Article Text

Abstract
Background Apps can potentially support asthma self-management; however, attracting downloads and encouraging on-going adherence are challenging.
Objectives We observed the impact of different recruitment strategies and app features on adoption and continued use.
Methods Practice nurses in five practices in Lothian/Oxford approached adults with active asthma to try out a prototype app. We also advertised the app via social media (Asthma UK; AUK Centre for Applied Research). We observed patients’ download and retention rates and sent pre- and post-trial questionnaires. We sampled 15 patients for interviews before and after using our app for 1 month to explore motivations, triggers and barriers to adoption and usage. Interviews were transcribed and analysed thematically with reference to the Fogg behaviour model.
Results Social media attracted 87 users, but only 15 (17%) used the app for 30 days. Practices recruited 24 patients, 13 (54%) continued for 30 days. Successful adoption was dependent on ease of downloading and sufficient motivation. Some patients needed technological assistance with downloading the app and starting to use the features. Adherence was dependent on motivation derived from a sense that the healthcare professional and/or researcher was interested in the results, and that using an app to support their self-management could improve their asthma control.
Conclusion Social media attracted more downloads in a short time. However, most patients stopped using the app within a month. Practices attracted fewer downloads, but patents adhered longer to the app. Dual promotion strategies (social media with practice support) may be the optimal approach to encourage adoption and adherence to telehealth.
- asthma
- self-management
- telehealth
- mobile application
- social media
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Asthma is one of the most common long term conditions, affecting over 235 million people worldwide.1 It can be controlled by medications, but is ideally managed in the context of supported self-management, with an asthma action plan provided by clinicians explaining what to do when symptoms are worsening. However, few asthma patients have an asthma action plan2 despite overwhelming evidence that supported self-management improves asthma outcomes.3 Asthma action plans are usually paper-based but are easily mislaid. One solution is to incorporate them within a mobile app to facilitate availability when it is needed.
Adoption in relation to apps refers to the process of persuading – or triggering – someone to download an app. Adherence refers to the sustained use of an app, not necessarily every day but when needed. The Fogg behaviour model suggests that three core elements motivation, ability and a trigger must converge at the same time for a desired behaviour to take place.4 Motivation and ability can be traded off against one another, for example, patients may be willing to perform a difficult task if they are highly motivated by the promise of better health outcomes. Ability refers to the patients’ skill/dexterity with respect to downloading and using the app, which in turn, is related to the simplicity (or otherwise) of using the app. A trigger is a stimulus that prompts patients to adopt and use the app (e.g. an acute attack, an advertisement or clinician’s suggestion).
If app use is to contribute to supported self-management, it is important to understand how to increase motivation to use it, ensure the app is within patients’ ability to use and the impact of different types of trigger. To explore these challenges, we therefore developed a prototype app to support asthma self-management. We then observed the impact of different recruitment strategies on adoption and explored features associated with adoption and adherence to app usage.
METHODS
This study commenced in September 2016 and ended in July 2017, with the approval of the South East Scotland National Health Service Research Ethics Committees (NHS REC 02) and the National Health Service Health Research Authority (NHS HRA). The REC reference number was 16/SS/0101. All participants gave their fully informed consent.
Settings
Adults requiring medication to manage their asthma were approached to participate in this study via their primary care practice or via social media.
Primary care practice
Five UK primary care practices (four in Lothian; one in Oxford), each of which had at least one nurse who provided asthma care, participated in the study. At a training session, the nurses were provided with packs, including a practical guide on inviting patients to download and use the app, a log to record the gender and age of the patients to whom they gave information packs and contact details of the research team for queries.
Social media
The Facebook and Twitter platforms of Asthma UK and the Asthma UK Centre for Applied Research (AUKCAR) promoted the study. The messages included brief information and a link to information for patients on how to download the app (e.g. would you like to test an app that helps you manage your asthma better? [shortened URL], Need a helping hand to manage your asthma? Try our new app [shortened URL]). Asthma UK had 379,000 followers in Twitter5 and 66,665 followers in Facebook in August 20176; while the AUKCAR had 577 followers in Twitter7 in August 2017 (but no Facebook account).
App prototype
Based on our previous systematic review,8 a review of social forum discussions about the ‘wanted’ features of an asthma app9 and the advice of our lay and professional advisory groups, we developed a prototype app. With this app, patients could monitor (on a five-point scale) 10 aspects of their asthma status, including the Royal College of Physicians three-questions,10 use of reliever inhaler, use of preventer inhaler, nasal symptoms, smoking status and exercise level. Other features in the app included a current medication record, medication and task reminders, peak flow log, a free-text diary and a health report (that could be e-mailed to their practices). There was also an app tutorial and a facility to ask questions about the app. In addition, the app incorporated a blank asthma action plan, based on the Asthma UK action plan.11 Patients were advised that their general practitioner or asthma nurse could help to complete the action plan during their next review.
Patient recruitment
To explore the impact of different recruitment strategies on adoption of the app, we utilised three different approaches to invite patients to use the app for up to 3 months:
Practice recruitment: Practices used two strategies to recruit participants. Each practice invited people on their asthma register (randomly selecting 100 people in larger practices) by a letter to use the app and participate in the qualitative aspects of the research (Stream A). In addition, practice asthma nurses invited patients to try out the app by handing out information packs to patients who attended for a routine consultation during the course of the study by Stream B. Nurses were not expected to teach patients to download and use the app; technological support was provided by the research team and the app developer.
Social Media recruitment: Users of the Facebook and Twitter platforms of Asthma UK and AUKCAR were sent invitation messages which provided links to the project website (A4A: App for Asthma, ‘download instruction’ page) (Stream C).
After downloading the prototype app from the Google play store or Apple app store,12,13 patients were asked to enter the stream code A, B or C. Because there may be some overlap between these recruitment strategies (a few patients recruited via their practice might also receive a social media promotion; some attendees for a review might also receive a practice invitation letter), allocation was defined by the form of invitation to which the patient responded as determined by the instructions they were following. All patients completed an eligibility check (aged ≥16 years; with ‘active asthma’14; UK resident) and gave online consent for the research team to review their app usage. A short tutorial ‘popped up’ and they could then start to use the app. Technical support, such as an in-app enquiry message, enquiry email and enquiry hotline were provided by the research team and the app developer.
Data collection
Qualitative data collection
Fifteen patients from stream A were purposively sampled based on age, ownership of an action plan, previous experience of healthcare apps and invited to provide one-to-one interviews before and after using the app for a month in order to explore their reasons for adopting and continuing to use the app (or not). At least one GP, asthma nurse and member of the administration staff in each of the five practices were interviewed to explore the impact of the app on consultations and organisation of care. See Supplementary file B for the topic guides.
Quantitative data collection
From the Bitly online platform15 and Google analytics,16 we measured the number of hits on the ‘download instruction’ page, the number of registrations, on-going usage including pages accessed and data entered. Patients were invited to complete a pre-study questionnaire during online registration (rating ‘agree’, ‘neutral’ and ‘disagree’ on reasons for downloading the app) and a follow-up questionnaire on the 90th day (rating features that encouraged on-going use). See Supplementary file A for the questionnaires.
Data synthesis and analysis
Qualitative data analysis
Interviews were digitally recorded, transcribed and entered into NVivo for analysis. Framework analysis, informed by the Fogg behaviour model,4 was used to explore patients’ motivations, triggers and abilities to use the app prototype. Analysis was iterative so that insights from the early interviews informed the topic guide for later interviews and the 90-day questionnaire.
Quantitative data analysis
We assessed adoption and adherence numerically with the following parameters:
Number of registrations: The total numbers of patients who registered an account on our app database.
Adoption: The hit rate was calculated as the proportion of registrations to the number of people who received our information (A: the numbers of invitation letters sent to patients; B: the number of patients who took our information packs from the nurses and C: the number of unique views on our project webpage for download instruction).
Adherence: The retention rate was the proportion of registered patients who were still using the app after 30, 60 and 90 days.
Patients’ ratings on the pre-study and 90-day questionnaires were analysed using descriptive statistics to identify the reasons for downloading the app and the features that encouraged them to continue to use the app.
RESULTS
Patient recruitment from streams A, B and C
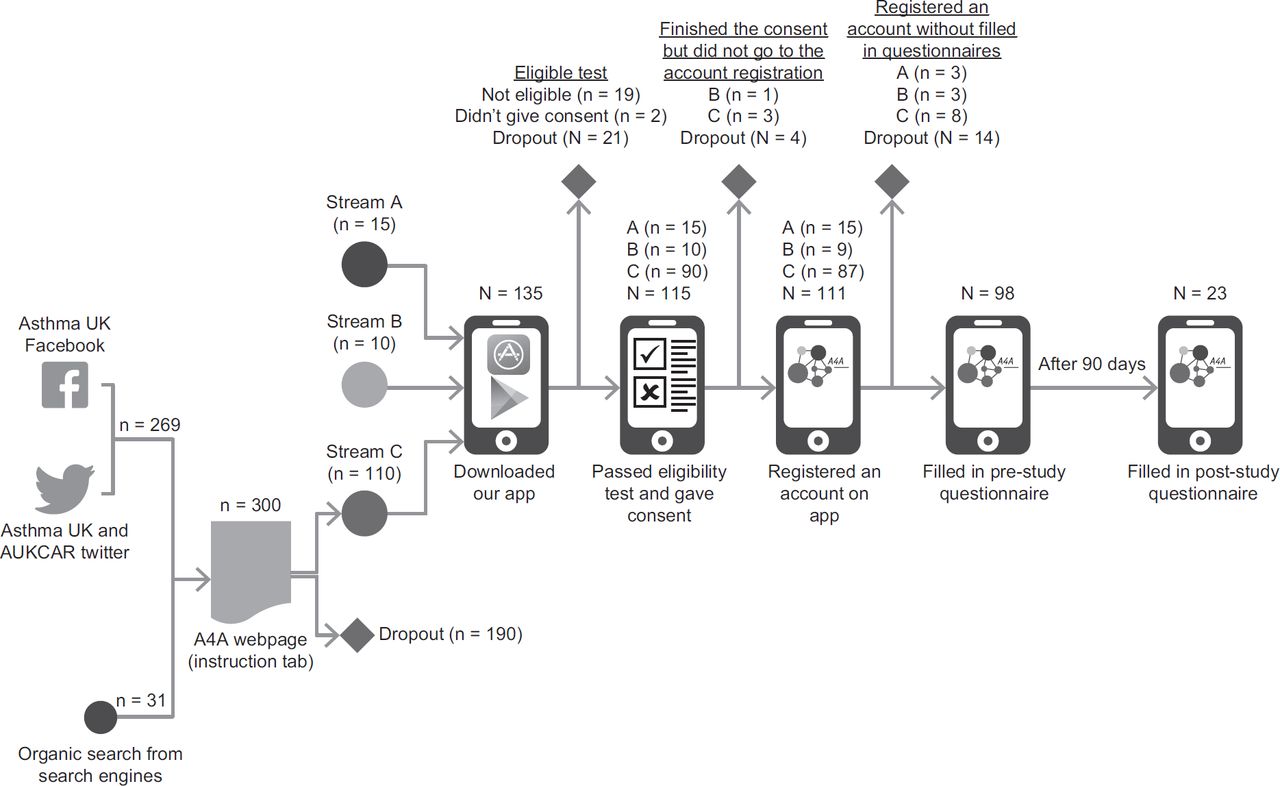
Figure 1 shows the flow of patients through the study.
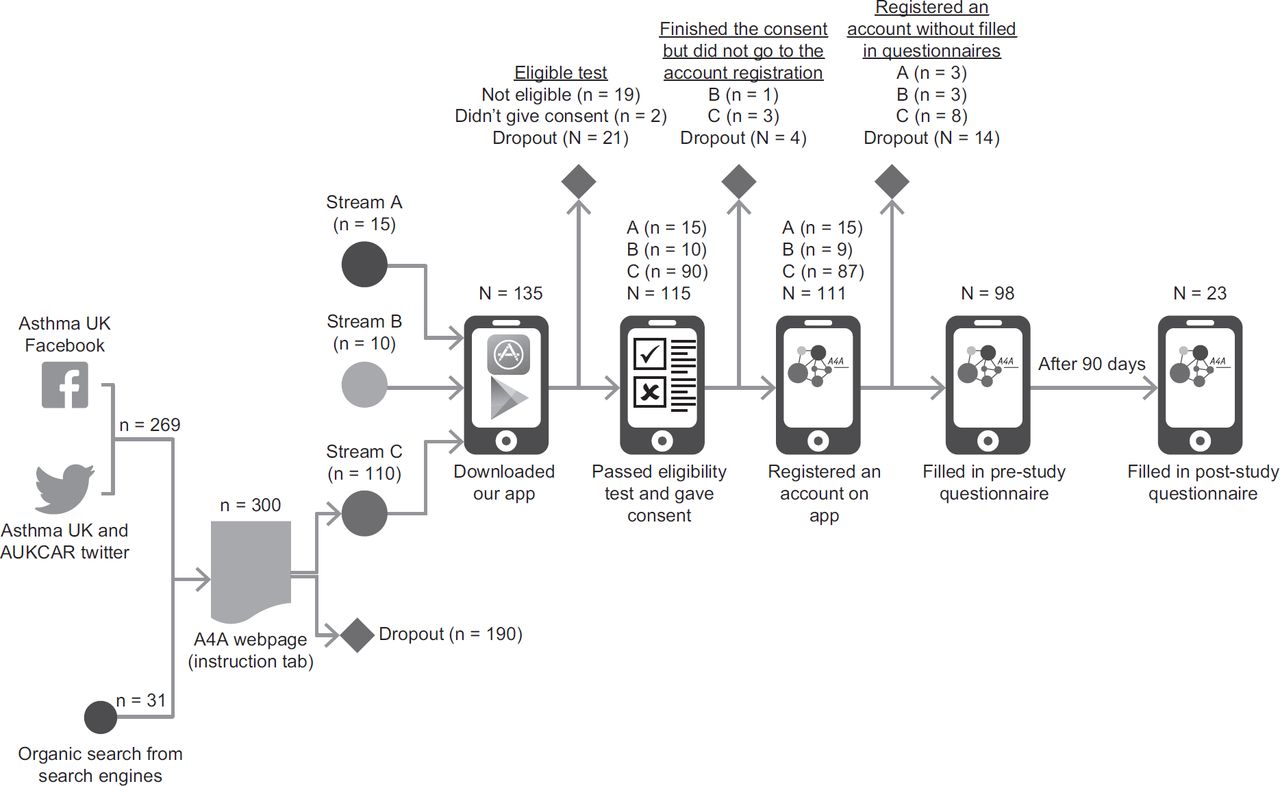
Stream A: Of a combined list of over 1757 asthma registered patients, 1115 met our inclusion criteria (≥16 years with active asthma14). Of these, 560 eligible patients were randomly selected by GPs and sent an invitation to participate. Twenty-eight (5.0%) patients agreed to participate. Most patients did not give reasons for not taking part: one declined because their asthma was well controlled and one had no smartphone. Fifteen respondees were purposively sampled to individual interviews. Three of the remaining patients not sampled for interviews joined stream B and used the app for 3 months.
Stream B: Of the eligible patients (≥16 years; active asthma.14) who attended their annual review during our study period, 48 accepted a pack from their asthma nurse during the consultation. Six (12.5%) subsequently downloaded the app prototype and registered an account on the app.
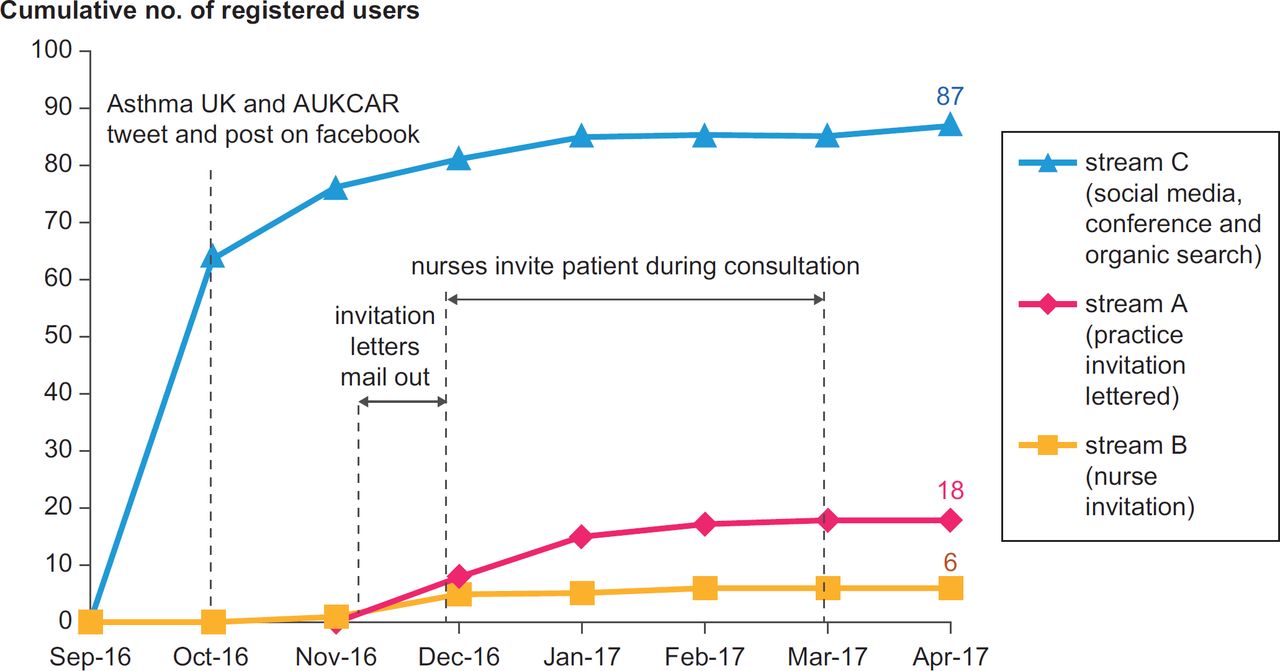
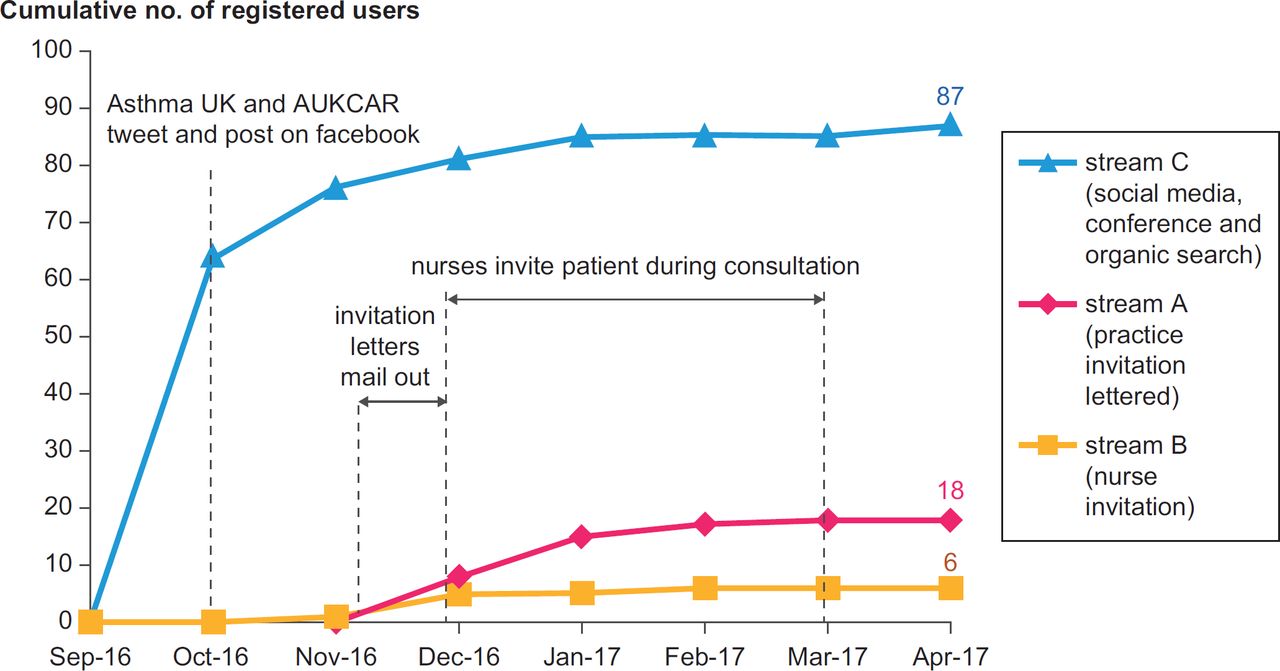
Stream C: Over 400,000 people are signed up to the Asthma UK Centre’s and AUKCAR’s social media. We had 300 unique views on the download page of our project website. The majority of these views came from clicking on our advertisements on Asthma UK and AUKCAR Facebook and Twitter (269/300, 90%); others arose from organic search as a result of hearing about the app from conferences or friends (31/300, 10%). Eighty-seven (29%) viewers passed our eligibility check (≥16 years; active asthma; registered with a UK general practitioner), downloaded and registered an account on the app.
A total of 111 patients were recruited. Of these, 101 patients provided (in the pre-study questionnaire) their age and gender; 98 completed the questionnaires, providing information such as action plan ownership, regular preventer medication usage and experience with digital devices and healthcare apps. Table 1 summarises the patients’ characteristics. Only 3% of patients had special needs (e.g. needing dyslexic friendly font) to use a smartphone.
Characteristics of patients for interviews
The characteristics of the 15 purposively sampled patients in the qualitative study are summarised in Table 1. The majority of patients were female over 26 years old and had not used healthcare apps before. Only five had a written action plan; five had been verbally told ‘what to do’ in the event of symptom deteriorations. Half were Android users and half Apple iOS users. All agreed to take part in pre-study interviews; however, one declined the post-study interview as she felt she had nothing more to tell us and one could not be contacted.
Adoption
The three different recruitment approaches (or ‘triggers’) elicited different response rates. Figure 1 shows the uptake from the three streams. We recruited far more people through social media than practice invitations (letter or verbally). Patients registered an account within days of releasing the advertisements on social media. Of 300 web-page views from social media, 87 (29%) registered to use the app; this ‘hit rate’ was higher than practices’ invitations [GP invitation letter: 18/560 (3.2%); nurses’ invitation in a review: 6/48 (12.5%)]. However, Asthma UK and AUKCAR social media have over 400,000 ‘followers’, so less than 0.1% were attracted to look at the website. The majority of participants (59%) were aged 26–45 years, female (87%) and had no healthcare app experience (82%).
We used the motivation, ability and trigger categories of the Fogg behaviour model4 to explore why patients downloaded our app prototype using data from the qualitative interviews, usage data and pre-study questionnaire.
Adoption: motivation
The key positive motivators described by interviewees were to help research, to improve their asthma by monitoring, to be reminded to take their medications and curiosity about what an app could do for their asthma. Some patients had more than one motivation for adoption.
it [taking part in this research] could be helpful for the medical, you know, studies or something. So to advance their work [Patient 3, 26–45, F]
The motivation is to see if I can improve it [their asthma], not to a level that I’m not prescribed inhalers anymore but to a better level [Patient 10, 26–45, F]
Curiosity is my main motivation [Patient 7, 65+, M].
Respondents to the pre-study questionnaire (see Table 2) agreed that being part of a research study and wanting to control asthma symptoms were key motivators; the offer of desirable features in the app was also rated as an important motivator. Almost 90% of patients agreed that being free of charge would encourage them to download the app. Being busy and having asthma under control were the key reasons given by interviewees for not downloading the app.
I think the reason (not to download) is that as you would have seen I’m exceptionally busy and so I tend to, I don’t use apps much. So, in fact, I probably only use about four in total. My asthma has been completely under control [Patient 13, 46–65, M].
Adoption: abilities
Most of the patients were able to download, activate and use the app prototype by themselves. Some (typically older) patients needed assistance; however, they could complete the download by following our email advice or by seeking help from younger family members. Their difficulties included (a) being unable to find the app on app stores (b) confusion with Google payment setup during download, (c) unsure about how to free-up their phone’s memory for downloading and (d) lacking confidence with technology.
Well I think that somebody younger would get it straight away but as I say I’m not very good with these things [Patient 2, 46–65, F].
Adoption: triggers
Most patients (93%) responding to the pre-study questionnaire indicated that they would download an app if it was recommended by their known and trusted health care professional; whereas two-thirds (67%) would respond to general advice from the NHS which they thought might not be applicable to them individually. Only half (51%) said they would respond to a generic recommendation from a commercial organisation with no relationship to their health such as Facebook, Twitter. From the observed recruitment (see Figure 2), only 12.5% registered after a personal invitation from their nurse though this compares to <0.1% who responded to the social media publicity.
The asthma nurses identified some challenges of recruiting people to use the app. Over the 3 months of the recruitment, they had review appointments for an estimated 300 patients, many of whom were children or ineligible for other reasons. Also, a significant proportion failed to attend the appointment they had made. Most of the patients who received the information showed interest in the app; however, few subsequently registered an account on the app.
So December, probably December into the middle of January we didn’t see many people with asthma so that’s maybe half of it [Practice nurse 1].
Adherence
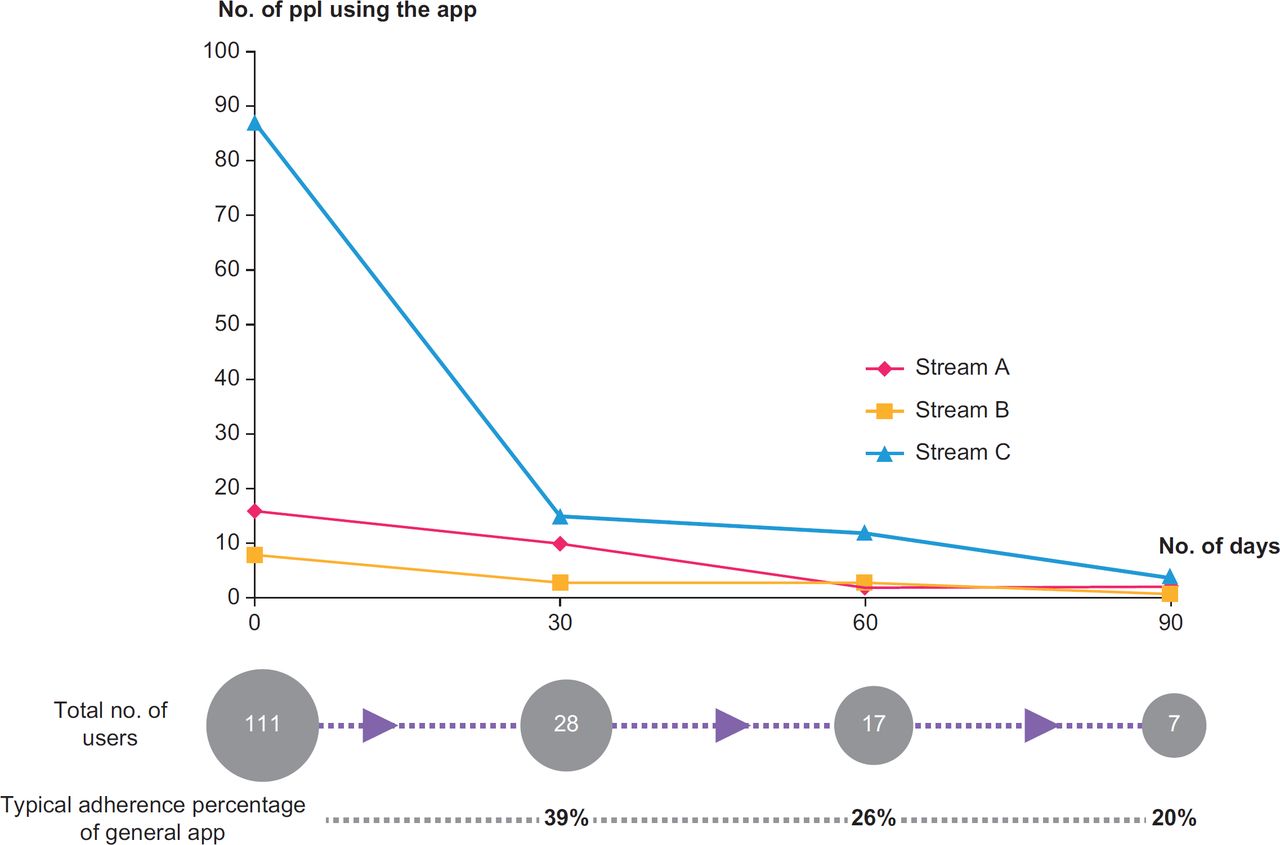
The usage of the app fell over time; only 25% of the participants were still using the app after 30 days. Patients from social media stopped using the app rapidly in the first 30 days from 87 to 15 participants: a reduction of 83%. The usage rates from practice-recruited patients also declined but less rapidly compared to that in the social media group. Those invited by the nurse in a review reduced by 63% and the ‘Practice letter’ group reduced by 38% (but the latter were involved in qualitative interviews at a month which may have influenced their decision to keep using the app). For comparison, the adherence pattern in the nurse-invited patients is similar to that observed in general app usage which typically falls to 39% after 30 days, 26% and 20% of users after 60 and 90 days, respectively.17 Figure 3 illustrates the attrition and the associated table provides details of attrition by age and gender.

{kind=link}
{kind=link}
{kind=link}
We used the motivation, ability and triggers of the Fogg behaviour model4 to explore why patients adhered to our app (or not) using data from the qualitative interviews, usage data and post-study questionnaire.
Adherence: motivation
Encouragement from GPs, asthma nurses or researchers motivated patients to keep the app on their smartphone/tablet and potentially use it when their symptoms were getting worse or when they needed help on managing their asthma. Perceived health benefits and practical help managing their asthma were the main reasons for continuing to use the app given by post-trial interviewees. The app helped them to understand their asthma, made them aware of their asthma’s triggers and how they were affected, enabled them to assess and improve control and (if possible) reduce medication.
I can keep a track on maybe how, in linking what’s going on in life versus what triggers your asthma…to educate people on their asthma I think yeah it is a good thing [Patient 5, 26–45 years, usage: 48 days]
Some patients valued the medication reminder features as a memory aid and encouragement to maintain exercise. One person highlighted how the free-text diary provided her with psychological support.
I would use the app more as a memory aid for all aspects of my asthma, when to take the medication [Patient 4, 65 years+, usage: 129 days]
it’s made me feel a little bit guilty so it’s then motivated me to work out the next day [Patient 10, 26–45 years, usage: 55 days].
I think by just putting it into the app and just saying I feel a bit down today it sort of raises my spirits. (laughs)… it’s like a support in a way because nobody ever comes into the house and says ‘how are feeling, [Name]’? [Patient participant A2, 46–65 years, usage: 68 days]
Several interviewees indicated that contributing to research was an important incentive; two suggested that financial initiatives might encourage adherence.
Adherence: abilities
Most patients were able to use the app prototype by themselves, although some (from across the age range) had initial questions (e.g. queries about the 10 monitoring questions, unsure how to enter and save responses, difficulty in visualising logged data on the healthcare graphs and managing the reminder alarm system).
Adherence: triggers
A pop-up push notification, with a ‘single-click’ return to the app, was pre-set at 18.00 every day. Some patients used the app immediately after the notification; some ignored it because they were busy or forgot, or had nothing they wanted to input into the app and some disabled the notification. Although reminders were mentioned as a useful feature, overall the use of the notifications did not seem to encourage patients to continue to use the app. Some patients who enabled the notifications never used the app, whereas some patients who disabled the notification used the app for more than 30 days.
A reminder comes on my phone and then if I’m working night shift and I’m sitting there then I have time that I’ll fill it out but if I’m off and I’m busy then I tend not to do it [Patient 5, 26–45 years, usage: 48 days].
DISCUSSION
Summary of findings
One hundred and eleven patients, aged ≥16 years old, with ‘active asthma’ adopted our app prototype for 3 months; 15 of these were interviewed. Numerically, the adoption from social media far exceeded recruitment via practices, although if considered as a proportion of people potentially reached by the invitation (400,000 Twitter and Facebook followers versus 300 people reviewed for their asthma), the practice recruitment rate was greater, albeit slower (2% of people who attended clinics). Adherence to the app fell over time, with greater attrition amongst patients recruited via social media than those invited personally by their practice nurse (83% reduction versus 63% at 30 days). Most patients prioritised recommendations from people they knew and trusted, considered that encouragement from their GP or asthma nurse would motivate them to download and continue to use an app to support their self-management, especially if it improved their asthma control. Reminders (e.g. to log control, take medications, undertake exercise) were described as useful triggers though response (or not) to notifications was influenced by motivation. Some patients needed assistance with downloading and starting to use the features of the app, though most found the process straightforward.
Strengths and limitations
Underpinned by a behaviour model,4 our study provides insight into patients’ adoption and usage of an asthma self-management app with respect to trigger events, patient’s motivations and abilities. However, there are some limitations.
Firstly, although we explored perceived motivation, observed ability and measured the response on downloads and usage of different triggers, the small numbers meant we were unable to quantify the level of impact associated with different recruitment techniques. In addition, some patients may have received more than one form of invitation. Streams A, B and C were defined by the format of the invitation that triggered the response but it is possible that a few patients may have been exposed to multiple motivators. We, therefore, avoided statistical analysis, using observational quantitative findings to add a complementary picture of the themes emerging from the qualitative analysis.18
Secondly, the findings are not generalisable to patients with ‘high risk’ asthma, children, the elderly and patients without a smartphone (though the latter is a reducing problem with increasing smartphone penetration rate globally19).
Thirdly, the triggers that we explored for adoption were limited to practice invitation letters, nurse invitations during consultations and social media, though these are feasible recruitment strategies that could be implemented in routine healthcare service and research.
Interpretation in relation to published literature
Our findings can be interpreted in the light of the Fogg behaviour model.4 Table 3 illustrates our findings mapped on the model.
Adoption
Successful adoption was dependent on ease of downloading and sufficient motivation (see Table 3). People could respond easily to the trigger of a tweet or post by clicking a link on the social media they were using at the time. In contrast, those invited by letter or personal invitation from their practice had to remember to find the download information next time they use a suitable device, and in addition, may have been less familiar with the process of downloading apps. Social media users were not motivated personally by their GPs or asthma nurses, so very few of the people who saw the ‘tweet’ or ‘Facebook message’ responded – though numerically the wide reach and instant impact of social media produced more and very prompt downloads than practice invitations. The combination of an easy download/registration process and sufficient motivation are targets for encouraging adoption.
Adherence
Adherence was dependent on motivation, typically derived from a sense that the healthcare professional and/or researcher were interested in the results. Patients from social media stopped using the app prototype more rapidly than those invited by their practice even though the triggers (notifications and reminders) were the same for the social media and two practice recruited streams. The ease/difficulty of using the app was similar for both streams as judged by questionnaire responses and perceptions expressed in interviews. However, patients receiving a personal invitation from their practice, and especially those involved in the qualitative research were motivated to continue using the app at least for the duration of the study (Hawthorne effect20). Motivation is the key target for maintaining adherence to using an app.
Implications for healthcare services providers
Our findings suggest that using a dual promotion strategy: utilising social media for its reach and ease of response, but also promoting personal invitations from trusted healthcare professionals may be an effective dual approach to increasing patients’ adoption of an asthma app. Social media can trigger patients to respond to invitations to use the app but they quickly stop using the app without the motivation provided by an interested professional.
Our focus was asthma, but studies in other disease areas echo these findings. In the context of diabetes, patients stopped checking their blood glucose if professionals did not show interested in their logs.21 Tele-monitoring of diabetes encouraged home monitoring as a result of presumed professional surveillance22 and improved clinical outcomes were demonstrated in trials of telehealth in diabetes and heart failure which included monitoring and feedback.23 Tele-monitoring can thus support the motivation provided by on-going interest from professionals, though from a practical perspective this requires the professional to be able to seamlessly access their patients’ information during a consultation.24
Easy and immediate access to downloading is a key to trigger adoption. Patients invited by their asthma nurse could not just click a link, they had to make time to use their mobile phone or tablet, seek out the website from paper instructions. Healthcare providers should consider facilitating the download process, for example, by providing a QR code on invitation letters or following up an asthma review with an e-mail, including a link to allow direct downloading. A few people needed help with downloading and using the app, and effective implementation will require resources for providing (easily accessible) technical support.
CONCLUSION
Using social media may provide a ‘quick win’ in terms of initial downloads, but adherence to app dropped rapidly over time. Practice engagement may be important to provide motivation for sustained use of an app. Practical implementation strategies include enabling easy access to download links, simple intuitive software and ensuring that professionals perceive advantages to using the system as their buy-in is crucial to maintaining motivation and on-going engagement with the ‘app’.
Acknowledgments
We are grateful to patient and professional participants to take part in this study; Ellen Drost from the Scottish Primary Care Research Network who helped with practice recruitment; Asthma UK and the Asthma UK Centre for Applied Research Centre (AUKCAR) for use of their social media for patient recruitment. Melissa Goodbourn (AUKCAR) facilitated patient and public involvement; and the Primary Care Respiratory Society UK enabled professional user engagement. We thank Richard Parker for statistical advice and uMotif Limited for providing the app’s configuration services.
References
Footnotes
Funding CyH is funded by a PhD studentship from the Chief Scientist Office (Scotland) [AUKCAR/14/01]. This work is carried out with the support of the Asthma UK Centre for Applied Research [AUK-AC-2012-01]. The views expressed in this publication are those of the authors and not necessarily those of the Chief Scientist Office (Scotland).
Conflict of Interests None.
Author Contributors Chi Yan Hui, Brian McKinstry, Robert Walton and Hilary Pinnock designed the study. Chi Yan Hui undertook the data extraction and synthesised the data with Hilary Pinnock; Hilary Pinnock is the study guarantor. Chi Yan Hui with Hilary Pinnock wrote the initial draft of the manuscript. All authors contributed to the writing of the paper and reviewed the final manuscript.