate days, therefore signifying potential deterioration in the score. A persistent alarm was defined as a threshold alarm that continues to remain for 7 days. Over the period from 23 March 2020 to 11 August 2020, 98 eyes of 65 patients each developed a minimum of one ‘Alleye alarm’.
The total number of threshold alarms produced was 164. Of the 98 eyes producing alarms, follow-up data of 85 eyes were available. Of these 164, 30 persistent alarms were generated. The mean age of patients with alarms was 65.1 years (SD=11.1; range 41–90 years) and 56.2% were female. On clinical review, 28 eyes were considered worse, followed by 38 considered as stable, 12 eyes improved. Classification of seven eyes was missing. The summary of patients’ characteristics is available in table 1.
Patient characteristics of eyes triggering ‘threshold alarms’ (n=98)
The mean change in VA from baseline to follow-up post threshold alarm generation was −4.23 letters (95% CI: −6.24 to −2.22; p<0.001). The mean change in CMT was +29.5 µm (95% CI: −0.08 to 59.13; p=0.051). The mean number of alarms generated per patient was 1.67 (range 1–9). Based on the clinical assessment and the patients’ willingness to be treated, 51 eyes (60.0%) received an intravitreal injection, 29 eyes received no injection, 3 eyes had a contra-indication for treatment and 2 eyes were not treated because the patients declined injection. Sixty-six eyes (78.5%) producing alarms either had a drop in VA, increase in CMT or both (figure 2).

Distribution of changes of visual acuity and central macular thickness (CMT) for patients at the next follow-up visit after triggering ‘threshold alarms’ (n=84) and whether intravitreal injections were received in these patients or not.
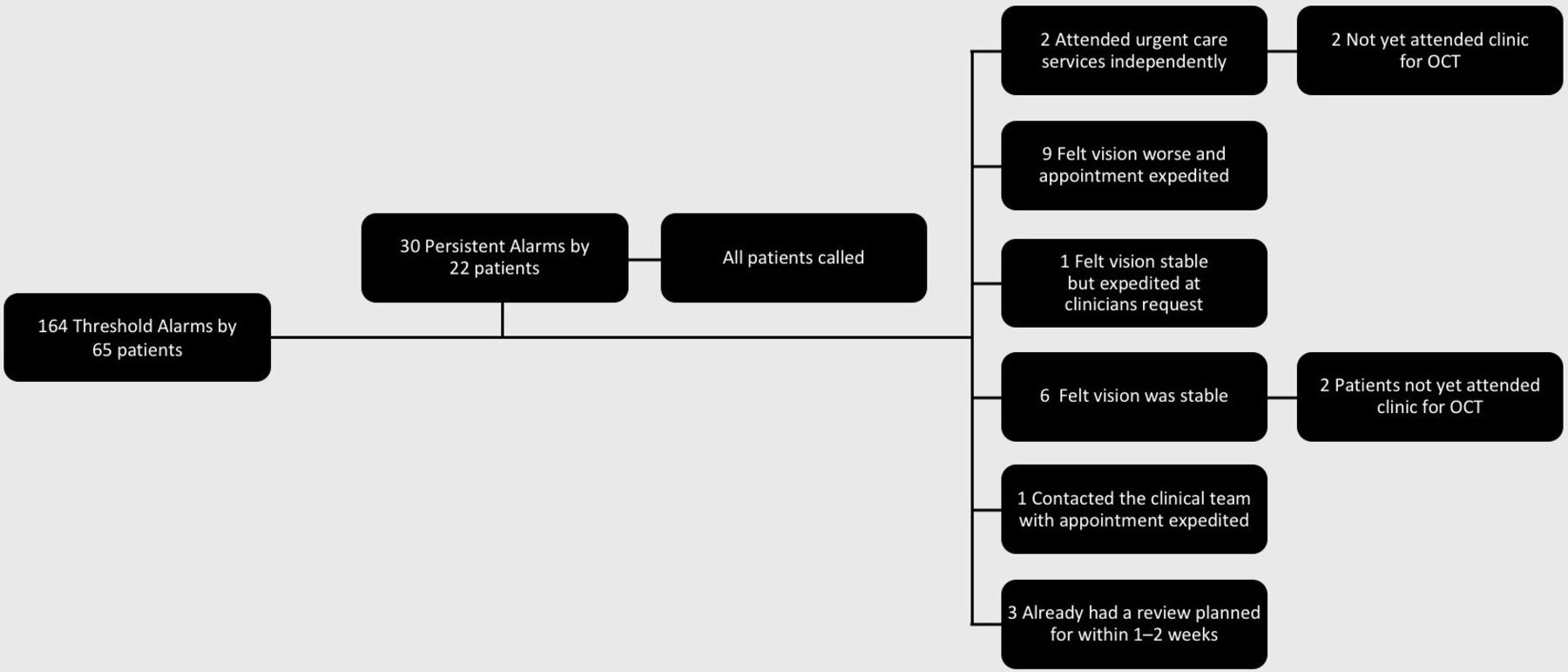
The 30 persistent alarms were generated by 24 eyes (22 patients). VA dropped by −4.79 letters (95% CI: −6.73 to −2.85; p<0.001) and CMT increased by +87.8 µm (95% CI: 5.2 to 170.4; p=0.038) in this group of patients. Injections were provided in 20/24 eyes (83.3%). Compared with the group with threshold alarms, the likelihood for an injection was significantly higher (p=0.034). The patient flow outcomes for these patients are demonstrated in figure 3.

{kind=link}
{kind=link}
{kind=link}
Flow of patient of outcomes after triggering a ‘persistent alarms’. OCT, optical coherence tomography.
Eyes considered to have worsened since the last clinical review had a higher probability of receiving an injection (89.3%) than stable (42.1%) or improved (66.7%) eyes. Similarly, eyes showing a worsening in the follow-up visit had a higher drop in VA (−8.4 letters (SD 8.8)) than stable (−2.3 letters (SD 9.6)) or improved (−3.0 (SD 8.4)) eyes. In addition, CMT increases were highest in those eyes classified as worse (+116.9 µm (SD 144.8)), while stable (−17.4 µm (SD 51.2)) and improved (−18.1 µm (SD 206.3)) eyes had a slightly lower CMT than before the lockdown.
Discussion
Main findings
Due to the exceptional circumstances during the lockdown, we were able to study the consequences of delayed treatment and the relationship between changes of the Alleye signal and clinical parameters in the absence of any treatment. We demonstrated a close relationship between the frequency of the Alleye alarms and the subsequent deterioration of macular disease coupled with the need for intravitreal injection therapy. Four out of five patients presenting with alarms showed signs of clinical progression and two out of three patients required immediate intravitreal therapy. Figure 3 flowchart demonstrates the outcomes of those patients generating persistent alarms.
Results in context of the existing literature
Macular disease can affect individuals of all ages and is particularly debilitating as it affects central vision. Nearly 1.5 million people in the UK have macular disease.7 Self-monitoring of vision for macular disease is an area gaining significant traction, fuelled by clinical needs, service requirements and patient interest.1 The WHO has identified ‘self-care’ as a key health topic and defines it as the ability of individuals, families and communities to promote health, prevent disease, maintain health and cope with illness and disability with or without the support of a health worker.8 The WHO further advocates evidence-based digital technologies and mHealth approaches which can be accessed fully or partially outside of formal health services. Within the UK, there is an increasing backlog of routine appointments as a direct consequence of the COVID-19 pandemic.9 This is due to the postponement of clinical reviews following clinical triage resulting from the need to reduce face to face contact during the peak of the pandemic.10 The literature so far discussed the immediate challenges for the management of glaucoma.11 12 However, even prior to this, ophthalmology as a specialty was well on its way to buckling under the strain applied by our National Health Service.13 It has been known for several years that ophthalmology is the busiest outpatient specialty in the UK, with an estimated 30%–40% of increased demand over the next two decades.14 A combination of workforce shortages, clinic space and increasing healthcare requirements for an ageing population has resulted in health-service initiated delays, demonstrated by the RCOphth and British Ophthalmological Surveillance Unit to be resulting in permanent and severe visual loss for our patients.15
It is therefore of benefit to patients and doctors to avoid unnecessary in person hospital appointments that have direct impacts on waiting lists for others. It is also worth sparing a thought for the stable patient, attending hospital for a clinical review that is not required. This is a waste of resources for both the patient and hospital, and a source of potential unnecessary anxiety generated for an individual, which must not be underestimated. Conversely, there will be many patients in the community waiting for their first hospital appointment with long delays, with potential avoidable harm incurred.16 Prior to this study, it had been demonstrated that Alleye was highly accurate in detecting wet AMD.4 5 This is the first study of its kind observing all patients with known macula pathology.
Strengths and limitations
This study was conducted using a pragmatic approach, which we recognise as both a strength using a real-world approach, and as a potential limitation. Due to the lockdown, the onboarding of patients using video and telephone consultations was necessary. Therefore, it cannot be entirely ensured that the information and instructions provided to the patients was always understood to the desired degree. In addition, regular patient contact was not feasible and an inherent assumption was made that patients would adhere to our testing recommendations. Finally, due to the backlog of patients requiring hospital visits following the easing of the lockdown restrictions, a few of the patients with Alleye alarms had not yet returned for a clinical follow-up before writing up this paper, precluding the collection of the results of all threshold alarms. Using video and telephone consultations, we maintained what we felt was an appropriate level of contact and were able to successfully triage patients requiring a hospital visit. Inevitably, some delays may have occurred due to natural concerns from patients who were reluctant to attend hospital due to the risk of catching COVID-19, and these patients may have returned for later reviews to the hospital despite Alleye threshold alarms, however, no patients voiced a deterioration of vision at the same time as a direct reluctance to attend. If advised, all patients attended for earlier review. Delays in returning to the hospital may have contributed to disease progression resulting in a positive correlation between occurrence or frequency of Alleye alarms and the likelihood of the evidence of clinical signs of progression in the follow-up visit.
Implications for research
These results provide promise for the future directions of research for remote monitoring of vision in the context of macular disease.6 17–19 Future studies should focus on the false negative rate of Alleye, that is, those patients returning at follow-up post lockdown whose clinical parameters have deteriorated, but did not trigger a threshold Alleye alarm. Moreover, our observation that patients with persistent alarms had a higher likelihood for progression and subsequently required intravitreal injections could be further explored. Our data suggest that changing the policy of alarm management could have an impact on the specificity of the alarm signal. If confirmed, healthcare providers could easily adapt the management based on Alleye alarms according to their local requirements and service capacities. While the sensitivity of Alleye in the screening setting has been assessed before,4 5 sensitivity and positive predictive values in the monitoring situation still need confirmation. Another stream of research should assess the impact of home monitoring in conjunction with telemedicine to increase the efficiency of care delivery and the monetary impact of home monitoring on health service cost. While there is some indication from other clinical fields that remote management of chronic diseases is cost-beneficial,20 21 robust evidence in the field of ophthalmology is limited. Finally, with view to the drug pipeline extended release applications, the value of home monitoring to support patient management between reviews should be assessed, as the prolongation of intervals between face to face visits bears the risk of missing deterioration.
Implications for practice
Telemedicine in ophthalmology has been steadily gaining traction over the last few years. Increasingly, time is far more binary, categorised into the ‘Pre-COVID-19’ and the ‘Post COVID-19’ era.10 People often talk of a ‘new normal’. It is important to recognise that an effective, efficient and safe telemedicine programme cannot be implemented overnight. It is imperative that for technological solutions to have longevity that they harness systems and procedures that are already in place.22 For self-testing and home monitoring to be incorporated into routine clinical practice, it requires a network of ophthalmic technicians, nurses and clinicians to support its use. If incorporated into routine care, particularly in an era where face to face review is the exception and not the rule, we could move towards our ultimate aim of ensuring the right patient is seen at the right time. We are still at the precipice of decentralised care for retinal diseases. In addition to the monitoring of functional limitations by Alleye, morphological examination methods using mobile OCT devices will soon be available.23 This provides exciting potential for the exploration of the interaction between function and morphology to strengthen the informative value of home measurements.
Conclusion
Our work illustrates that Alleye alarms and their frequency act as reliable indicators for worsening of macula pathology, and should prompt clinicians to consider expediting such patients’ face to face clinical reviews. We are at the beginning of a new era of medical care, in which valid clinical data from patients staying at home will be available in real time and can be included in the decision-making process of the need for on-site clinical visits. The ecosystem of digital developments is only just beginning. We envision a future in which the interaction of integrated digital solutions will have a major impact on the way healthcare is organised for chronic eye diseases.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Ethics approval
The research described adhered to the tenets of the Declaration of Helsinki and this study was registered under the Digital Clinical Laboratory and Audit department of Moorfields Eye Hospital NHS Foundation Trust as part of a service improvement project. All patients included as part of routine clinical care gave their informed consent by accepting the user agreement within the app during sign up, which allowed the use of their anonymised data for this analysis. Data for this analysis were obtained from a review of the electronic medical records from these patients.
Footnotes
Twitter @pbmthomas, @medignition, @dawnasim
Contributors DAS, MI and LMB provided substantial contributions to the conception and design of the work. MI, DAS, SS, RD, ML conducted the acquisition of the data. DAS, MI and LMB were involved in the drafting the initial manuscript and revising it critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LMB is a founding member of Oculocare Medical, which develops innovative products in eye care, such as the self-monitoring test described in this paper.
Provenance and peer review Not commissioned; externally peer reviewed.