Article Text

Abstract
Background Quality improvement professionals often choose between patient-specific interventions, like clinical decision support (CDS), and population-based interventions, like registries or care management. In this paper, we explore the synergy of these two strategies, targeting the problem of procedure documentation for patients with a history of splenectomy.
Methods We developed a population health documentation (PHD) intervention and a CDS intervention to improve splenectomy documentation within our electronic health record. Rates of splenectomy documentation were collected before and after the implementation of both interventions to assess their impact on the rate of procedure documentation.
Results Both the PHD and CDS interventions led to statistically significant (p<0.001) increases in the baseline rate of splenectomy documentation of 27.4 documentations per month. During the PHD intervention, 444.7 splenectomies were documented per month, while 40.8 splenectomies per month were documented during the CDS intervention.
Discussion Both approaches were successful, with the PHD intervention leading to a larger number of incremental procedure documentations, in batches, and the CDS intervention augmenting procedure documentation on an ongoing basis. Our results suggest that population health and CDS strategies complement each other and, where possible, should be used in conjunction.
Conclusions PHD and CDS strategies may best be used in conjunction to create a symbiotic relationship in which current problem and procedure documentation gaps are closed using PHD strategies, while new gaps are prevented through ongoing CDS interventions
- Decision Support, Clinical
- Decision Support, Computerised
- Information Technology
- Quality Improvement
- Quality Measurement
Statistics from Altmetric.com
- Decision Support, Clinical
- Decision Support, Computerised
- Information Technology
- Quality Improvement
- Quality Measurement
Background
Quality improvement professionals have a range of tools in their armamentarium, including provider-centric strategies like training, patient-specific strategies like clinical decision support (CDS) alerts and reminders, and population-based strategies like registries and centralised care processes. In this paper, we consider two complementary strategies: CDS and a population health documentation (PHD) intervention to improve electronic documentation of splenectomy.
Splenectomy, a procedure to remove a damaged spleen, is performed in response to trauma to the spleen, hyperactivity of the spleen, a number of blood diseases, as well as other conditions.1 2 The surgical procedure places patients at an increased risk of sepsis due to the spleen’s role in fighting infections.3 Due to this increased risk, it is recommended that splenectomy patients receive a number of vaccinations, including the pneumococcal vaccine, Haemophilus influenzae type b vaccine and meningococcal vaccine, and it is recommended that some patients receive preventive antibiotic therapy.2 4
CDS can help ensure that patients are properly vaccinated following a splenectomy by alerting providers when a patient is due for a vaccine.5–7 However, this CDS requires splenectomy to be properly documented on patient problem or procedure lists within the electronic health record (EHR). Unfortunately, gaps in splenectomy documentation are common. In previous work, we found that 71% of patients with mention of the word ‘splenectomy’ on their chart did not have documentation of splenectomy on their problem list.6
Documentation gaps within the EHR are not limited to splenectomies, as problem and procedure lists have routinely been shown to be incomplete and inaccurate.8–10 In previous work, we found that problem list completeness varied considerably based on condition, ranging from 4.7% for renal insufficiency or failure to a maximum of 78.5% for breast cancer. Notably, 7 of the 17 conditions we studied had an estimated problem list completeness of less than 50%.11 Documentation gaps on the problem list have important downstream effects. In particular, the problem list enables CDS, with one study estimating that over 22% of all decision support rules rely on the coded problem list.12 As a result, documentation gaps have the potential to impact quality of care.13 14
In the specific case of splenectomy, the risks posed to patients lacking proper documentation are not theoretical. In previous work,15 we described a case at Partners HealthCare, when a splenectomy patient without proper documentation of the procedure on their medical record did not receive the recommended pneumococcal vaccinations following their splenectomy. Subsequently, they developed pneumococcal sepsis and lost multiple digits.
In response to this case, we reassessed the protocols and systems that were in place at our organisation to ensure, as best we could, that splenectomy patients received proper care following their splenectomy. During this assessment, we identified two EHR-related problems that contributed to this issue: a lack of proper documentation of splenectomy on patient problem lists, and low compliance rates for CDS related to vaccinations for patients following a splenectomy.15 As a result, we developed multiple interventions aimed at improving splenectomy documentation within the EHR.
Methods
We developed two interventions to address gaps in the documentation of surgical splenectomy within our EHR: a PHD intervention and a CDS intervention. In previous work,15 we outlined the use of the PHD method to improve splenectomy documentation through the manual review of a filtered set of patient charts, borrowing from population health techniques to address ‘gap’ cases in bulk. Alongside that intervention, we developed a novel CDS intervention to improve splenectomy documentation on an individual patient level. Both interventions were implemented at Partners HealthCare within the Longitudinal Medical Record (LMR), a home-grown Office of the National Coordinator for Health Information Technology-Authorized Testing and Certification Body (ONC-ATCB) certified outpatient medical record that was used at Partners HealthCare. Here, we describe both the PHD and CDS interventions and assess their relative effectiveness and broader implications.
The PHD intervention
Through our PHD intervention, we aimed to address gaps in splenectomy documentation in bulk. To do so, we aimed to (1) identify a cohort of patients who may have had a splenectomy, but lacked proper documentation of the procedure on their chart, (2) manually review these charts to determine whether the patients had a previous splenectomy and (3) add splenectomy to patient problem lists when appropriate. To identify a cohort of patient charts for review, we used a previously developed natural language processing (NLP) algorithm for splenectomies to identify cases where splenectomy may have been documented in a provider note, but was not documented on the patient problem list.6 The algorithm had an estimated sensitivity of 64.1% and positive predictive value of 86.0%, which allowed us to identify surgical splenectomy patients with relatively high confidence. The algorithm is described in detail in our prior publication.6
The NLP algorithm was run on all provider notes for patients seen at our institution in the previous 3 years (July 2007 through July 2010), which produced a list of 4324 patient charts for review. These charts were manually reviewed by four internal medicine residents employed at Partners HealthCare in 2010 who reviewed the charts of these patients (for which they did not typically provide care) as part of a quality improvement programme, outside of their normal duties. The residents reviewed each of the 4324 charts of patients with a potential splenectomy and, if appropriate, added splenectomy to the patient’s problem list. Residents reviewed charts between July and December 2010. Because the work was performed in addition to the residents’ normal duties, and for patients they did not otherwise care for, the residents were paid $1.45 for each chart they reviewed.
In a separate effort, another quality improvement programme within the Partners HealthCare network made an effort to augment splenectomy documentation within the EHR between August 2013 and October 2013. Documentations resulting from this effort were analysed separately, but the results were excluded because their effort did not stem directly from our intervention.
The PHD intervention was conducted as part of a quality improvement project at Partners HealthCare and was not required to be reviewed by our institutional review board.
The CDS intervention
In previous work, we demonstrated the efficacy of CDS alerts to improve problem list documentation within the EHR.16 Given the effectiveness of this intervention, we sought to develop CDS alerts to improve the documentation of splenectomy within the EHR. To do so, we aimed to (1) identify patients who had previously undergone a splenectomy, but lacked proper documentation of the procedure on their chart, (2) alert providers to potential documentation gaps through CDS alerts integrated within the provider workflow and, (3) when appropriate, directly add splenectomy to patient charts through provider acceptance of the CDS alerts. To identify patients to target for the CDS intervention, we developed a ‘procedure inference algorithm’ as an automated method of identifying patients who had previously undergone a splenectomy. The algorithm identified patients who had been billed for a splenectomy (as indicated by the CPT (Current Procedural Terminology) codes, ICD-9 (International Statistical Classification of Diseases and Related Health Problems 9th Revision) procedure codes and DRG (diagnosis-related group) codes for splenectomy in table 1) on or before 23 January 2012. Using this logic, we identified 3517 patients who were potential candidates for CDS alerts.
Billing codes used to identify splenectomy patients for CDS alerts
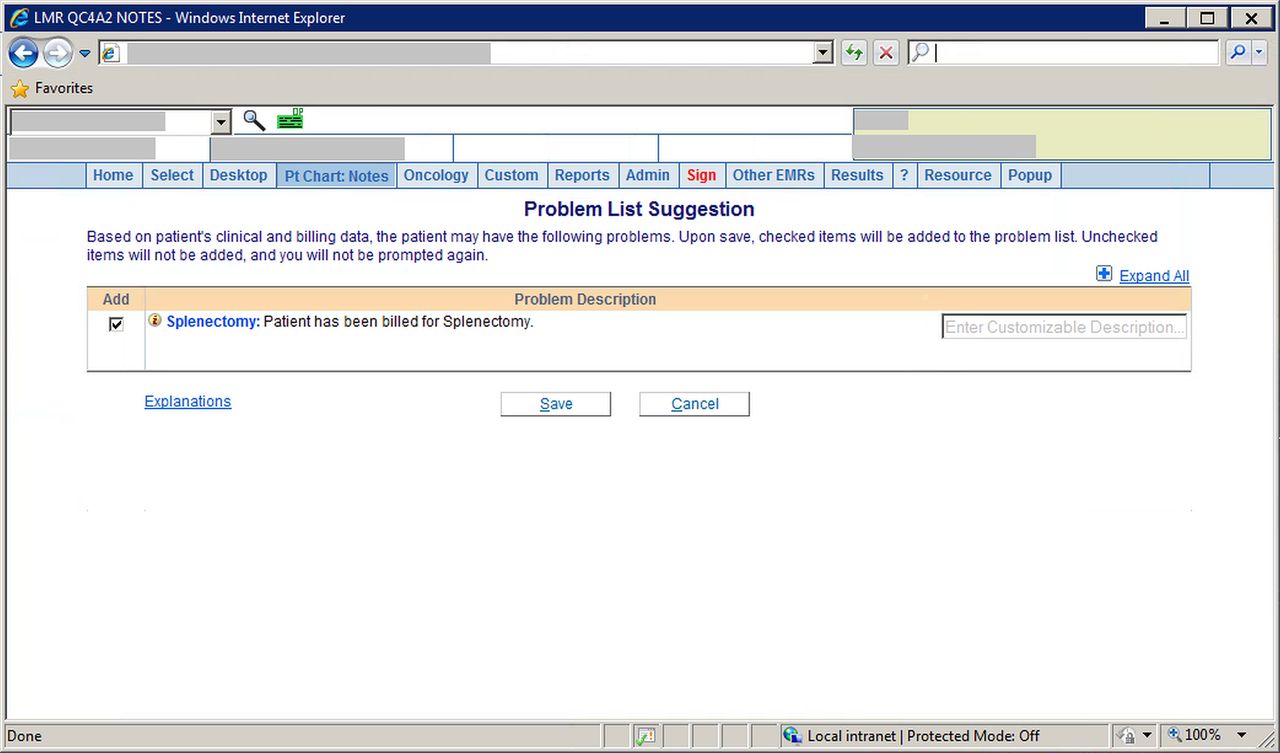
CDS alerts were then generated when an outpatient provider attempted to write a note on the chart of one of these patients who also lacked previous documentation of splenectomy on their problem or procedure list. The alert suggested adding splenectomy to the patients’ procedure list, and could be accepted (automatically adding splenectomy to the procedure list), overridden (suppressing the alert for 1 year) or cancelled (suppressing the alert for the current encounter only) (figure 1). Alerts went live within the LMR in August 2012. We collected data on splenectomy documentations that resulted from the CDS intervention through May 2015. The CDS intervention was reviewed and approved by the Partners HealthCare Human Subjects Review Committee.

Screenshot of the clinical decision support alert for splenectomy.
Comparison of methodologies
To assess the impact of both the PHD and CDS interventions on splenectomy documentation, data were collected on the number of splenectomy procedures added to patient problem lists at Partners HealthCare between February 2008 and May 2015. Using a negative binomial regression model, we compared the rate of splenectomy during both interventions to the baseline rate of splenectomy documentation to assess the impact of the interventions on splenectomy documentation.
Results
In the time when neither the CDS nor the PHD interventions were live, splenectomy was documented on 27.4 charts per month. Both the PHD and CDS interventions led to a significant (p<0.001) increase in the rate of splenectomy documentation within our EHR. Figure 2 shows the rate of splenectomy documentation from February 2008 through May 2015, with the CDS and PHD interventions indicated.

Splenectomies documented per month, February 2008 to May 2015. CDS, clinical decision support; PHD, population health documentation.
PHD intervention
The PHD intervention was carried out between July 2010 and December 2010. During that time, residents reviewed each of the 4324 charts flagged by our NLP algorithm as potentially requiring splenectomy documentation, and added splenectomy to 2668 (61.7%) charts. In this period, splenectomy was documented on 477.2 patient charts per month which was significantly greater than the baseline splenectomy documentation rate of 27.4 charts per month (p<0.001).
CDS intervention
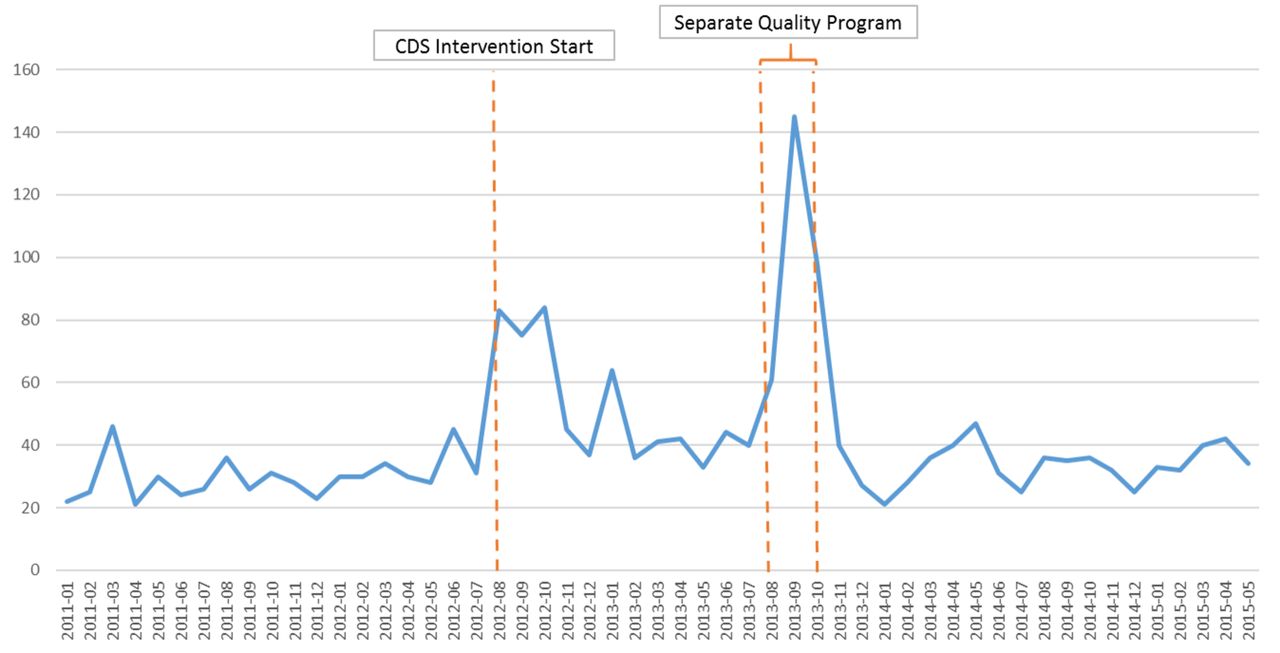
The CDS intervention went live in August 2012 with 3517 patients eligible for alerts based on the presence of splenectomy billing codes on their chart. From the go-live until 31 May 2015, 354 of these patients triggered a CDS alert and 248 (70.1%) had splenectomy added to their chart directly from the alert. This led to a significant increase in the splenectomy documentation rate during the CDS intervention period. Over the course of the CDS intervention, splenectomy was documented on 1264 patient charts, a rate of 40.8 charts per month. This was significantly greater than the prior documentation rate of 27.4 charts per month (p<0.001). As shown in figure 3, splenectomy documentation initially spiked following the CDS intervention go-live, but gradually fell towards the prior documentation rate. This is likely because the current billing data for splenectomies (which were stored outside of the LMR) were not updated in the EHR after the CDS intervention first went live. Thus, incident splenectomies after go-live were not captured. While this was a limitation of our particular implementation, in a fully integrated EHR and billing system ongoing splenectomy billing codes could be captured in real time and, in theory, the CDS intervention could continue to support the splenectomy documentation rate.
{kind=link}
{kind=link}
{kind=link}
Splenectomies documented per month, January 2011 to May 2015. CDS, clinical decision support.
Comparison of methodologies
A head-to-head comparison of the impact of the PHD intervention and the CDS intervention is challenging given that the interventions did not occur simultaneously, particularly since there was a backlog of undocumented splenectomies which was addressed, at least in part, by the PHD intervention prior to the CDS intervention going live. At baseline, only approximately 30% of splenectomy patients had splenectomy properly documented on their chart.6 A portion of this documentation gap was addressed during the months the PHD intervention was live, and thus, there was greater potential for impact on splenectomy documentation (i.e., fewer splenectomy patients had it documented on their chart) at the start of the PHD intervention than at the start of the CDS intervention. As a result, conclusions about the relative impact of these interventions should be made with caution.
Despite these cautions, it is likely that the PHD intervention had a larger impact on splenectomy documentation than the CDS intervention given the magnitude of the difference in number of splenectomy procedures documented during the two interventions. In the 6 months in which the PHD intervention was active, splenectomy was documented on 477.2 charts per month—many more than the 64.7 charts per month on which splenectomy was documented in the first 6 months that the CDS intervention was live.
Discussion
Our results demonstrate that both CDS and PHD interventions can have a significant impact on documentation gaps for procedures within the EHR. While our results are specific to splenectomy documentation, they can easily be extended to documentation of other problems and procedures. In previous work, we developed inference algorithms for 17 conditions, including heart failure, hypertension and coronary artery disease.11 Applied as CDS alerts, these algorithms led to significant increases in problem list documentation.16 Using similar algorithms to identify patients, we believe that PHD extensions of these interventions could have a similar impact on the documentation of these problems. Documentation of these problems on patient problem lists has important implications for patient care, including enabling CDS for these conditions. Examples include checks for ACE inhibitors or angiotensin II receptor blockers for patients with heart failure, antihypertensive medications for patients with hypertension and aspirin for patients with coronary artery disease.
Beyond documentation, similar approaches could also be used for diagnosis, screening, selection of appropriate therapy and follow-up of abnormal results. For example, an abnormal mammogram without appropriate follow-up could be set to trigger an alert during routine clinical care, and also be brought to the attention of a centralised result management group using a report—that group could then initiate follow-up directly, or contact the clinicians involved.
Given our results and these extensions, we discuss several important implications for problem list management, problem list ownership and for the design of CDS and EHRs.
PHD versus CDS interventions
Proper documentation of problems and procedures within the EHR has implications for patient safety and quality of care13 14 17 and is incentivised by the meaningful use of financial incentive programme for EHR use in the USA.18–20 Given the importance of addressing gaps in problem and procedure list documentation, the relative effectiveness of the PHD and CDS interventions should be assessed. Our results suggest that PHD interventions are more efficient in addressing gaps in splenectomy documentation, but given their reliance on manual chart review (which is known to be costly, time consuming and labour intensive, with previous studies estimating that a single chart review can take over 13 minutes21) they are more expensive than CDS interventions. In addition, PHD interventions create an ongoing cost in that their implementation requires financial incentives for the individuals reviewing and updating patient charts. In a fully integrated EHR and billing system, CDS interventions can be implemented with a single upfront cost and minimal maintenance costs (although there is also a difficult-to-measure cost of additional work for providers receiving alerts, as well as a potential cost of alert fatigue). Further, PHD interventions do not directly engage providers caring for the patient. While this is advantageous relative to CDS in that it does not further burden busy providers, taking the responsibility of problem list documentation away from physicians may negate some of the positive effects of problem list documentation. A summary of the strengths and weaknesses of both the PHD and CDS interventions can be seen in table 2.
Comparison of PHD and CDS interventions
In comparing patient-focused interventions (such as the CDS intervention) and population-based interventions (such as the PHD intervention) to support documentation in the EHR, it is useful to consider how these strategies are used to improve compliance with recommended care. As an example, consider how these strategies may be used to improve pneumococcal vaccination rates. A population-based strategy might involve a resident or non-physician health professional reaching out to all patients who are due for a pneumococcal vaccine, who would be identified using patient registries or data from the EHR. Meanwhile, a patient-specific intervention might use incentives for providers or CDS alerts within the provider workflow to encourage providers to offer indicated pneumococcal vaccination to patients during routine visits. These strategies have similar strengths and weaknesses to the PHD and CDS interventions to support EHR documentation. Both population-focused interventions address ‘gap’ cases as a population as opposed to individually, which is likely more efficient, but more labour intensive than patient-focused interventions to address gap cases. Meanwhile, both patient-focused interventions address gap cases individually, during the routine course of care. While these strategies are less labour intensive and occur during typical workflows, they also add one more item to an already long list of competing demands that providers must address when caring for patients.
In the example of pneumococcal vaccination, the patient and population-based strategies are complementary. Population-based strategies can efficiently address large gaps in patient vaccinations at once, while patient-focused interventions can prevent new gaps in vaccination rates from forming by addressing gap cases on an ongoing basis, during the routine course of care. A similar argument can be made for documentation interventions within the EHR. Large gaps in documentation exist within the EHR due to several factors including poor EHR usability and design which undoubtedly impact physician documentation rates. To address these gaps, PHD interventions appear to be more efficient and less interruptive than CDS interventions. Further, asking physicians to improve their documentation within the EHR would prevent future gaps from forming. Our results show that CDS can assist in improving documentation on individual patient charts, thereby demonstrating the symbiosis between the two strategies: PHD interventions close existing documentation gaps while CDS interventions prevent new gaps from forming.
As an example, consider again the specific case of splenectomy. Patients who have had a splenectomy only have it documented about 30% of the time, per our previous estimates.6 Over time, the total number of undocumented splenectomy patients increases as more patients are seen within the health system. Given our results, we feel that the PHD intervention is best suited to address the initial documentation gap given its efficiency. However, the CDS intervention appears to be a good strategy to prevent future gaps in splenectomy documentations from forming because it addresses potentially undocumented splenectomies during the routine patient care workflow. Thus, implemented together, the strategies are symbiotic, closing initial documentation gaps efficiently and preventing new gaps from forming over time.
Expanding beyond physicians for PHD interventions
Within the PHD intervention, residents were asked to review charts and document splenectomy where appropriate. However, this task may not truly require a physician’s expertise. The process of reviewing charts for splenectomy (or other problems or procedures) is relatively simple—it involves reviewing physician notes to determine whether or not there has been previous documentation of the problem or procedure. While there are undoubtedly borderline cases in which documentation is unclear, the vast majority of charts will be distinctly binary—either a patient has had the problem or procedure, or they have not. Thus, asking non-physician health professionals (such as practice managers, population health managers or research assistants) to complete this task may be a cheaper, and more efficient (assuming time is more readily available for non-physicians) means of implementing PHD interventions. However, in certain circumstances, physician documentation may be more useful for substantiation of billing than non-physician documentation, so this must be weighed in the cost analysis.
Implications for problem list ownership
Our study suggests that residents (and potentially non-physician health professionals) can improve documentation of patient problems and procedures within the EHR. This finding is in accord with previous work in which we found that shared responsibility and ownership of the problem list correlated with higher problem list completeness.17 As a result, it is reasonable to question whether or not a patient’s primary care physician (PCP) should be responsible for their problem list given the bevy of other patient concerns they must address. Given our findings, we argue for the expansion of shared responsibility regarding problem list ownership, although we acknowledge the need for more research in this area. Although PCPs are often viewed as the owners of a patient’s problem list,17 our work suggests that problem lists can be better maintained and more complete when problem list documentation is supported by specialist physicians, and even non-physicians such as population health managers. Particularly when facilitated by PHD interventions, expanding problem list responsibility to include both physicians and non-physician health professionals may lead to more accurate and up-to-date problem and procedure lists.
Limitations
This project has several important limitations. First, our CDS intervention did not incorporate billing codes to identify additional gap cases on an ongoing basis. While this limitation would not impact a fully integrated EHR and billing system, it was a limitation of our work since the billing system was, at the time, separate from the EHR. Second, given that the PHD and CDS interventions did not occur simultaneously, it is difficult for a direct one-to-one comparison of the two interventions. While we feel that the magnitude of the difference in the number of documentations from each method highlights the efficiency of the PHD method, it is difficult to confirm this efficiency relative to the CDS intervention given how the interventions were carried out. Third, neither the CDS nor the PHD intervention takes full advantage of available EHR data, and thus neither achieve their optimal sensitivity. The CDS intervention only captures patients who had their splenectomy within our network as it relies on billing codes from our network. On the other hand, the PHD intervention relies on the splenectomy being documented in a provider’s note and thus may miss splenectomy patients without notation of the procedure in provider notes. Ideally, the CDS intervention could incorporate NLP data to supplement billing data while the PHD intervention could supplement note data with billing data. This would represent an ideal state for both interventions. Finally, this project was conducted at a single institution to supplement the documentation of a single procedure. Although we believe that this work can be extended to other procedures and conditions at other healthcare organisations, it is difficult to determine how well our conclusions will generalise to other settings.
Conclusion
CDS alert interventions and PHD interventions both represent effective strategies to improve documentation of problems and procedures within the EHR. These strategies may best be used in conjunction to create a symbiotic relationship in which current problem and procedure documentation gaps are closed using PHD strategies, while new gaps are prevented using ongoing CDS interventions. Healthcare organisations should consider dedicating resources towards PHD interventions given its demonstrated efficacy in improving documentation gaps in the EHR.
References
Footnotes
Contributors DSM assisted in the analysis and interpretation of data and drafted the initial draft of the manuscript with supervision from AW. TG designed and oversaw the population health documentation intervention. AT designed and validated the natural language processing algorithm used for the population health documentation intervention. AW designed and conducted the clinical decision support intervention. All authors provided critical revisions to the manuscript, approved the final version of the manuscript and take responsibility for the integrity and accuracy of this work.
Competing interests None declared.
Ethics approval Partners HealthCare Human Subjects Committee.
Provenance and peer review Not commissioned; externally peer reviewed.