Emerging Patient-Driven Health Care Models: An Examination of Health Social Networks, Consumer Personalized Medicine and Quantified Self-Tracking

Abstract
:
1. Introduction
1.1. Scope of Analysis
2. Emerging Patient-Driven Health Care Models
2.1. Health Social Networks
2.2. Consumer Personalized Medicine
2.2.1. Consumer personalized medicine introduction
2.2.2. Consumer personalized medicine definition
2.2.3. Categories and types of consumer personalized medicine
Personalized genomics
Direct-to-consumer blood and other biomarker tests
Environmental testing
Predictive biosimulation
2.3. Quantified self-tracking
2.3.1. Quantified self-tracking introduction
2.3.2. Quantified self-tracking definition
2.3.3. Categories and types of quantified self-tracking tools
2.3.4. Categories and types of environmental tracking tools
3. Discussion of Emerging Patient-Driven Health Care Models
3.1. The Future of Health Care and the Evolving Health Care Delivery Model
3.2. The Evolving Role of the Patient
3.3. The Evolving Role of the Physician
3.4. The Advent of Health Social Networks as Influence Entities
3.5. Changing Legal, Economic and Regulatory Institutions
3.6. The Future of Clinical Trials: Vertical and Horizontal Stratification
3.7. Changing Drug Discovery and After-Market Studies
3.8. Discussion Summary of Emerging Patient-Driven Health Care Models
4. Conclusions
4.1. Summary and Opportunity
Figures and Tables
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Legend: | QS: quantified self-tracking |
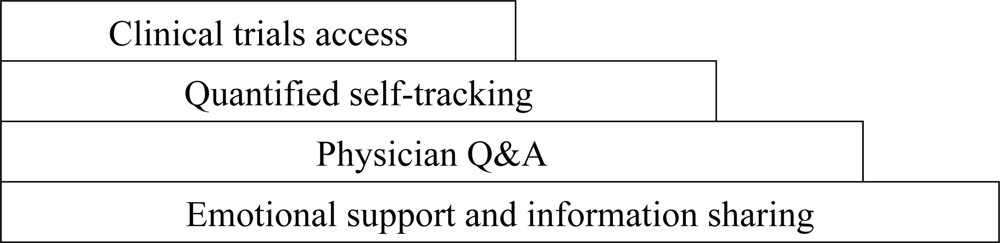
| ES&IS: emotional support and information sharing | CT: clinical trials access |
| Q&A: physician Q&A | N&I: networking and information |
| Name and URL | Focus | Services |
|---|---|---|
| General health social networks | ||
| PatientsLikeMe
http://www.patientslikeme.com | General: 16 conditions, ex: ALS, MS, HIV/AIDS | ES&IS, QS, CT |
| CureTogether
http://www.curetogether.com | General: 175 conditions, ex: endometriosis, migraine | ES&IS, QS |
| MedHelp
http://www.medhelp.org | General: tracking, physician Q&A | ES&IS, Q&A, QS |
| Inspire
http://www.inspire.com | General: over 1,000 health and wellness groups, journaling | ES&IS, CT |
| DailyStrength
http://www.dailystrength.org | General: 600+ conditions | ES&IS |
| OrganizedWisdom
http://www.organizedwisdom.com | General: 60 conditions, referenced research citations | ES&IS |
| WellSphere
http://www.wellsphere.com | General: 50+ communities, ask an MD feature | ES&IS, Q&A |
| MDJunction
http://www.mdjunction.com | General: 750+conditions, physician listings and marketplace | ES&IS, Q&A |
| ehealth forum
http://ehealthforum.com | General: physician Q&A; 1.2M questions logged on the site | ES&IS, Q&A |
| HealthChapter
http://www.healthchapter.com | General: 715 groups | ES&IS |
| Trusera
http://www.trusera.com | General: 23 main topic areas | ES&IS |
| iMedix
http://www.imedix.com | General: information, support and answer response | ES&IS, Q&A |
| Wellescent
http://www.wellescent.com | General | ES&IS |
| WeGoHealth
http://www.wegohealth.com | General: answer response from health activists | ES&IS, Q&A |
| Experience Project
http://www.experienceproject.com | General: members, stories, discussions | ES&IS |
| Peoplejam
http://www.peoplejam.com | General | ES&IS |
| Cause-specific health social networks | ||
| TuDiabetes, http://tudiabetes.com dLife, http://www.dlife.com SugarStats, http://www.sugarstats.com | Diabetes; SugarStats offers self-tracking | ES&IS
ES&IS ES&IS, QS |
| Prostate Cancer Info Link
http://prostatecancerinfolink.ning.com | Prostate cancer | ES&IS |
| I’m Too Young for This
http://www.imtooyoungforthis.org | Youth with cancer | ES&IS |
| CareFlash, http://www.careflash.com Care Pages, http://www.carepages.com | Personal webpages to share health updates with family and friends | ES&IS |
| WeAreDiabetic.org, WeAreCeliac.org
http://weare.us | General/support: 14 communities | ES&IS |
| Physician social networks | ||
| Sermo
http://www.sermo.com | General: free membership to verified physicians | N&I |
| Medscape Physician Connect
http://www.medscape.com http://tiny.cc/pRhuj (detail) | General: free membership to verified physicians | N&I |
| Asklepios
http://www.asklepios.ca | General: Canadian physician networking and collaboration tool | N&I |
| MedicalExchange MEDTING
http://www.medting.com | Online research, publishing and case collaboration with images and videos | N&I, Collaboration |
| OR-Live
http://www.or-live.com | Online surgical and health care video and webcast communication platform | N&I, Collaboration |
| The Doctor’s Channel
http://www.thedoctorschannel.com | Doctors learning from each other via short streaming video clips | Education |
| Additional medical industry physician and scientist social networks:
http://scienceroll.com/2008/05/24/community-sites-for-scientists-and-physicians-the-list | ||
| Service | Function |
|---|---|
| Trixie Tracker
http://www.trixietracker.com | Track and display the activity patterns of babies; sleeping, eating, diaper changes, etc. (website) |
| MyMonthlyCycles
http://mymonthlycycles.com Mon.thly http://mon.thly.info Ovulation.com http://www.ovulation.com | Track menstrual cycles, use fertility calendars (websites and smartphone (iPhone, G1) applications) |
| BedPost
http://www.bedposted.com | Measure sex frequency, duration, quality (website) |
| Tweet what you eat!
http://www.tweetwhatyoueat.com | Maintain a food diary with updates through SMS text messages, instant messages or web input. Calorie count suggestions come from a crowd-sourced database (website) |
| Zume Life’s Zuri
http://www.zumelife.com | Generate medical reminders and track medication, biometrics, food, exercise and health status. Customized health tracking via a speech transcription service (website, device and iPhone application) |
| Keas
http://www.keas.com | Highly personalized full health and wellness profiles, ongoing lab results, custom questionnaires and interaction with physicians and other health providers (website, due to launch in 2009) |
| Product | Functions | Connectivity | Pricing | Availability |
|---|---|---|---|---|
| FitBit
http://www.fitbit.com 2 inch belt unit | Energy expenditure, sleep measurement | Wireless | $99 one-time fee including device + ongoing website access | Available Q1 2009 |
| GoWearFit
http://www.gowearfit.com Arm band + display watch | Energy expenditure, sleep measurement | USB | $159.95 + $6.95/month website subscription fee | Available now |
| Bodybugg
http://www.bodybugg.com Arm band + display watch | Energy expenditure | USB | $249 + $14.95/month website subscription fee | Available now |
| WalkingSpree
http://www.walkingspree.com Pedometer | Energy expenditure | USB | $99.95 | Available now |
| ActiHealth
http://www.actihealth.com | Blood pressure, weight, activity | USB, Bluetooth | $130 pedometer | Not yet available |
| Tanita
http://www.tanita.com/radiowirelessscales.shtml | Wireless bathroom scales | Bluetooth | $249.99 | Available now |
| OrSense
http://www.orsense.com | Non-invasive spot and continuous glucose monitoring | Manual | N/A | Not yet available |
| Kickbee
http://portfolio.menscher.com/itp/kickbee | Tracking of baby kicks from the womb | Sensor, Bluetooth | N/A | Not available commercially |
References
- Cassman, M; Arkin, A; Doyle, F; Katagiri, F; Lauffenburger, D; Stokes, C. Systems Biology: International Research and Development, 1st Ed ed; Springer: New York, NY, USA, 2007; pp. 3–10. [Google Scholar]
- Anderson, C. The End of Theory: The Data Deluge Makes the Scientific Method Obsolete. WIRED Magazine. 2008.
- Brockman, J (Ed.) Engineering Biology: A Talk with Drew Endy. Online text from Edge: The Third Culture series ‘Life What a Concept!’. 2008.
- Hill, CT. The Post-Scientific Society. Issues in Science and Technology. 2007.
- Arnst, C. Health 2.0: Patients as Partners. Business Week. 2008.
- Ibid.
- Eysenbach, G. Medicine 2.0: Social Networking, Collaboration, Participation, Apomediation, and Openness. J. Med. Internet Res 2008, 10, 5–6. [Google Scholar]
- Frost, JH; Massagli, MP. Social Uses of Personal Health Information Within PatientsLikeMe, an Online Patient Community: What Can Happen When Patients Have Access to One Another’s Data. J. Med. Internet Res 2008, 10, e15. [Google Scholar]
- Arnst, C. Health 2.0: Patients as Partners. Business Week. 2008.
- Wicks, P. PatientsLikeMe for ALS/MND. Presented at the 18th International ALS/MND Symposium, Toronto, Canada, December 1–3, 2007.
- Wicks, P. Parkinson’s disease: more non-motor symptoms for younger sufferers.
- Wicks, P; Massagli, M; Wolf, C; Heywood, J. Measuring function in advanced ALS: Validation of the ALSFRS-EX extension items. European Journal of Neurology. 2009.
- Arnst, C. Health 2.0: Patients as Partners. Business Week. 2008.
- Fornai, F; et al. Lithium delays progression of amyotrophic lateral sclerosis. Proc. Natl. Acad. Sci. U.S.A 2008, 105, 2052–2057. [Google Scholar]
- Carlson, R. Cost Per Base of DNA Sequencing and Synthesis. Online image from the ‘Synthesis’ blog.
- Svendsen, B. Premium genome mapping service. Online text from the ‘Springwise’ blog.
- Anonymous. 23 and Me and the Parkinson’s Institute Announce Initiative to Advance Parkinson’s Disease Research. Online text from ‘Parkinson’s in the News,’. 14 May 2008.
- Anonymous. The scent of a woman (and a man). The Economist. 2008.
- Winslow, R. FDA to Use Simulation Technology for Drug Testing. Wall Street Journal. 2008.
- Hesse, M. Bytes of Life: for every move, mood and bodily function, there’s a web site to help you keep track. The Washington Post. 2008.
- Brophy-Warren, J. The New Examined Life: Why more people are spilling the statistics of their lives on the Web. The Wall Street Journal. 2008.
- Anonymous. Remote Monitoring of Pacemaker Patients on Medtronic Carelink(R) Network Detects Clinically Actionable Events More Quickly Than Combination of Transtelephonic Monitoring and Routine Office Visits. Reuters. 2008.
- Charles, C; Whelan, T; Gafni, A. What do we mean by partnership in making decisions about treatment? Brit. Med. J 1999, 319, 780–782. [Google Scholar]
- Gorman, JM; den Braber, M. Semantic Web Sparks Evolution of Health 2.0 – A Road Map to Consumer-Centric Healthcare. Presented at the Health 2.0 Unconference, Amsterdam, Netherlands, April 12, 2008; pp. 1–2.
- Moore, K. King’s commentary on genome testing. Online text from the King’s College London ‘News archive 2008,’. 6 November 2008.
- Lewis, R. DNA Masters. Nature 2007, 449, 940–941. [Google Scholar]
- Tapscott, D; Williams, AD. Wikinomics, 1st Ed ed; Penguin Group: New York, NY, USA, 2006; pp. 7–9. [Google Scholar]
- Charles, C; Whelan, T; Gafni, A. What do we mean by partnership in making decisions about treatment? Brit. Med. J 1999, 319, 780–782. [Google Scholar]
- Magee, M. Home Centered Health: Part 1 What will it take to create the ideal healthy home?
- Bosworth, A. A Modest Proposal: New Products and Services to Fix Health Care. Presented at the Connected Health Symposium, Boston, MA, USA, October 28, 2008.
- Bensinger, G. Corporate wellness, Safeway style. San Francisco Chronicle. 2009.
- Charles, C; Whelan, T. Gafni, A. What do we mean by partnership in making decisions about treatment? Brit. Med. J 1999, 319, 780–782. [Google Scholar]
- Vogt, E; Kuperberg, J. Creating a Partnership Model for Health Education and Health Care. Presented at the 1996 Partnerships for Networked Consumer Health Information Conference, Racncho Mirage, CA, USA, May 12–14, 1996.
- Luque, L; Basagoiti, I; Johnsen, E; Karlsen, R. Study of the ePatient as a provider of health content in the Internet. Presented at the Medicine 2.0 Congress, Toronto, Canada, September 4–5, 2008.
- Millar, J. A Shared Care Model for Complex Chronic Disease Care: A Community of Practice. Presented at the PHSA Navigation Workshop, Vancouver, British Columbia, Canada, February 23, 2004; pp. 9–10.
- Charles, C; Whelan, T; Gafni, A. What do we mean by partnership in making decisions about treatment? Brit. Med. J 1999, 319, 780–782. [Google Scholar]
- Parker-Pope, T. Are patients swimming in a sea of health information? Or are they drowning in it. The New York Times. 2008.
- Waldrop, M. Science 2.0: Great New Tool, or Great Risk. Scientific American. 2008.
- Hughes, B. To 2.0 or not to 2.0 – have junior doctors already answered the question? Presented at the Medicine 2.0 Congress, Toronto, Canada, September 4–5, 2008.
- Mesko, B. Medical education and building an on-line reputation in the world of web 2.0. Presented at the Medicine 2.0 Congress, Toronto, Canada, September 4–5, 2008.
- Anderson, J. Healthcare Uncovered. Online text, 2008.
- Young, L. Health Savings Accounts: More Time, Less Money. Business Week. 2008.
- Pollack, A. Gene Testing Questions by Regulators; New York Times, 2008.
- Crenson, M. 23andMe Statement in Response to Letter from California Department of Health. Online text from ‘The Spittoon’ blog. 6 July 2008.
- Pollack, A. California Licenses 2 Companies to Offer Gene Services. New York Times. 2008.
- Dimasi, JA; Grabowski, HG. The Cost of Biopharmaceutical R&D: Is Biotech Different? Manag. Decision Econ 2007, 28, 469–479. [Google Scholar]
Share and Cite
Swan, M. Emerging Patient-Driven Health Care Models: An Examination of Health Social Networks, Consumer Personalized Medicine and Quantified Self-Tracking. Int. J. Environ. Res. Public Health 2009, 6, 492-525. https://doi.org/10.3390/ijerph6020492
Swan M. Emerging Patient-Driven Health Care Models: An Examination of Health Social Networks, Consumer Personalized Medicine and Quantified Self-Tracking. International Journal of Environmental Research and Public Health. 2009; 6(2):492-525. https://doi.org/10.3390/ijerph6020492
Chicago/Turabian StyleSwan, Melanie. 2009. "Emerging Patient-Driven Health Care Models: An Examination of Health Social Networks, Consumer Personalized Medicine and Quantified Self-Tracking" International Journal of Environmental Research and Public Health 6, no. 2: 492-525. https://doi.org/10.3390/ijerph6020492