Article Text

Abstract
National Health Service (NHS) Scotland is about to embark on the implementation of hospital electronic prescribing and medicines administration systems. There are a number of risks associated with such ventures, and thus drawing on existing experiences from other settings is crucial in informing deployment.
Drawing on our previous and ongoing work in English hospitals as well as the international literature, we reflect on key lessons that NHS Scotland may wish to consider in going forward. These deliberations include recommendations surrounding the key aspects of deployment strategy: 1) the way central coordination should be conceptualised, 2) how flexibility in strategy can be ensured, 3) paying attention to optimising systems from the outset, 4) how expertise should be developed and centrally shared, and 5) ways in which learning from experience can be maximised.
Our five recommendations will, we hope, provide a starting point for the strategic deliberations of policy makers. Throughout this journey, it is important to view the deployment of hospital electronic prescribing and medicines administration systems as part of a wider strategic goal of creating integrated digital infrastructures across Scotland.
- Hospital electronic prescribing and medicines administration
- implementation
- strategy
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Electronic health (or eHealth) functionalities associated with prescribing and medicines administration have been shown to improve the safety and quality of care and also to contribute to increasing healthcare efficiency.1 These systems therefore play an essential part in international efforts to modernise health systems.2,3 For example, National Health Service (NHS) England has established eHealth systems as a strategic priority. These efforts were underpinned by an Integrated Digital Care Fund of £240m in hospital settings and, more recently, the implementation of the recommendations made in the Wachter Review – in particular, the funding of NHS Global Centres of Digital Excellence.4–7
The widespread deployment of hospital electronic prescribing and medicines administration (HEPMA) systems in Scotland, with JAC and Ascribe as the preferred options, is imminent and it is therefore now timely to reflect on experiences from other health systems to inform the strategy that Scotland should adopt.8 Drawing on previous and ongoing work, we distil five key lessons that policymakers should consider going forward.9,10
Overall, the implementation of HEPMA is best viewed as part of a journey towards digitising health systems. Implementation-related activities in this process can be seen as being part of the system lifecycle including conceptualisation, planning, implementation and adoption, and optimisation activities.11 Our group has developed an implementation toolkit to this effect, intended to help guide healthcare organisations in their efforts to implement HEPMA systems (see http://www.eprescribingtoolkit.com/).11
Examining activities through the lifecycle perspective indicates that once systems are chosen, the system lifecycle is already relatively advanced (i.e. at the contracting stage). As NHS Scotland is at this advanced stage in the lifecycle, we here focus on the pre-implementation, implementation and adoption, and optimisation stages.
Central coordination
Some central coordination is essential to streamline efforts to move towards optimisation (preferably reducing the time to deliver the benefits that optimisation will generate) and set standards that will eventually allow sharing of data across Scottish care settings.12 Experiences of similar ventures have shown that if central support and impetus is lacking, adoption of complex technological systems in healthcare can be slow.13 Given the central approach, there is, however, a risk that systems will be viewed as imposed by local hospitals and users,14,15 which may hamper their intended use and slow down implementation timeliness.16 Setting up a range of structures that allow continuous strategic input from implementer sites and academic evaluators may help to address this (see Figure 1 for a proposed model). NHS Scotland has the advantage that relevant stakeholders can come together in person to exchange experiences (in contrast to England where travel distances and larger stakeholder numbers complicate the feasibility of face-to-face meetings). Existing structures now need to be utilised to strengthen national engagement activities and to involve end users from all of the impacted professions ensuring that systems bring the intended benefits to individual users earlier on in the process than might otherwise be achieved.17 This may be realised through establishing a single central source of information to underpin face-to-face or other engagement activities and information needs of different stakeholders.11 Here, it is important to convey from the start that system implementation and use is not primarily pharmacy led (as is often the case), but should draw on the range of professions – in particular, doctors (who prescribe electronically) and nurses (who administer and record this on the system) – that are affected by the wider transformation of healthcare delivery associated with new systems.10 This needs to involve active participation of other professions in system choice or customisation, work process mapping, benefits realisation and system optimisation. As such complex electronic systems can result in significant changes to the way individual professions operate, benefits may take some time to realise and a critical mass of users from various backgrounds may be needed to achieve desired outcomes.13

There are also significant opportunities surrounding economies of scale afforded by the national procurement model being pursued in Scotland and these should be harnessed. Central coordination of implementation efforts, including training strategies, should help to draw on existing experiences, to feedback lessons learned across implementations, and to share expertise and pool resources.18 An important aspect here is the setup of nationally shared risk/hazard registers, where known technical limitations and potential mitigation strategies are shared between hospitals. This should, if possible, be agreed with HEPMA vendors in advance.
Flexibility in strategy based on periodic review
The deployment strategy needs to be flexible and responsive to local needs wherever possible to help mitigate potentially adverse consequences resulting from the national procurement model.19 In order to achieve this, ongoing evaluation of implementation progress and potential risks is vital.20 This should also include formative feedback to implementer sites thereby helping to build local evaluation expertise and to guide next steps.
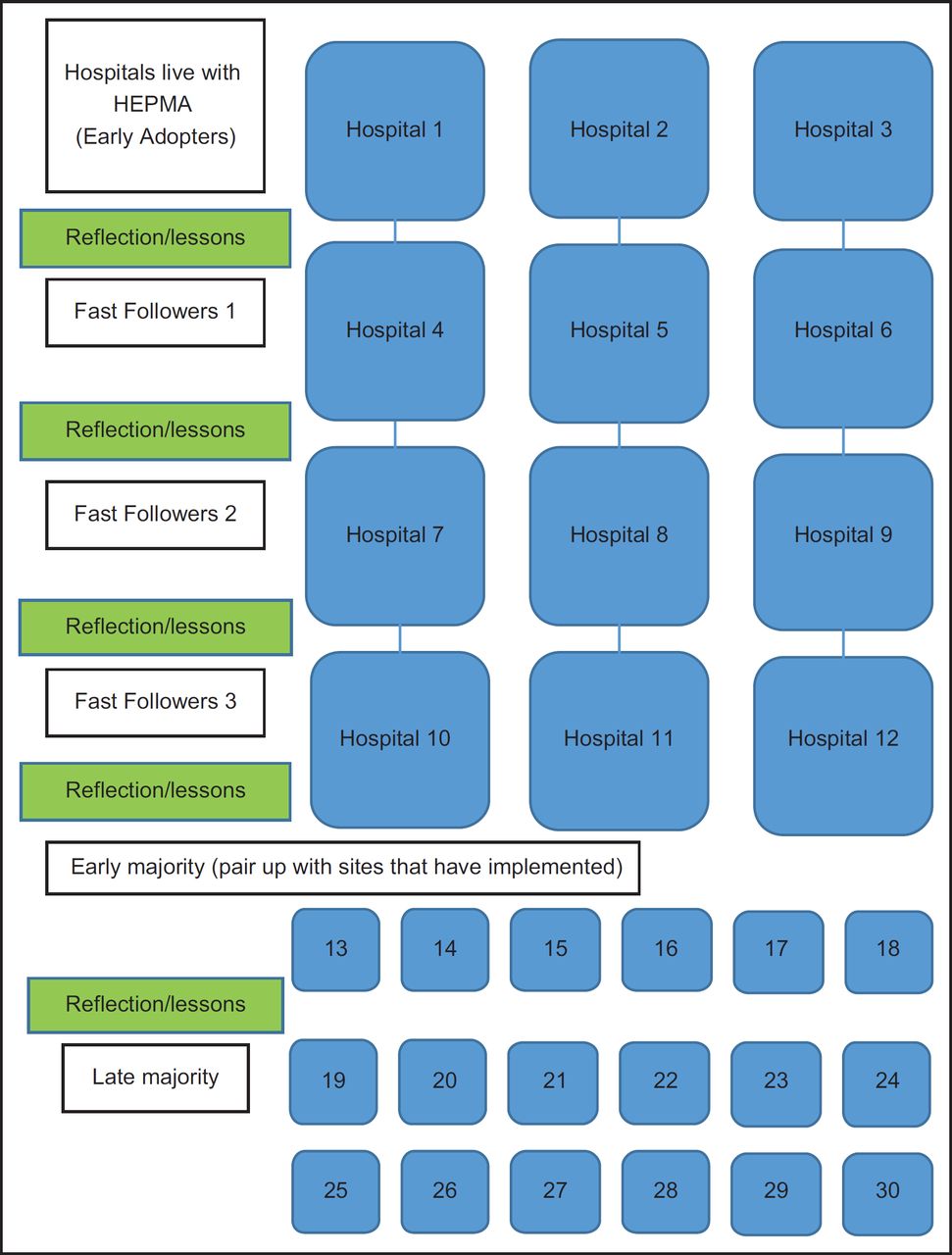
In terms of deployment strategy (see Figure 2 for a proposed model, further discussed below), there should be a formal review after each cohort of hospitals goes live, feeding back lessons learned into future planning and making adjustments where necessary. We suggest that a multidisciplinary National Advisory Board is established, which will be responsible for strategic oversight of implementation efforts and progress and also liaise with local implementation teams and suppliers. This will also help to oversee individual sites’ readiness and thus manage the scheduling of go-lives.

{kind=link}
{kind=link}
Focus on system optimisation from the start
In line with the system lifecycle perspective, system optimisation needs to be seen as the end goal, as deriving value from HEPMA is very dependent on achieving this.21 It is however, more often than not an afterthought in many implementation efforts. The implementation of HEPMA systems in Scotland represents a real opportunity to share optimisation experience, as some hospitals in the UK/Scotland have refined systems over a number of years to realise significant benefits.10 If ‘fast followers’ effectively utilise the experiences from ‘early adopters’, this can help to reduce the timeline to realise benefits.
It is also important to view HEPMA as part of the growing health information infrastructure in Scotland, where an increasing number of users draw on a range of sources of information and collect data from these that are then (in due course) centrally collated and analysed. Interfacing and data analytics activity should be central to these optimisation efforts, as the HEPMA system that is likely to be deployed in Scotland is an interfacing (rather than an enterprise) solution with limited inbuilt data analytics capability.22 A national data strategy on how this may be achieved should guide ongoing analytics efforts and HEPMA implementation should be viewed as part of the journey towards realising this aim.
Developing, sharing and retaining expertise
NHS Scotland has limited implementation and optimisation expertise, which may hamper efforts to successfully deploy and derive benefits from HEPMA.23 A central problem is that all too often external project managers are seconded to oversee implementations and then leave with the accumulated knowledge. Internal capacity development using local staff and increasing their skill set ensuring that staff is retained at local level should therefore be a priority for the Scottish Government. Developing and retaining expertise is important for implementing hospitals in order to help maintain and continually refine systems beyond the initial implementation period, whilst sharing expertise nationally can help to maximise existing resources. Creating new career pathways, structures and incentives are essential activities that thus need to be carried out in parallel to system implementation. This has also been recognised in the recent Wachter Review, which includes strategic recommendations for the digitisation of NHS England.7 Efforts should ideally be inter-disciplinary reflecting the broad range of skills and expertise needed to exploit HEPMA for patient, professional and system benefits. Periodic sharing of experiences should also be promoted across hospitals, and to this end, the establishment of an implementation peer support and networking group could be considered.
Learning from experience
There is already significant expertise available within the UK, including hospital sites that have implemented and optimised the same system that is likely to be procured in Scotland. Implementer sites have also over time developed important insights surrounding the limitations of commercial systems and devised strategies to manage potential safety risks associated with altered user workflows and technological interface design.22,24–26
There are further a range of academic evaluators that have insights into local, national, and international experiences. Drawing on this expertise will be vital in facilitating the implementation and ongoing optimisation of systems. The proposed structures in Figure 1 may help to conceptualise how it can be effectively harnessed.
In terms of deployment strategy, we propose that hospitals pair up with those that already have implementation experience in relation to planning, direct implementation and ongoing optimisation. Figure 2 outlines how this may be conceptualised, incorporating periodic review and reflection on experiences after each new cohort of hospitals goes live. A phased deployment strategy should be considered at the outset, thereby allowing an opportunity for learning from early efforts, followed by accelerated implementation across the remaining hospitals.
Conclusions
We have made a number of recommendations that will, we hope, help Scottish policymakers ensure successful deployment of HEPMA systems, resulting in accelerated realisation of benefits for system users and implementing organisations. We further argue that, although lessons from implementing eHealth systems from other countries need to be learnt, simplistic mirroring of the attempts of other countries should be avoided.27 Rather, local context needs to be taken into account and plans should be adapted accordingly.
More generally, it is important to pursue the strategic goal of creating integrated digital infrastructures across Scotland.28 The implementation of HEPMA presents an important stepping stone and a real opportunity in this respect.
Acknowledgments
We are very grateful to all participants who kindly gave their time and to the extended project and program teams of work we have drawn on. We would also like to thank two anonymous peer reviewers for their helpful feedback on an earlier version of this manuscript.
References
Footnotes
Contributors and sources AS and ASl conceived this work. AS is currently leading a National Institute for Health Research (NIHR) funded national evaluation of electronic prescribing and medicines administration systems. KC is employed as a researcher on this grant and led on the write-up and drafting the initial version of the paper, with AS and ASl commenting on various drafts.
Funding This work has drawn on data funded by the NHS Connecting for Health Evaluation Programme under Grant NHS CFHEP 001, under Grant NHS CFHEP 005, under Grant NHS CFHEP 009, and under Grant NHS CFHEP 010, the National Institute for Health Research under its Programme Grants for Applied Research scheme under Grant RP-PG-1209-10099 and The Commonwealth Fund. KC is supported by a Chief Scientist Office (CSO) of the Scottish Government Post-doctoral Fellowship and a grant by the Edinburgh and Lothians Health Foundation and AS is supported by the Farr Institute. The views expressed are those of the author(s) and not necessarily those of the NHS, the CSO, the NIHR or the Department of Health.
Competing interest declaration The authors declare that they have no competing interests.