Article Text

Abstract
Objective Risk stratification is crucial to optimise treatment strategies in patients with COVID-19. We aimed to evaluate the impact on mortality of an early assessment of cardiac biomarkers in patients with COVID-19.
Methods Humanitas Clinical and Research Hospital (Rozzano-Milan, Lombardy, Italy) is a tertiary centre that has been converted to the management of COVID-19. Patients with confirmed COVID-19 were entered in a dedicated database for cohort observational analyses. Outcomes were stratified according to elevated levels (ie, above the upper level of normal) of high-sensitivity cardiac troponin I (hs-TnI), B-type natriuretic peptide (BNP) or both measured within 24 hours after hospital admission. The primary outcome was all-cause mortality.
Results A total of 397 consecutive patients with COVID-19 were included up to 1 April 2020. At the time of hospital admission, 208 patients (52.4%) had normal values for cardiac biomarkers, 90 (22.7%) had elevated both hs-TnI and BNP, 59 (14.9%) had elevated only BNP and 40 (10.1%) had elevated only hs-TnI. The rate of mortality was higher in patients with elevated hs-TnI (22.5%, OR 4.35, 95% CI 1.72 to 11.04), BNP (33.9%, OR 7.37, 95% CI 3.53 to 16.75) or both (55.6%, OR 18.75, 95% CI 9.32 to 37.71) as compared with those without elevated cardiac biomarkers (6.25%). A multivariate analysis identified concomitant elevation of both hs-TnI and BNP as a strong independent predictor of all-cause mortality (OR 3.24, 95% CI 1.06 to 9.93).
Conclusions An early detection of elevated hs-TnI and BNP predicts mortality in patients with COVID-19. Cardiac biomarkers should be systematically assessed in patients with COVID-19 at the time of hospital admission in order to optimise risk stratification.
- coronary artery disease
- global health
- systemic inflammatory diseases
- myocardial disease
- cardiac risk factors and prevention
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- coronary artery disease
- global health
- systemic inflammatory diseases
- myocardial disease
- cardiac risk factors and prevention
Introduction
COVID-19 subsequent to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is causing a dramatic pandemic,1 with over 2 million confirmed cases and over 150 000 deaths as of 22 April 2020.2
An early risk stratification is crucial in patients with COVID-19 in order to identify those that benefit from intense monitoring and aggressive treatment strategies.1 This is of paramount importance in conditions of limited human and material resources, which is a frequent occurrence during COVID-19 surges.3 4
Besides the respiratory involvement, a cardiac involvement has been described in patients with COVID-19.5–9 Two studies from China have suggested that patients with COVID-19 who develop a myocardial injury during hospitalisation, detected with cardiac troponin, have a higher risk of mortality as compared with those who do not develop a myocardial injury.7 8 These findings have been subsequently confirmed in large retrospective series from Europe and USA.10 11
Whether an early detection of cardiac involvement, through the measurement of cardiac biomarkers at the time of hospital admission, may play a role for risk stratification in patients with COVID-19 is currently unknown.
The aim of the present study was to evaluate the impact on mortality of an early detection of elevated cardiac biomarkers in patients with confirmed COVID-19.
Methods
Humanitas Clinical and Research Hospital (Rozzano-Milan, Lombardy, Italy) is a large tertiary centre that has been largely converted to the management of COVID-19. All consecutive patients diagnosed with COVID-19 according to the WHO interim guidance hospitalised up to 1 April 2020 and available data on cardiac biomarkers were retrospectively included in this institutional registry. No exclusion criteria were applied.
Data collection
Data were retrospectively collected from the electronic medical records and validated through review of all source documentation by five investigators. The following data were collected: patients’ demographics, cardiovascular risk factors, medical history, comorbidities, clinical and haemodynamic parameters at presentation, baseline and in-hospital medical therapy, laboratory parameters at baseline and during hospitalisation, and clinical outcomes.
Cardiac biomarkers
A biomarker of myocardial injury—that is, high-sensitivity troponin I (hs-TnI)—and a biomarker of cardiac stress—that is, B-type natriuretic peptide (BNP)—were used as biomarkers of cardiac involvement. The first available value obtained within 24 hours of hospital admission was considered. The value was considered as elevated if above the upper limit of normal serum levels according to our institutional laboratory normal ranges (ie, hs-TnI ≥19.6 ng/L, BNP ≥100 pg/mL). At our institution, hs-TnI and BNP assays have been integrated into the laboratory test panels for patients with COVID-19 at the time of hospital admission since the beginning of COVID-19 outbreak in Italy, due to the early concerns for cardiovascular involvement emerging from Chinese experience. Hs-TnI values were obtained with the chemiluminescent immunoassay ACCESS hs-TnI, Beckman Coulter, using the DXI800 platform.
Outcomes
The primary outcome was all-cause mortality. Secondary outcomes were admission in the intensive care unit (ICU), acute respiratory distress syndrome (ARDS) and shock.
Definitions
COVID-19 was defined according to the WHO interim guidance. SARS-CoV-2 tests were performed with the reverse transcription PCR assay.
In case of multiple accesses to the ICU, only the date of the first access was considered as the date of occurrence of this outcome, while the overall duration of stay in ICU was calculated. In case of multiple intubations, only the date of the first intubation was considered as the date of occurrence of this outcome, while the overall duration of intubation was calculated. ARDS was defined according to the Berlin definition.12 Shock was defined as mean arterial pressure <70 mm Hg or systolic blood pressure (SBP) <100 mm Hg despite adequate amount of fluids and clinical and laboratory signs of hypoperfusion.13
Arterial hypertension, dyslipidaemia and diabetes mellitus were defined based on reported medical history and medical therapy. Dyslipidaemia was defined based on cholesterol and triglycerides values during hospitalisation and on use of lipid-lowering medications. Chronic kidney disease was assessed based on the estimated glomerular filtration rate (eGFR) with the Modification of Diet in Renal Diseases. Other comorbidities were defined based on reported medical history. Haemodynamic and respiratory parameters were recorded at the time of hospital admission.
Data analysis
Continuous variables are reported as median (IQR) and were compared using Student’s t-test or the Mann-Whitney U or Wilcoxon test in case of two-group comparisons on the basis of normality of data distribution, verified using the Kolmogorov-Smirnov goodness-of-fit test. In case of continuous variable comparisons between more than two groups, analysis of variance was performed. Bartlett’s test for equal variances was performed to assess if the variances were comparable between groups. Categorical variables are reported as number (percentage) and were compared using the χ2 test without Yates’ correction for continuity or the Fisher’s exact test as appropriate. OR and 95% CI for the primary and secondary outcomes were calculated with binary logistic regression. Clinical follow-up was censored at the date of death or discharge. We performed two multivariable logistic regression analyses to test the multiplicative association between baseline clinical and laboratory variables and all-cause mortality. In the first one, the backward stepwise selection incorporated age, sex, body mass index >30 kg/m2, body temperature >37.5°C, eGFR <60 mL/min/m2, diabetes mellitus, chronic obstructive pulmonary disease, left ventricular ejection fraction <50%, malignancy, heart rate >100 bpm, respiratory rate >20 bpm, hs-TnI, BNP, C reactive protein, absolute white cell count >10 000/mm3, D-dimer, gender, ferritin, lymphocyte count, white cell count, desaturation (defined as admission oxygen saturation without oxygen therapy below 94% or immediate necessity of oxygen therapy at the time of hospital admission) and baseline use of ACE inhibitors (ACEi) or angiotensin receptor blockers (ARBs). In the second model, we included the categorical variable cardiac involvement (hs-TnI ≥19.6 ng/L and BNP ≥100 pg/mL) in place of the continuous variables hs-TnI and BNP. The models included only vital parameters at admission and laboratory values obtained within 24 hours of hospital admission. Area under the curve (AUC) and 95% CI were calculated to assess the predictive discriminatory power of both models. Variables were excluded from the model in case of p values<0.20. An n-fold cross-validation for the AUC for death was performed for the two logistic regression models in order to provide cross-validated fitted probabilities for death. In brief, this method averages the AUCs corresponding to each fold and applies the bootstrap procedure to the cross-validated AUC to obtain statistical inference and 95% bias corrected CIs. Two-sided p values <0.05 were considered statistically significant. Statistical analyses were performed using Stata (V.13.0).
Results
A total of 397 consecutive patients with confirmed COVID-19 were included in this registry, with a median follow-up of 12 days (IQR 6–17 days). The median age was 66.7 years (IQR 55–75.7 years) and 267 patients (67.3%) were men.
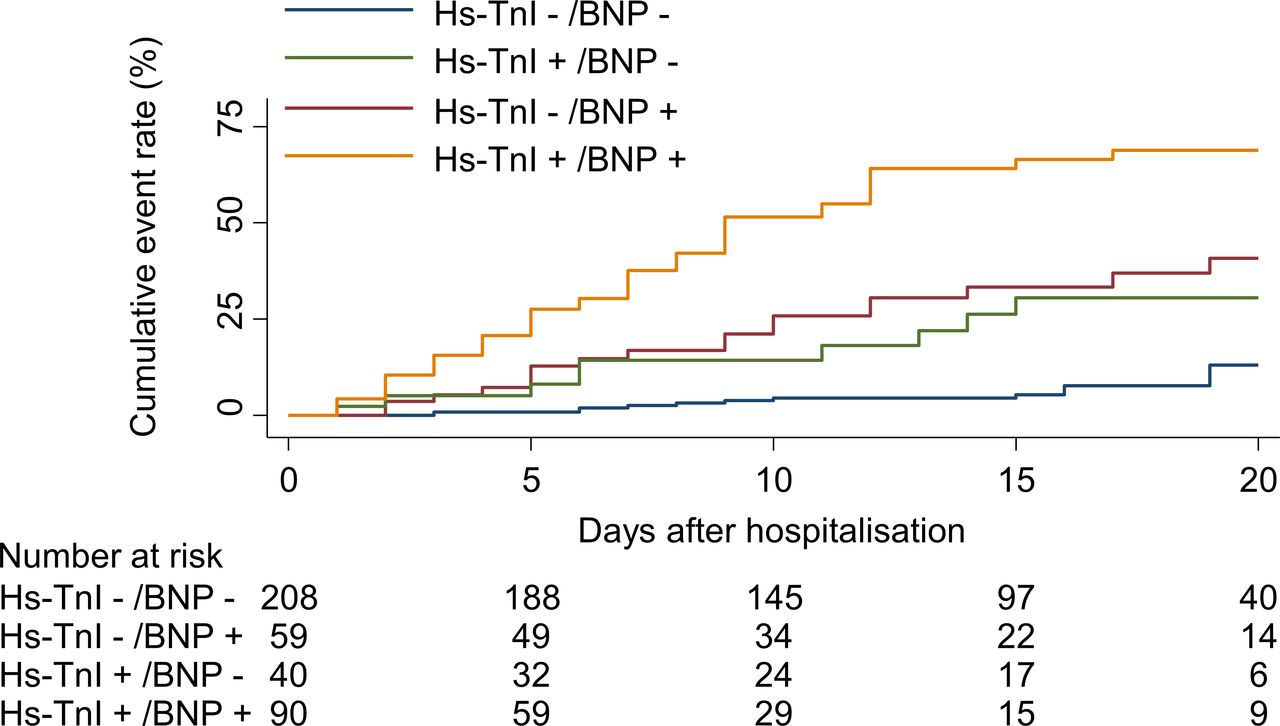
At the time of hospital admission, 208 patients (52.4%) had normal values for cardiac biomarkers, 90 (22.7%) had an elevation of both hs-TnI and BNP, 59 (14.9%) had elevated only BNP and 40 (10.1%) had elevated only hs-TnI.
Baseline clinical characteristics and clinical presentation are summarised in table 1. Patients with elevated cardiac biomarkers were older (p<0.001) and had more frequently dyslipidaemia (p<0.001), diabetes mellitus (p=0.005), a prior myocardial infarction (p<0.001), a left ventricular ejection fraction <50% (p=0.001), a history of atrial fibrillation and a prior cerebrovascular event (p<0.001) as compared with those without elevated cardiac biomarkers.
Baseline clinical characteristics and presentation
With respect to non-cardiovascular comorbid conditions, patients with elevated cardiac biomarkers had more frequently chronic kidney disease (p<0.001) and chronic obstructive pulmonary disease (p=0.013) as compared with those without elevated cardiac biomarkers.
As it relates to clinical presentation, patients with elevated cardiac biomarkers had more frequently a heart rate >100 beats per minute and a respiratory rate >20 breaths per minute as compared with those without elevated cardiac biomarkers. Conversely, body temperature, SBP and first oxygen saturation did not differ significantly between groups.
Laboratory values are summarised in table 2. At baseline, patients with elevated cardiac biomarkers also had higher d-dimer (p<0.001), fibrinogen (p=0.013), creatinine (p<0.001), white cell count (p=0.007) and procalcitonin (p=0.026). Of note, only 10 patients (2.5% of total population) did not report a value of both hs-TnI and BNP at the time of hospital admission, 21 patients (5%) did not have a value of BNP while having a hs-TnI value and 7 patients (1.7%) did not report a value of hs-TnI while having a BNP value.
Laboratory values
Baseline and in-hospital medical therapy are summarised in table 3. Patients with elevated cardiac biomarkers were more frequently taking cardiovascular medications at the time of admission as compared with patients without elevated biomarkers. In-hospital pharmacological therapy did not differ substantially between groups.
Baseline and in-hospital medical therapy
Clinical outcomes are summarised in table 4. In-hospital follow-up was complete for all patients: 305 patients (76.8%) have been discharged and 92 patients (23.2%) died. The rate of mortality was higher in patients with elevated hs-TnI (22.5%, OR 4.35, 95% CI 1.72 to 11.04), BNP (33.9%, OR 7.37, 95% CI 3.53 to 16.75) or both (55.6%, OR 18.75, 95% CI 9.32 to 37.71) as compared with those without elevated cardiac biomarkers (6.25%). A significant differential effect by BNP elevation was observed with an increased risk of death among patients with elevated hs-TnI (pinteraction=0.044). The rate of admission in the ICU was higher in patients with elevated hs-TnI (27.5%), BNP (22.0%) or both (18.9%) as compared with those without elevated cardiac biomarkers (11.5%). Similar findings were observed for ARDS and shock.
Clinical outcomes
Cumulative event rates for all-cause mortality according to baseline cardiac biomarkers elevation are displayed in figure 1.

Cumulative incidence of mortality according to baseline cardiac biomarkers. BNP, B-type natriuretic peptide; hs-TnI, high-sensitivity troponin I.
A multivariate analysis including in the model only vital parameters at admission and laboratory values obtained within 24 hours of hospital admission, shown in online supplementary table 2, identified hs-TnI (OR 1.01, 95% CI 1.00 to 1.01, p=0.037) but not BNP as independent predictors of all-cause mortality, together with age (OR 1.10, 95% CI 1.05 to 1.15, p<0.001), desaturation (OR 2.54, 95% CI 1.16 to 5.59, p=0.020) and D-dimer (OR 1.51, 95% CI 1.01 to 2.28, p=0.046). An additional multivariate analysis, displayed in figure 2, identified elevated values of both hs-TnI and BNP as independent predictors of all-cause mortality (OR 3.24, 95% CI 1.06 to 9.93, p=0.039), together with age (OR 1.13, 95% CI 1.06 to 1.20, p<0.001), lymphocyte count (OR 0.19, 95% CI 0.05 to 0.71, p=0.014), and D-dimer (OR 1.00, 95% CI 1.00 to 1.01, p=0.049). AUCs were 0.884 (0.83–0.92) for the first and 0.938 (0.85–0.94) for the second model, indicating good predictive value in both cases (online supplementary figures 1 and 2). N-folds cross-validation resulted in a cross validated AUC of 0.883 (0.83–0.91) for the first and 0.926 (0.85–0.94) for the second model, confirming good predictive value of both models.
Supplemental material

{kind=link}
{kind=link}
Baseline predictors of mortality at multivariable logistic regression analysis. The backward stepwise selection incorporated age, sex, body mass index >30 kg/m2, body temperature >37.5°C, eGFR <60 mL/min/m2, diabetes mellitus, chronic obstructive pulmonary disease, left ventricular ejection fraction <50%, malignancy, heart rate >100 bpm, respiratory rate >20 bpm, cardiac involvement (defined as both hs-TnI ≥19.6 ng/L and BNP ≥100 pg/mL), C reactive protein, absolute white cell count >10 000/mm3, D-dimer, gender, ferritin, lymphocyte count, white cell count, desaturation (defined as admission oxygen saturation without oxygen therapy below 94% or immediate necessity of oxygen therapy at the time of hospital admission) and baseline use of ACE inhibitors or angiotensin receptor blockers. The model included only vital parameters at admission and laboratory values obtained within 24 hours of hospital admission. BNP, B-type natriuretic peptide; eGFR, estimated glomerular filtration rate; hs-TnI, high-sensitivity troponin I.
Discussion
We aimed to investigate the prognostic implications of an early cardiac involvement in hospitalised patients with COVID-19. Our findings can be summarised as follows:
Approximately 50% of patients with confirmed COVID-19 have evidence of elevated cardiac biomarkers at the time of hospital admission.
Cardiac biomarkers elevation at the time of admission is associated with higher rates of all-cause mortality.
The elevation of both hs-TnI and BNP at the time of hospital admission is a strong independent predictor of all-cause mortality.
Patients with COVID-19 have an extremely heterogeneous clinical presentation, ranging from absence of symptoms to major respiratory disorders requiring intensive care assistance.1 5 6 9 14 According to evidence from China, Europe and USA, patients with the most severe clinical presentation tend to be elderly and are characterised by a large number of clinical comorbidities. Among these, a significantly higher prevalence of cardiovascular risk factors and history of ischaemic heart disease have been described in patients with COVID-19 evolving in worse outcomes.1 5 6 Therefore, although respiratory symptoms represent the main clinical manifestations of COVID-19, several patients—regardless the presence of a prior cardiac history—also experience severe cardiovascular complications.9 In Wuhan, China, myocardial injury—diagnosed as an increase in high-sensitivity cardiac troponin—was observed in 5 of the first 41 patients with confirmed COVID-19.9 In a report of 138 patients with COVID-19 in Wuhan, 7.2% had evidence of myocardial injury, with higher levels of cardiac biomarkers in patients treated in ICU.5 Among patients who died from COVID-19 in China, 11.8% of those without known underlying cardiovascular disease showed elevated levels of hs-TnI or had cardiac arrest during hospitalisation.6
A few observational studies from China have specifically investigated the association of cardiac injury during hospitalisation and mortality in patients with COVID-19.7 8 In a case series of 187 patients with confirmed COVID-19, Guo and colleagues7 showed that patients with myocardial injury (ie, increased troponin T levels) during hospitalisation had an increased risk of mortality as compared with those without myocardial injury, regardless the presence of underlying cardiovascular disease. Similar findings were reported by Shi and colleagues8 in a cohort of 416 patients, in which cardiac injury during hospitalisation was common (occurred in 20% of patients) and associated with a higher risk of mortality. Another observational study evaluated specifically the impact of myocardial injury on clinical outcomes in 671 patients with severe COVID-19 and identified cardiac troponin I and N-terminal pro-BNP as independent predictors of in-hospital death by a multivariable Cox regression analysis.15 Further studies from Europe and USA confirmed these findings.10 11 However, an early detection of cardiac involvement and the impact of concomitant elevation of BNP and hs-TnI in patients with COVID-19 have not been specifically evaluated to date.
Overall, the currently available evidence has consistently shown an association of cardiac injury developed during hospitalisation with mortality in patients with COVID-19. In order to provide pragmatic evidence, with potential use for risk stratification, we evaluated the prognostic impact of an early evidence of elevated cardiac biomarkers. By showing a strong association with mortality of an early elevation of cardiac biomarkers, we support the systematic use of hs-TnI and BNP for risk stratification at the time of hospital admission. Moreover, we found a significant differential effect by BNP elevation with an increased risk of death among patients with elevated hs-TnI, confirming that the concomitant elevation of BNP and hs-TnI underlines a higher risk of in-hospital mortality than hs-TnI elevation alone.
The two cardiac biomarkers used in our study focus on different aspects of cardiac involvement. Hs-TnI is a biomarker of myocardial injury, while BNP is a biomarker of cardiac stress. We, therefore, focused our analysis on a global early evaluation of cardiac involvement. Potential mechanisms underlying an early cardiac involvement include direct myocardial involvement of SARS-CoV-2, myocardial injury due to hypoxaemia, myocardial injury due to increased thrombogenicity, cytokine storm triggered by the infection, increased sympathetic stimulation, endothelial dysfunction due to vascular cells SARS-CoV-2 infection and a right heart overload due to pulmonary implications of the disease. However, based on our findings alone, we cannot mechanistically impute to a cardiac damage the prognostic relevance of an early elevation of cardiac biomarkers. We rather hypothesise that an early evidence of cardiac involvement allows to identify patients with COVID-19 at the highest risk of adverse prognosis. However, the absence of cardiac involvement represents a favourable prognostic marker and a likely marker of lower risk of in-hospital death. Thus, an early assessment of BNP and hs-TnI in patients with COVID-19 may help physicians in the appropriate triage, timely intensive monitoring and treatment for subjects at high risk of death, and outpatient management for those at very low risk of death. Moreover, the presence of cardiac involvement might allow an early detection of previously undiagnosed cardiac diseases and more dedicated cardiological surveillance, eventually followed by more dedicated cardiovascular follow-up and tailored interventions after discharge. Resource allocation in case of new outbreaks and cardiovascular prevention might truly benefit from an early assessment of BNP and hs-TnI. Anyway, the association between elevated cardiac biomarkers and adverse prognosis need further evaluation in studies elucidating pathophysiological mechanisms of disease.
Of note, while rates of mortality were higher in patients with an early elevation of both hs-TnI and BNP, ICU admission occurred less frequently in these patients than in patients with only one of the two biomarkers elevated. This might be partly explained by the fact that an early elevation of both hs-TnI and BNP identified a patient population with a higher burden of comorbid conditions that might have not been considered for aggressive treatment strategies during the most intense phase of the COVID-19 outbreak in view of the limited available resources.3 4 It is important to underscore that the data included in this study focus on patients treated during the first 6 weeks of the outbreak, characterised by the highest degree of COVID-19 related pressure on the regional healthcare system.3 4
Our findings should be interpreted in light of some limitations. First, the single-centre nature of the study has intrinsic limitations. However, we systematically collected data of all consecutively hospitalised patients at our institution, increasing the generalisability of our findings. Second, beyond cardiac biomarkers, a more specific early evaluation of cardiac involvement with echocardiography might have provided additional information. However, echocardiography was not performed at the time of hospital admission in any of the included patients and its use was largely restricted during hospitalisation because of isolation conditions of wards and ICU during the COVID-19 pandemic. Third, ARDS diagnoses were probably under-reported among patients not admitted to ICU, limiting the reliability of our findings regarding this outcome. Fourth, 38 patients had no available values of hs-TnI, BNP or both due to issues with samples (ie, haemolysis) or mistakes in laboratory test requests. Lastly, the observational nature of our findings does not support a cause–effect relationship between cardiac involvement and mortality. However, our findings support the use of cardiac biomarkers for risk stratification of patients with COVID-19 at the time of hospital admission. In consideration of the wide diffusion and relative low cost of these biomarkers across all hospitals worldwide, their early assessment in patients with COVID-19 may represent a pragmatic tool for risk stratification.
Conclusions
Elevated hs-TnI and BNP at the time of hospital admission predict mortality in patients with COVID-19. Cardiac biomarkers should be systematically assessed in patients with COVID-19 at the time of hospital admission in order to optimise risk stratification.
Key messages
What is already known on this subject?
Myocardial injury is common in hospitalised patients with COVID-19 and is associated with mortality.
What might this study add?
An early elevation of both high-sensitivity troponin I and B-type natriuretic peptide at the time of hospital admission is a strong independent predictor of in-hospital mortality.
An early assessment of cardiac biomarkers is a pragmatic and feasible tool for risk stratification in patients with COVID-19, given the wide diffusion and relative low cost of these biomarkers across all hospitals worldwide.
How might this impact on clinical practice?
Clinicians should systematically assess cardiac biomarkers in patients with COVID-19 at the time of hospital admission in order to optimise risk stratification and improve resource allocation.
Acknowledgments
We would like to thank all the healthcare providers involved at Humanitas Clinical and Research Hospital during the COVID-19 outbreak.
Footnotes
Twitter @GGStefanini
Contributors GGS, MC, FC and GC conceived the idea and design for the study. GGS, MC and FC analysed the data. All authors contributed to interpret the data. GGS, MC and FC drafted the manuscript. All authors contributed to revise the draft critically for important intellectual content and approved the final manuscript.
Funding This work was supported by COVID-19 Welfare Funds of Regione Lombardia.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Humanitas Clinical and Research Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.