Article Text

Abstract
Objective The term health information exchange (HIE) is often used in health informatics, yet uncertainties remain about its precise meaning. This scoping review aimed to capture and analyse existing definitions in order to map variations in the use of this term and the concepts associated with it.
Methods Systematic literature search to identify published definitions of HIE and related terms. Medline, Web of Science, Library Information Science and Technology Abstracts, EMBASE and CINAHL Plus were searched to identify relevant papers, and Google to identify grey literature. Searches were not limited by language or date of publication. Both explicit and equivalent conceptual definitions were included. Included definitions were summarised and thematically analysed in order to identify and map the underpinning constructs.
Results Our searches revealed 603 scientific articles and 5981 website links. From these, a total of 268 unique definitions of HIE were identified and extracted: 103 from scientific databases and 165 from Google. Eleven constructs emerged from the thematic analysis. Contextual factors influenced the emphasis of the definitions and the overall framing of HIE as an organisational entity that facilitates and or as a process of sharing health information between diverse stakeholders.
Conclusions HIE is a complex and evolving construct, for which multiple definitions exist. In order to encourage consensus, the authors propose this broad definition, which encompasses the key attributes of HIE described in the literature: “HIE is the electronic mobilisation of clinical and administrative information within or across organisations in a region or community and, potentially, internationally between various systems according to locally and/or nationally recognised standards while maintaining the authenticity and accuracy of the information being exchanged, enabling stakeholders to make informed decisions to enhance healthcare quality of a patient and population. HIEs are multi-stakeholder organisations that oversee the business, operational and legal issues involved in the exchange of information.”
- eHealth
- health informatics
- health information exchange
- scoping review
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Effectively delivering integrated patient care and business transactions within the healthcare ecosystem requires the exchange of patient-related data between stakeholders within and across organisations, in order to support clinical decision making and organisational functions such an insurer reimbursement.1 The process of transferring or sharing this information using information and communications technologies is often referred to as electronic health information exchange (HIE).2,3
Much of the current narrative around HIE has been centred around the United States (US) policy context, arising from the Health Information Technology for Economic and Clinical Health (HITECH) Act. This aims to improve the efficiency, consistency, safety and equity of healthcare services through better information sharing between relevant stakeholders, contingent upon the ‘meaningful use’ of electronic health records (EHRs), and is backed by a programme of financial incentives and penalties to encourage change.4,5 These developments have drawn particular attention to HIE in the US, although the same activities are being undertaken internationally. The screenshot in Figure 1 shows the number of global Google searches, since 2004, for the specific term ‘HIE’ (lower line) and the topic more generally, which is computed from several indicators (upper line).
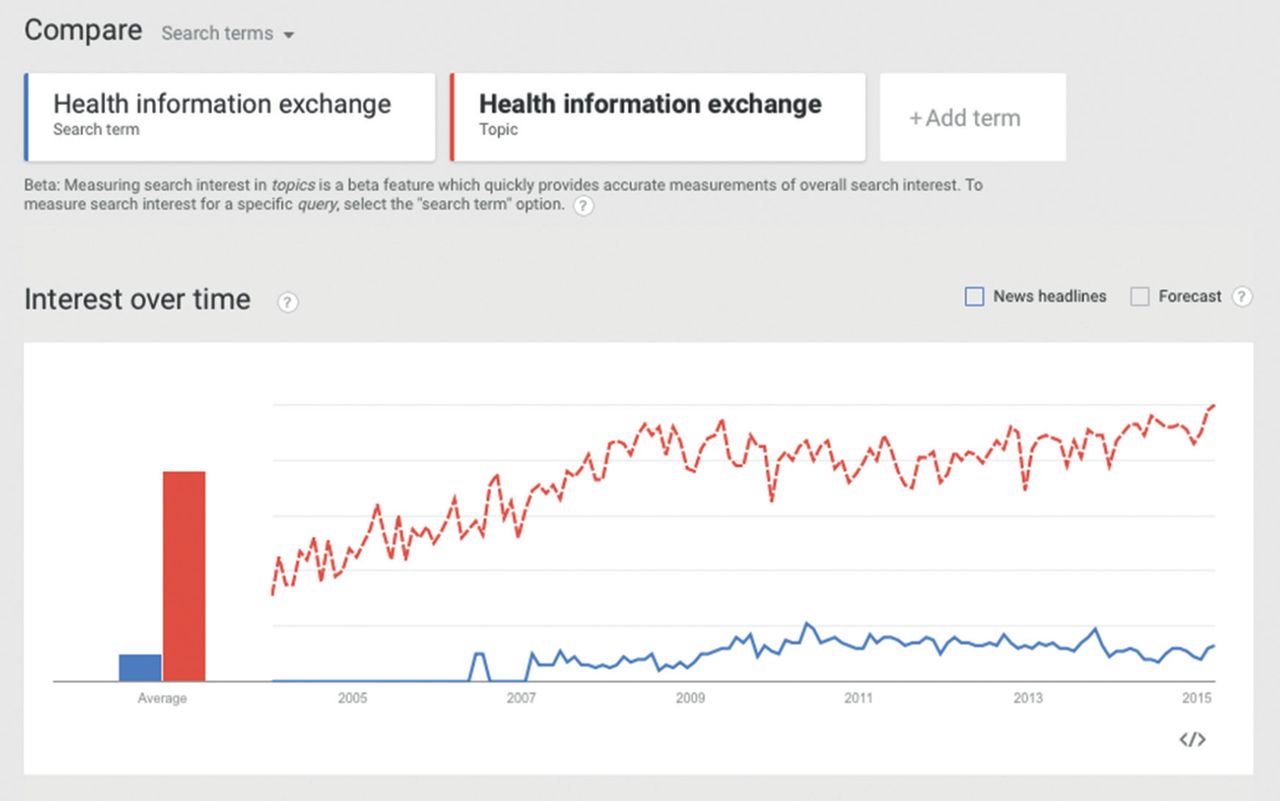
Much of the web traffic shown in Figure 1 is driven from the US and closely reflects the ‘meaningful use’ agenda, which has important but somewhat different implications for clinicians, healthcare delivery organisations, insurers and healthcare information technology providers. It also reflects the explicit use of the search term ‘HIE’, which is close-coupled with the US policy and business environment.
Although the term HIE is widely used, the way in which it is used varies in significant ways across stakeholders and contexts, including policymakers, academic institutions, professional organisations and funding bodies. Examples of diversity include ‘occupational’ HIE,4 HIE as a feature of the EHR5 and HIE as a corporate network of data warehouses serving a health organisation.6 This raises the potential for ambiguous or inconsistent definitions to hinder meaningful dialogue around health informatics policy, research and practice. For this reason, we decided to undertake a detailed scoping review in order to analyse the ways in which the term is being interpreted in the literature and how these vary across different organisations and contexts. The research therefore set out to answer the question “What is HIE?” with reference to the ways in which it has been defined and the concepts underpinning these definitions. The approach was inspired by earlier scoping reviews of eHealth7,8 and aimed to clarify the different uses of the term to in order aid the sharing of information about HIE across stakeholders and inform emerging taxonomies in health informatics.9,10
METHODS
Design
Systematic scoping review of the published and grey literature.11
Inclusion criteria
Definitions appearing in print or digital format were searched that explicitly refer to HIE or equivalent terms such as clinical information exchange and healthcare information exchange, as well as related concepts such as electronic data interchange (EDI). ‘Definition’ was taken to include explicit statements of the meaning of the term with reference to key concepts (e.g. ‘HIE is the movement of patient information across nodes of a health system using health information technologies and standards for data exchange’) and conceptual definitions, in the form of functional descriptions of HIE (e.g. ‘organisations exchange health information using middleware systems and interoperability standards such as HL7’).
Exclusion criteria
References to HIE not accompanied by either an explicit or an implied definition (as above) were excluded.
Search strategy
Searches were not limited by language. The searches covered the period from 1900 to February 2014.
Web searches: AA and CP first conducted a Google search using the narrative terms shown in Table 1.
Scientific databases
The explicit search terms and structured queries shown in Table 2 were used to interrogate Medline; Web of Science; Library Information Science and Technology Abstracts; EMBASE; and CINAHL Plus. There was no medical subject heading (MeSH) term available for HIE, clinical information exchange or healthcare information exchange and hence the reliance on key words.
Query strings were adapted as necessary for each academic database and for the purposes of Google searching. Titles, abstracts and text of the citations identified in the academic database were independently reviewed by two authors (AA and CP) before articles were retrieved for further analysis. Any disagreements between the investigators were resolved by a third reviewer (AS).
Reference lists of the included articles were also scrutinised for any relevant sources and cited work. Websites included reports, encyclopaedias, dictionaries, blogs, hospitals, vendors, letters, presentations, documents, white papers, articles and references. Duplicate citations and definitions were excluded from the results.
Data extraction
Data extraction tables were prepared to include details of the definition, author, source, year and country of origin. Duplicates appearing in more than one database were excluded prior to further analysis.
Analysis
As this was a scoping review of definitions, rather than a systematic review of research evidence, analysis did not involve appraisal of study quality.8,12–14
All potentially relevant articles identified by the search were analysed by hand in order to determine whether they contained an explicit definition of the term or an equivalent conceptual definition. Definitions were descriptively analysed according to publication date, geographical origin, provenance, and terminology used. AA undertook a high-level pass through the data to create a draft coding framework, which was refined in consultation with CP before beginning the coding process.8,12 Definitions were then thematically analysed, with each definition coded according to its various qualitative attributes. The codes were iteratively adapted in order to achieve the best fit with the data, equivalent to qualitative research, where coding proceeds until the point of ‘saturation’ where no new codes were required to describe the data.
RESULTS
The Google search yielded 5981 Web pages referring to the term HIE, whilst the searches of scientific databases revealed 603 articles referring to HIE (see Figure 2). These were analysed in order to determine whether they contained an explicit or conceptual definition.

Table 3 shows the number of definitions (see also Appendix A) extracted from Google and scientific databases.
Definitions dated back to the year 1957.15 Definitions ranged in length from 1116 to 146 words.17 Most of the definitions were from the US. See Table 4 for the number of definitions from various countries and regions. Other terms closely related to HIE found were ‘electronic data interchange’,18–20 ‘clinical information exchange’,21–26 ‘clinical document exchange’,27 ‘clinical HIE’,28,29 ‘healthcare information exchange’,30–35 ‘medical data exchange’ 36 and ‘information exchange.’37
KEY THEMES IDENTIFIED
The objective of facilitating exchange of health information among different systems or stakeholders was represented in the majority of definitions (See Appendices A and B).
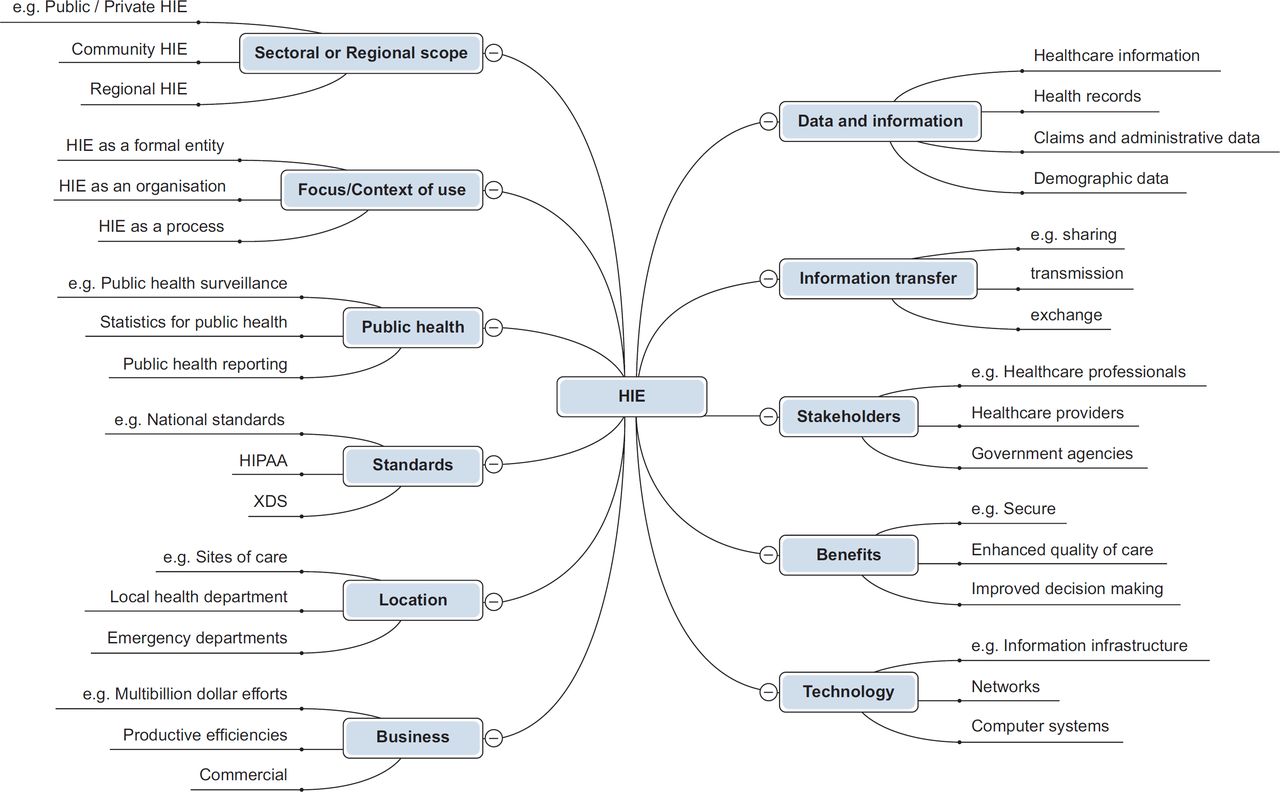
The analysis of the included definitions revealed 11 main conceptual themes. In Table 5, these are arranged according to their frequency in the corpus of included definitions, while Figure 3 represents them in terms of themes and sub-themes (not in the order of frequency). A more detailed breakdown of subthemes and their frequencies may be found in Appendix B.
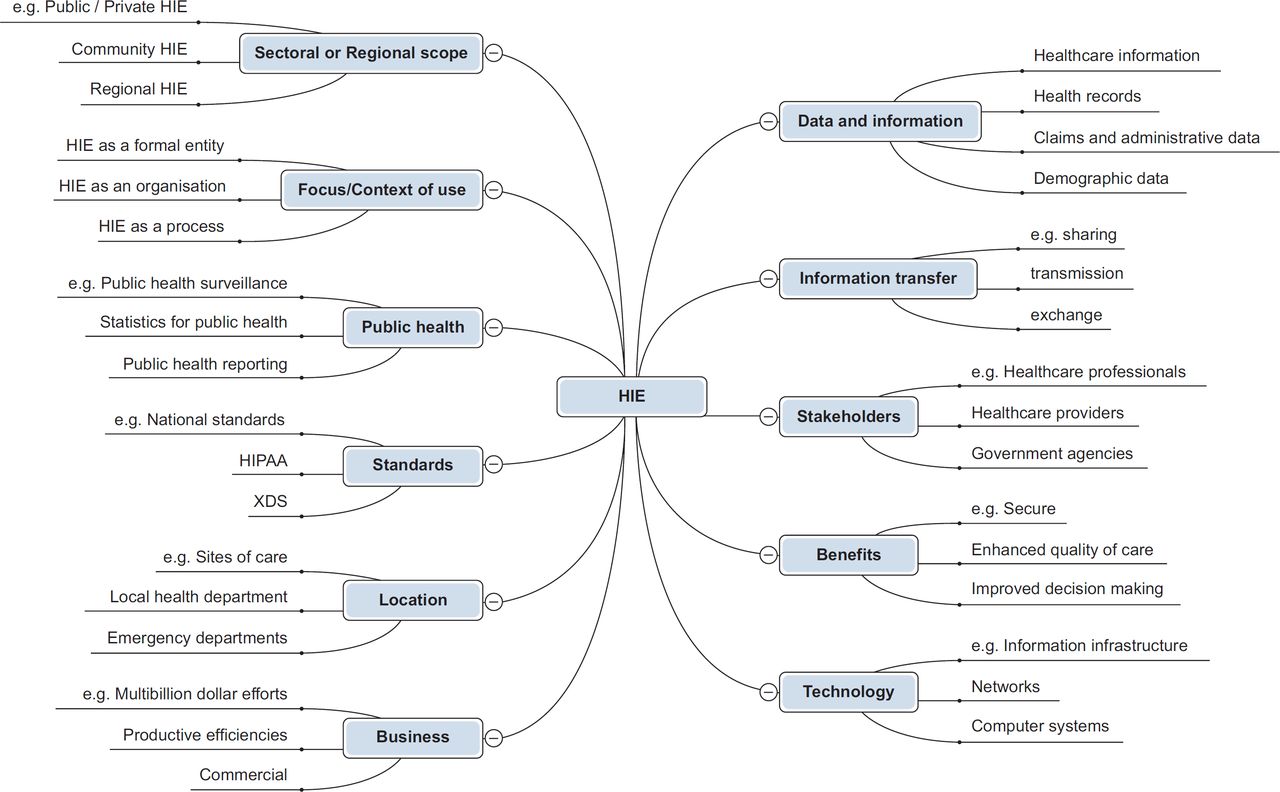
(Many definitions embedded a range of concepts and were thus tagged with more than one code or theme.)
The concepts represented within each higher order theme are described below.
Usage of data and information
The theme ‘data and information’ was divided into sub-categories that included ‘healthcare information’, ‘health records’, ‘claims and administrative’ and ‘demographic data.’
Health care information
Definitions referring to the types of information that could be shared, accessed or exchanged are given in Box 1.
Terms used to represent healthcare information
‘Health information’,2,5,45,49,54–98 ‘clinical information’,21,33,37,46,61,71,88,97,99–120 ‘clinical data’,23,30,33,87,110,111,121–131 ‘health data’,17,24,43,69,70,76,100,132-140 ‘patient data’,31,33,55,107,141–145 ‘healthcare information’,35,72,84,110,115,126,146–148 ‘clinical patient data’,1,149 ‘patient clinical data’,150 ‘patient health information’,151–158 ‘patient information’,16,26,29,40,41,47,66,97,116,159–165 ‘medical information’,21,28,34,97,107,129,166–171 ‘health-related information’,16,81,82,121,163,172–182 ‘patient-medical information’,183,184 ‘personal health information’,185 ‘clinical and demographic data’,186,187 ‘healthcare-related data’, 188–190 ‘health surveillance data’,191 ‘clinical and other patient data’,145 ‘surgical procedures’,42 ‘International Classification of Diseases’42 and ‘diagnostic codes and record episodes.’42
Health records
Healthcare information was categorised into various types of health records as given in Box 2.
Terms used to represent types of health records
‘Paper records’,161 ‘provider health records’ and ‘state registries’,79 ‘digital medical records’,192 ‘electronic medical record’ (EMR),113,165,191,193–198 ‘EHR’,5,57,67,81,107,136,162,169,179,199–209 ‘health information records’,130 ‘care records’,210 ‘personal health record’ (PHR),114,194 ‘patient health records’,211 ‘electronic patient records’212and ‘patient clinical records.’51
Further, the contents of healthcare information and health records included are given in Box 3.
Terms used to represent ‘contents’ of healthcare information and health records
‘Problem lists’,41,105 ‘illness’,96,185 ‘injuries’,96 ‘procedures’,42,105,126,158,184 ‘test results’,88,96,105,185,213,214 ‘radiology reports’,88,207,215,216 ‘allergies’,88,96,105,131,185 ‘images’ and prescriptions, 41,184 ‘medicines’,96,185 ‘medications’ lists,41,88,105,126,131‘hospitalization summaries’88 and ‘discharge summaries.’94,105,195
Claims and administrative data
Other health information involved claims and administrative data (see Box 4).
Terms used to represent claims and administrative data
Claims related to ‘health insurance and payments’,20 ‘claims information’217 and ‘health encounter claims’,79 whereas administrative data were labelled as ‘administrative health data’,69 administrative data,168 ‘administrative information’117,198 and ‘orders.’165
Information transfer as a function
Nearly, all the included definitions referred to health information are being exchanged through electronic processes. Words and expressions used to describe this process or its direction are given in Box 5.
Terms used to represent information transfer
‘Exchange’,55–57,141 ‘access’,69,82,138,207,218–220 ‘movement’,154,163,172,173,175–177,221 ‘sharing’,2,59,99,200,222 ‘multi-directional transfer’,223 ‘moving’,127,224,225 ‘bi-directional’,47,191,194 ‘mobilizes’,226 ‘connectivity’,54 ‘data flow’,122 ‘transferring’,55,61 ‘transfer’,58,70,109,112,115,133,160,216 ‘feed data repositories’,109 ‘transmission’,76,80,186,188,189,217,227,228 ‘transport’,49,100,184 ‘moves’,162 ‘access to and retrieval’87,110,111,115,121,130,160 and ‘link’/‘linking.’191,229–231
Further, health information was being exchanged and transferred through different mediums and methods such as ‘e-transfer’,55 ‘application-level communication’,49 ‘email’195,210 and ‘secure messaging.’196
Stakeholders involved in HIE
The third theme related to the range of stakeholders engaged in HIE, as shown in Box 6:
Terms used to represent different types of stakeholders involved in HIE
‘Doctors’67,69,85,96,142,156,166,179,184,185,232–234 or ‘physicians’,21,77–79,123,144,162,235–237 ‘clinicians’,1,56,87,97,99,109,131,135,161,213,218,238–240
‘nurses’,85,166,184,234,241,242 ‘patients’,5,38,90,109,133,138,206 ‘pharmacists’, 66,166,184 ‘health educators’,66 public health officials’,133 ‘healthcare professionals’, 29,33,36 ‘medical professionals’,90 ‘insurers’,142 ‘payers’,69,77,175,217,243 ‘policy makers’,233 ‘social workers’,66 ‘healthcare providers’,25,58,90,105,126,141,152,154,170,196,197,205,208,222,230,244 ‘customers’,44 ‘hospitals’,19,23,99,101,120,123,222,245 ‘health plans’,21,67,78,79,171 ‘laboratories’,67,77,85,246 ‘ radiology centres’,88 ‘pharmacies’,33,67,85,131,142,162,163,183,235,246,247 ‘hospitals’,21,32,124,184,195,215,222,237 ‘organizations’,134,223,226,248,249 ‘institutions’,34,36,44,99,141,250–252 ‘emergency departments’,25,128,142,213 ‘nursing homes’,101,123 ‘clinics’ (ambulatory/community),32,79,114,120,124,216 ‘quality assurance groups’,114 ‘government agencies’,18,188–190 ‘state agencies’,79 ‘public health agencies’,84,101,174,175,237,243 ‘public health facilities’,79 ‘public health entities’,114 ‘health information organizations’,188–190 ‘insurance companies’,18,33 ‘research groups’,114 ‘public health departments’123 and ‘federal reporting entities.’253
Some descriptions of stakeholders were more general, as shown in Box 7:
Potential benefits of HIE
Many definitions emphasised the benefits and potential benefits of using HIE, although these were framed in different ways. The dominant benefit was being able to transfer information in a secure way (see Box 8). Other themes related to healthcare quality, timeliness, improved decision making and patient centredness.
Terms used to represent potential benefits of HIE
Information security,25,30,43,60,70,89,95,98,100,127,153,157,164,173,182,191,198,227,234,238,255 ‘coded’,41,195 improved capacity for informed ‘decisions’,17,27,38,47,65,69,83,109,116,152,229,245,247,253 ‘effective’,21,71,103,115,121,129,160,234,252 ‘efficient’,33,84,95,121,148,160,233–235 ‘safer’,37,71,87,110,111,121,233 ‘coordinated’,81,234 ‘equitable’,37,71,110,111,115,121,129,130 ‘timelier’,103,121 patient-centred healthcare,37,71,84,110,111,115,121,129,130 ‘real-time’ information transfer,27,99,139,164,198,256 enhance ‘quality’ of healthcare,53,59,106,132,141,213,257 reduce costs,2,146,177,216,250,258 deliver ‘accurate’,97,107,213,247 ‘seamless’,47,99,140,255 ‘empowerment’93 and ‘complete’27,97,118,144,150,161,212,222,240,259 health information.
Technology required for HIE
Almost all of the definitions referred to ‘electronic’ or ‘digital’ data exchange. Most referred to the information infrastructure, systems or technology platforms used to host, transfer or exchange these data. Other related terms included those in Box 9.
Terms used to represent information technology
‘Technology platform’,43,47,165,225,260 ‘network infrastructure’,42,102,109,126,131,219,227,249,260–269 ‘health information technology’,154,172,189 ‘computer-based systems’,226 ‘technology model’,126 ‘information technology’,52,65,81,147,248,259,270 ‘HIE systems’,271,272 ‘document exchange system’,26,27,253 use of ‘online metadata registry’,242 ‘powerful technology’,273 ‘Web-based delivery systems’,215 ‘technical infrastructure’,133,267 ‘information infrastructure’,274 ‘electronic networks’,106 ‘electronic system’,152 ‘portal’,41 ‘computer network’,187 ‘interoperable technologies’,275 ‘central information systems’,159 ‘collection of activities and technologies’,104,276 ‘component of innovative’, 277 ‘friendly user interfaces’,278 ‘secured website’,116,170 ‘communication based on Web services’,51 ‘health care technology’,96 ‘health information systems’,265 ‘mobile computing technology’,119 ‘hubs’,136 ‘open source’231 and ‘data formats.’249
Focus/context of use
Different definitions also considered HIE with reference to its different contexts of use (see Box 10).
Examples of HIE in different contexts of use/focus
For instance, ‘nursing interventions’,279 ‘registered nurses’ working in home healthcare improving the quality of care through HIE,241 contributing to ‘emergency departments’24,119,124,142,161,213,239 and focusing on preventive and outcome-based medicines.158
HIE was also used for occupational health,15 mental health,280 HIV66,230 cancer care31 and cardiac surgery.119
It is also referred as a ‘set of activities’ to transfer information from one place to another,201,281 as a component of eHealth,43,246 as a method of utilising EHR81,144,169,204,209 or electronic patient record212 and as an important requirement of Stage 1 ‘meaningful use’ for hospitals.75,105,203,209,282
HIE was seen as an entity, organisation as well as a process as described below.
HIE as an entity or organisation
In many definitions, HIE was labelled as an ‘entity’60,70,73,74,77,83,143,227,283 that was established to exchange health information in a secure manner. It has also been prefixed as ‘legal entity’60 and ‘person or governmental entity.’227 In some definitions, HIEs were conceived as ‘organisations’186,284 or sets of organisational ‘services’ and infrastructures to support or streamline the exchange of health information.72,149,165,197,206,285,75,263,267,130 Other organisational concepts/terms used under this theme are given in Box 11).
Examples of HIE used as an entity or organisation
Here HIE was used as a ‘noun’, to describe an entity responsible for the exchange of health information.186,217,284 The term HIE was synonymously interchanged with local health information organisations,181 regional health information organisations (RHIOs)23,45,50,63,72,102,181,207,286 and sub-network organisations,181 though different names but serving the same purpose. Others perceived that HIEs were run and controlled by RHIOs,63 and were funded by healthcare delivery organisations.117
HIEs were occasionally recognised as multi-stakeholder organisations responsible for managing business and legal matters involved in the exchange of information.69 Moreover, HIEs were even regarded as the foundational part of accountable care organisations (ACOs)113 because they allowed EMRs to exchange information between various types of medical records. The other way around, HIEs were important for organisations that are transitioning into ACOs.94
HIE as a process
Here HIE was considered as the procedure involved in transferring electronic or digital health data in a protected environment among multi-stakeholders.68,81,145,178,180,200,223,224,235,261,283,284 Moreover, it was the process of utilising technology and systems to capture, store, share and retrieve the data electronically.35,48 In a few definitions, HIE was also reflected as a ‘verb’, an action, a process responsible for transmitting health information17,186,217,284 and collaboration among providers.21,32,94,117,171
Data standards
Incompatibility between systems and software has presented a barrier to HIE, and for this reason, the importance of interoperability standards is emphasised in the majority of definitions. Keywords and phrases related to this are given in Box 12.
Terms used to represent the use of data standards
‘Standards’,180,201 ‘nationally recognized standards’,100,121,137,154,173,175-177,228,283 ‘nationally recognized vocabularies’,195 ‘policies and standards’,133 ‘standardise’,149,152,208,254 ‘standardized content’,49 ‘standard procedures’,129 ‘nationwide standards’,283 ‘national standards’,153,188–190 standards-based infrastructure’,30 ‘standard-based exchange/solution’,36,238 ‘cross enterprise document sharing (XDS)’186 to ‘Health Insurance Portability and Accountability Act (HIPAA) standards.’ 89
Connectivity between different‘locations’
Definitions falling within this theme emphasised the exchange of information among facilities or organisations located in different areas (see Box 13).
Terms used to represent different locations
Such as within a ‘region’,2,21,52,69,72,76,87,110,115,145,147,162,163,171,231,233,257 or at a ‘regional level’,5,40,44,55,75,82,83,271,283 ‘community’,2,31,69,82,102,109,124,165,247,287 ‘non-clinical settings’,66 ‘metropolitan regions’,124 ‘sites of care’,150 ‘delivery settings’,54,59 ‘city’,233 ‘state/statewide’,21,40,82,131,156,164,168,191,203,205,233 ‘member sites’,267 ‘geographic area’,51,68,72,74,138,145 ‘provincial’,40 ‘local level/local health departments’,32,75,139,271 ‘national level’,40,44,75,271 ‘across countries’,76 ‘neighbourhood/neighbouring states’,168,283 ‘multi-state’83 and ‘nationwide.’57,256,283
Public health outcomes
The uses of HIE in population health were stressed in a number of definitions.97,127,165,255,288 Relevant concepts covered the uses of HIE for supporting public and community health practices, population health monitoring and research (see Box 14).
Terms used to represent public health functions of HIE
Concepts included connecting ‘public health departments’,122,139 supporting ‘public health practices’,254 undertaking ‘public heath activities’,150 linking ‘public health surveillance data’,191 ‘public health reporting’,148,253 evaluation and planning of ‘public health services’,148 ‘public health event-monitoring capability’,256 ‘public health situational awareness’,256 analysing the ‘health of the population’,110 ‘countrywide population health’,115 ‘statistics for public health’,72 assist ‘public well-being’,283 protecting ‘public interest’,91 ‘public health organizations’,32 promote ‘population health’, 65,109,141,148,243 health data on a ‘population level’,139 ‘track population health’,253 refine ‘US health care system’,56,74 HIE for a ‘16-county region’171 and ‘community betterment’.87,168
Business solutions/objectives of HIE
A number of definitions conceived of HIE as either a commercial solution facilitating information exchange or in terms of its business objectives.289 It was suggested that HIE will come up with their viable business plans when stimulus funding from the government will end.290 See more examples of HIE business solutions/objectives are given in Box 15.
Examples of HIE as business solutions/objectives
One vendor represented itself as a national HIE ‘company’,291 while other definitions emphasised issues like scalability and efficiency.258
Siemens offered a four-dimensional HIE ‘solution’, organised according to ‘economics’, ‘care’, ‘service’ and ‘technology.’198
Transactions between providers or between services or suppliers often involve secure data exchange.17,100 This may be conceived in terms of ‘data supplier and data receiver’ 17 but also ‘competitors’43 and ‘customers.’44
HIE has been spoken about in terms of exchanging health information across traditional business boundaries62 and also characterized as ‘large multi-billion dollar efforts.’252
HIE has also been characterised as an infrastructure that includes business models, technology model and the legal model to facilitate the exchange of information among various organisations.91,126
The ‘primary business focus’ of networks involved in building HIEs was to create value for the provider community by forming ‘productive efficiencies.’102
One of the authors termed HIE as entities built on ‘bilateral legal agreements’ between proprietary information systems to be able to share different kinds of data.177 HIE is seen as an administrative as well as a clinical tool,27,117,168 and as a tool for exchanging insurance information.292
Sectoral or regional scope
Many definitions conceived HIE in terms of sectoral, geographic or occupational scope (see Box 16)
DISCUSSION
The analysis has revealed considerable variability among existing definitions of HIE and insights into the range of concepts that are embedded within these definitions.
Many definitions included not only the exchange of patient information but also other types of information such as demographics, claims and administrative data. Definitions also described health information sharing and connectivity at the level of organisations, states or regions and nations, possibly reflecting the different ways in which care is organised in different national contexts.
While the US government has provided incentives for the adoption of HIE, securing long-term funding is a major challenge for sustainability. Implementing HIE represents an investment and not simply a cost and this is accompanied by a realisation that policy makers must find approaches to assure that all stakeholders who benefit from HIE pay to support it and specifically that efforts should be made to engage private payers.293
A wide variety of stakeholders are engaged in HIE, not only including healthcare professionals and patients but also policy makers, researchers, and insurance companies, for example. Although infrastructural, economic, technical and cultural barriers have impeded the participation of some stakeholder groups in HIE efforts, it remains the core of the vision for a connected, coordinated and learning health system.294
Not surprisingly, the majority of definitions highlighted the importance of secure information exchange and many pointed to the requirement for common data standards necessary for the quality of data content, clinical documentation, data mapping and, most importantly, interoperability between disparate systems.201 Common standards will also ensure data protection, confidentiality, interoperability and privacy.29,129,189,228
The value of HIE for supporting public health is referred to in many of the definitions, with the ability to meaningfully move clinical data across disparate systems being seen as vital for effective health surveillance and management of care delivered outside health facilities.295
Strengths and limitations
This review aimed to identify, classify and map definitions of HIE and was not intended as an in-depth analysis of the challenges and opportunities presented by HIE, although such issues were inevitably reflected in many of the definitions. The search terms used to identify definitions of HIE were limited to those that we considered most relevant and it is possible that extending them to include other pertinent concepts in health informatics might have revealed further descriptions of HIE and HIE-like concepts. However, we have followed previous authors in prioritising the search for explicit definitions, as a means of generating insights into how the concepts has evolved and how it is being discussed.8,12 Using both research databases and a general web search engine gave us greater scope to reach both academic and non-academic literature. Internet searches were restricted to Google and while it is possible that additional definitions may have been found using other search engines, the very large number of hits produced by our queries suggests that it was an effective means of identifying the majority of relevant content in the online grey literature.
The included definitions reflect the dominance of the US literature pertaining to HIE and, to some extent, the language used to describe information sharing concepts in that national context. We acknowledge this limitation, interpreting it as a consequence of the major investment in HIE in the US over recent years, with its inevitable knock-on effects on the volume of literature emerging from that part of the world. As the term gains wider international currency and other countries prioritise investments in HIE, this national balance may change. Nevertheless, a post-hoc analysis excluding the US definitions revealed similar themes as found across our entire corpus of 268 definitions, which encompasses research pre-HIPPA, suggesting that that the concept and function of HIE is similar in different parts of the world and has consistencies over time (Table 6).
Implications for research, practice and policy
The definitions of HIE appearing in the literature vary on a number of philosophical and conceptual attributes, and many are context specific. The ways in which different authors choose to describe concepts is inevitably influenced by their backgrounds and vested interests and it is therefore not surprising to observe the differences in emphasis. However, we were struck by the clear alignment of the HIE concept with specific technologies or business opportunities in some definitions, where HIE is used describe a service, an organisation or a technology, rather than a process or concept. Such a language was often used by businesses promoting their products or in the context of state information systems, where ‘the exchange’ is pictured as an operational entity. This creates important obstacles to communication about HIE, particularly for policymakers involved in making decisions about strategy and procurements.
We have not found a single definition that encompasses all of the key attributes of HIE identified by our thematic analysis. The one suggested by Finn69 is one of the most comprehensive and differentiates ‘HIE’ as a concept related to the processes of data transfer and sharing, and ‘HIEs’ as entities responsible for overseeing effective HIE, while also recognising the benefits, scope and stakeholders involved.69 The broad concept of HIE also describes a set of enabling technologies that support these processes, including data standards and public health objectives. The use of HIE as a noun describing organisational entities concerned with mediation and governance of information transfers is largely, although not exclusively, a US phenomenon and also qualitatively different from process-oriented definitions. It has therefore has been placed in separate sentence. Based on our review, we proposed the following integrated definition of HIE shown in Box 17, which is a heavily adapted version of the one proposed by Finn.69
While this definition may not be ideally suited to all contexts (such as HIE for specific diseases and/or community HIE), we believe it provides a good overall fit with the themes identified in the heterogeneous corpus of definitions revealed by our review and therefore propose it for possible wider adoption (see Figure 4).
Adapted and proposed HIE definition
‘HIE is the electronic mobilisation of clinical and administrative information within or across organisations in a region or community and, potentially, internationally between various systems according to locally and/or nationally recognised standards while maintaining the authenticity and accuracy of the information being exchanged, enabling stakeholders to make informed decisions to enhance healthcare quality of a patient and population. HIEs are multi-stakeholder organisations that oversee the business, operational and legal issues involved in the exchange of information.’

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CONCLUSIONS
This review has shed light on the different facets of HIE. In the spirit of promoting further scholarly discussion and debate, we have proposed a definition that encompasses the key underpinning constructs. We recommend that future authors consider the findings of this review before developing new definitions of HIE, in order to avoid adding further heterogeneity. We also hope the review has value for policymakers involved in planning, procurement and evaluation of HIE.
Acknowledgments
We wish to record our appreciation to Professor Brian McKinstry and the anonymous reviewers for their comments on an earlier draft of this manuscript.
Appendix A: Extracted Definitions
Appendix B: Recurrent topics of HIE
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.↵
- 212.↵
- 213.↵
- 214.↵
- 215.↵
- 216.↵
- 217.↵
- 218.↵
- 219.↵
- 220.↵
- 221.↵
- 222.↵
- 223.↵
- 224.↵
- 225.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.↵
- 232.↵
- 233.↵
- 234.↵
- 235.↵
- 236.
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.↵
- 247.↵
- 248.↵
- 249.↵
- 250.↵
- 251.
- 252.↵
- 253.↵
- 254.↵
- 255.↵
- 256.↵
- 257.↵
- 258.↵
- 259.↵
- 260.↵
- 261.↵
- 262.
- 263.↵
- 264.
- 265.↵
- 266.
- 267.↵
- 268.
- 269.↵
- 270.↵
- 271.↵
- 272.↵
- 273.↵
- 274.↵
- 275.↵
- 276.↵
- 277.↵
- 278.↵
- 279.↵
- 280.↵
- 281.↵
- 282.↵
- 283.↵
- 284.↵
- 285.↵
- 286.↵
- 287.↵
- 288.↵
- 289.↵
- 290.↵
- 291.↵
- 292.↵
- 293.↵
- 294.↵
- 295.↵
- 296.
- 297.
- 298.
- 299.
- 300.
- 301.
- 302.
- 303.
- 304.
- 305.
- 306.
- 307.
- 308.
- 309.
Footnotes
Funding We would like to thank Higher Education Commission Pakistan and The University of Edinburgh for providing funds for this review.