Article Text

Abstract
Objective Clinical decision support systems (CDSSs) can reduce medical errors increasing drug prescription appropriateness. Deepening knowledge of existing CDSSs could increase their use by healthcare professionals in different settings (ie, hospitals, pharmacies, health research centres) of clinical practice. This review aims to identify the characteristics common to effective studies conducted with CDSSs.
Materials and methods The article sources were Scopus, PubMed, Ovid MEDLINE and Web of Science, queried between January 2017 and January 2022. Inclusion criteria were prospective and retrospective studies that reported original research on CDSSs for clinical practice support; studies should describe a measurable comparison of the intervention or observation conducted with and without the CDSS; article language Italian or English. Reviews and studies with CDSSs used exclusively by patients were excluded. A Microsoft Excel spreadsheet was prepared to extract and summarise data from the included articles.
Results The search resulted in the identification of 2424 articles. After title and abstract screening, 136 studies remained, 42 of which were included for final evaluation. Most of the studies included rule-based CDSSs that are integrated into existing databases with the main purpose of managing disease-related problems. The majority of the selected studies (25 studies; 59.5%) were successful in supporting clinical practice, with most being pre–post intervention studies and involving the presence of a pharmacist.
Discussion and conclusion A number of characteristics have been identified that may help the design of studies feasible to demonstrate the effectiveness of CDSSs. Further studies are needed to encourage CDSS use.
- decision support systems, clinical
- electronic health records
- health information exchange
- health information systems
- medical informatics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- decision support systems, clinical
- electronic health records
- health information exchange
- health information systems
- medical informatics
Background
Healthcare systems are affected by numerous factors that can reduce quality of care and increase the costs of the services offered. Medication errors are a relevant problem that must be faced with an eye to both patient safety and healthcare-system sustainability. The total costs associated with medication errors in the USA have been estimated at US$42 billion/year and a study has revealed that medication errors during hospital stays may affect up to 6.2% of prescribed medications in the USA and up to 1.5% in the UK.1 2
A prescription error may be caused by handwriting problems and poor treatment decisions, potentially leading to the inappropriate use of drugs and harm for patients.3 Excessive and inappropriate prescriptions can result in severe consequences, such as adverse drug reactions, increased risk of toxicity, prolonged hospital stays, increased antimicrobial resistance, decreased faith in the medical profession and wastage of public funding.4 This problem is particularly relevant for patients suffering from multiple chronic diseases and requiring the concomitant prescription of different drug classes, a condition that increases the likelihood of medication errors and of potentially inappropriate medications (PIMs) prescription.
Digital technologies5 including Clinical Decision Support Systems (CDSSs) represent possible strategies for the prevention and reduction of prescription errors. CDSSs consist of digital tools designed to provide interactive computer-based information to assist healthcare professionals in the clinical decision-making process. They were first developed 50 years ago with the aim of promoting optimal problemsolving, decision-making and facilitating the actions of decision-makers as well as making patient data easier to assess. In addition to the support provided to healthcare professionals, CDSSs can produce additional knowledge to guide clinicians by generating new evidence in real time, thus promoting the practice of evidence-based medicine.6
Traditional CDSSs consist of a clinical knowledge base, which is the inference engine that combines information from the knowledge base with input data, and of the user interface. In general, it incorporates concepts that are derived from scientific literature and expert knowledge and should be constantly updated to keep up with new evidence generated in clinical practice.7 Traditional CDSSs can offer clinicians patient-specific advice based on globally recognised recommendations, as well as increase physician adherence to medical guidelines.
Non-knowledge-based CDSSs are based on artificial intelligence (AI-CDSSs) and have been recently introduced in clinical practice.8 9 AI-CDSSs still require a data source but leverage AI and machine learning to generate recommendations tailored to patient characteristics. Modern CDSSs are primarily knowledge based since AI-CDSSs require computer-intensive and time-consuming processes and the analysis of a significant amount of data to provide accurate decisions.
The use of these systems has been widely discussed and promoted by healthcare services. They can be used for multiple purposes, including diagnostics, prescription and alarm systems. However, the introduction of CDSSs into all areas of clinical practice still faces several obstacles, including the low ease of system use, negative end-user attitudes towards the system, inaccurate and poor-quality data or documentation, fragmented workflows, financial challenges and an excess of insignificant alerts (alert fatigue).10 11 New studies should be designed based on the evaluation of previous interventions with CDSSs, regardless of the healthcare setting selected, in order to identify barriers to be overcome for their implementation and key characteristics which proved to generate a positive impact on patient health and on clinicians performances. Although previous studies12–15 have already estimated the ability of CDSSs to improve healthcare, this kind of evidence has not yet been achieved.
Therefore, the aim of this scoping review is to identify the characteristics of studies in which a CDSS has been effectively implemented in any area of clinical practice producing positive outcomes. Secondary objective is to propose a checklist to be used by healthcare professionals for the implementation of future interventions aimed at demonstrating the effectiveness of CDSSs in improving the quality of care in different settings (ie, hospitals, community pharmacies, general practitioner’s (GP) clinics).
Material and methods
Search strategy
This scoping review was performed according to the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR).16 The PRISMA-ScR checklist is shown in online supplemental table S1.
Supplemental material
Scopus, PubMed, Ovid MEDLINE and Web of Science were searched in order to identify relevant articles. The following filters were applied: article language Italian or English, publication date between January 2017 and January 2022, excluding reviews. Given the recent introduction in clinical practice of CDSSs to improve prescriptive appropriateness, a 5-year period was considered sufficient to identify eligible studies. The final search was conducted on 10 January 2022. The author LGA performed an initial search in Scopus with a combination of the terms “Clinical Decision Support System” and “Inappropriate Prescriptions” to identify relevant keywords. The keywords extracted from the most relevant titles and abstracts were discussed by the authors to select those to be used for the final search. Subsequently, the identified keywords were associated with the Medical Subject Heading terms and approved by all the authors. The final search was conducted by LGA with the query shown in figure 1 and was verified by CC.
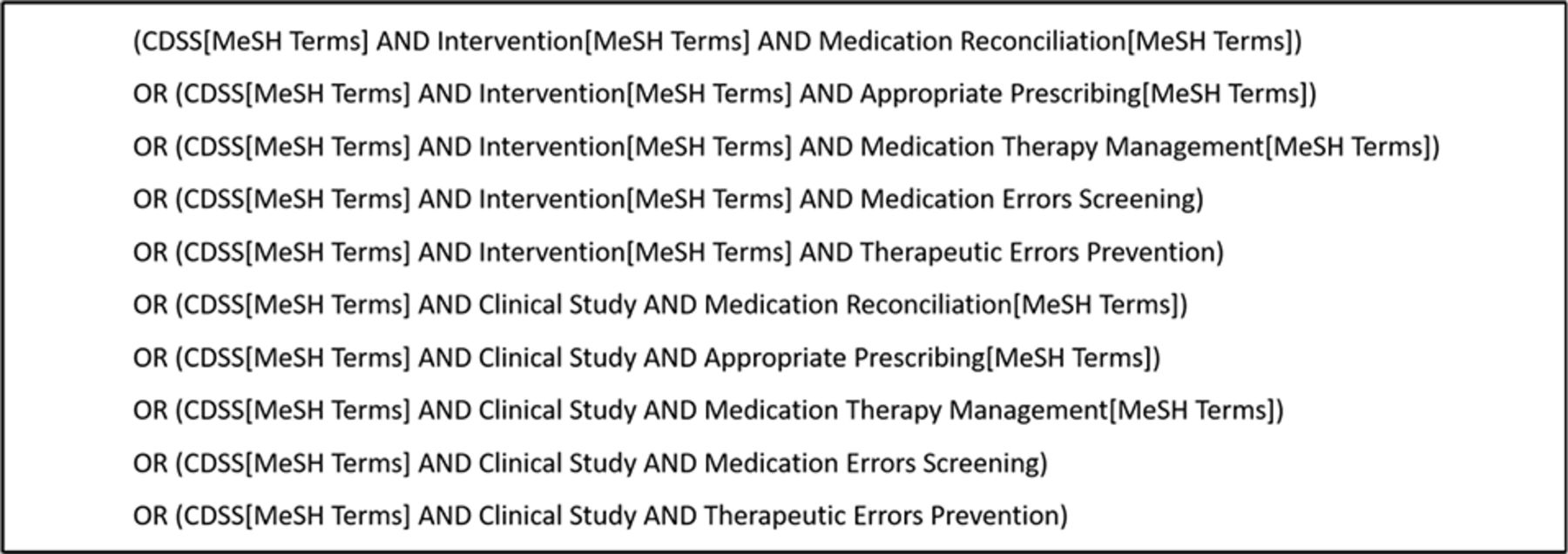
Final search query.
Eligibility criteria
The question that drove this review was ‘Can we learn from previous studies which characteristics and design should have interventions that effectively leverage CDSSs to improve quality of care and prescriptive appropriateness?’. To answer this question, prospective and retrospective studies that reported original research on CDSSs for clinical practice support were identified. Studies including a measurable comparison of the intervention or observation conducted with and without the CDSS were included. Randomised, observational, diagnostic and mixed-method studies were included, while qualitative (survey and semi-structured interview) studies and development reports were excluded. The review does not include studies or documents that describe computerised systems that do not provide decision support, such as electronic health record (EHRs), apps or web-based platforms for therapy self-management. The list of eligibility criteria is given in table 1.
Inclusion and exclusion criteria for title and abstract screening
Study selection
The search results were extracted by LGA into a table in Microsoft Excel to remove duplicates. Two authors (LGA and CC) then independently screened study titles and abstracts for inclusion and exclusion criteria. In case of disagreement between LGA and CC, the other authors were asked whether or not to include the study in the next step. Where available, the full texts of potentially relevant articles were screened by LGA and subsequently confirmed by CC. Unavailable full-text articles were defined as publications that could not be accessed either electronically or via a library.
Publications were included if they described a CDSS that was implemented in a real clinical setting and used by healthcare providers to aid decision-making. All systems that analysed patient-specific information to generate case-specific guidance messages through rule-based and algorithm-based software were considered valid, regardless of the targeted assistance (eg, diagnostics tests, chronic disease management, therapy recommendations, drug prescribing, medication reconciliation, medication error detection). Moreover, studies had to report at least one outcome that was capable of measuring the effect of the CDSS on the quality of care provided to patients.
Data extraction
A Microsoft Excel spreadsheet was prepared to extract data from the included articles (online supplemental table S2). All of the authors agreed on what data items to extract to guide the process of result elaboration. Data recorded included: medical area of interest; characteristics of the system and its focus; study setting and design; end user; outcomes measured; study period; sample characteristics; summary of the results.
Results
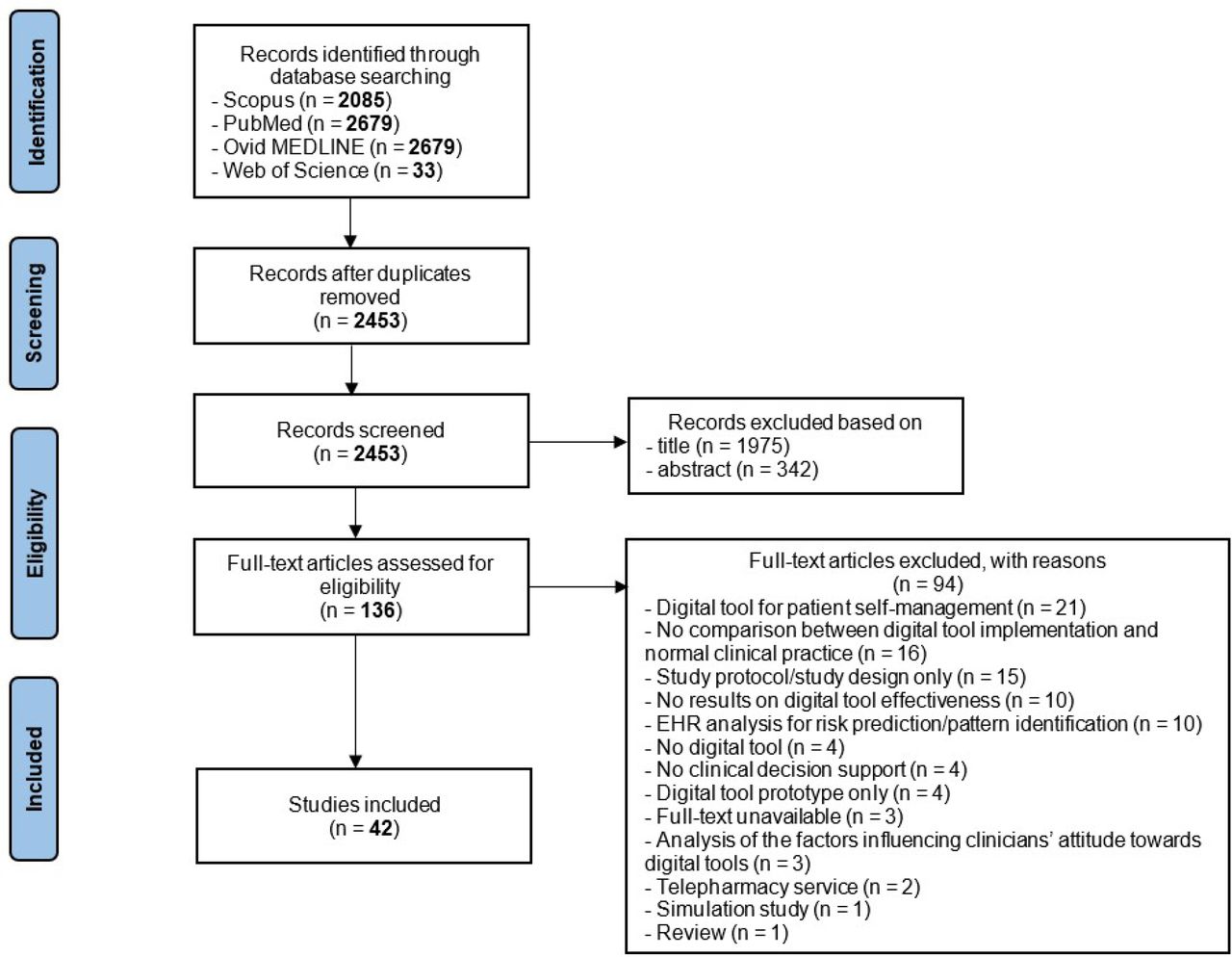
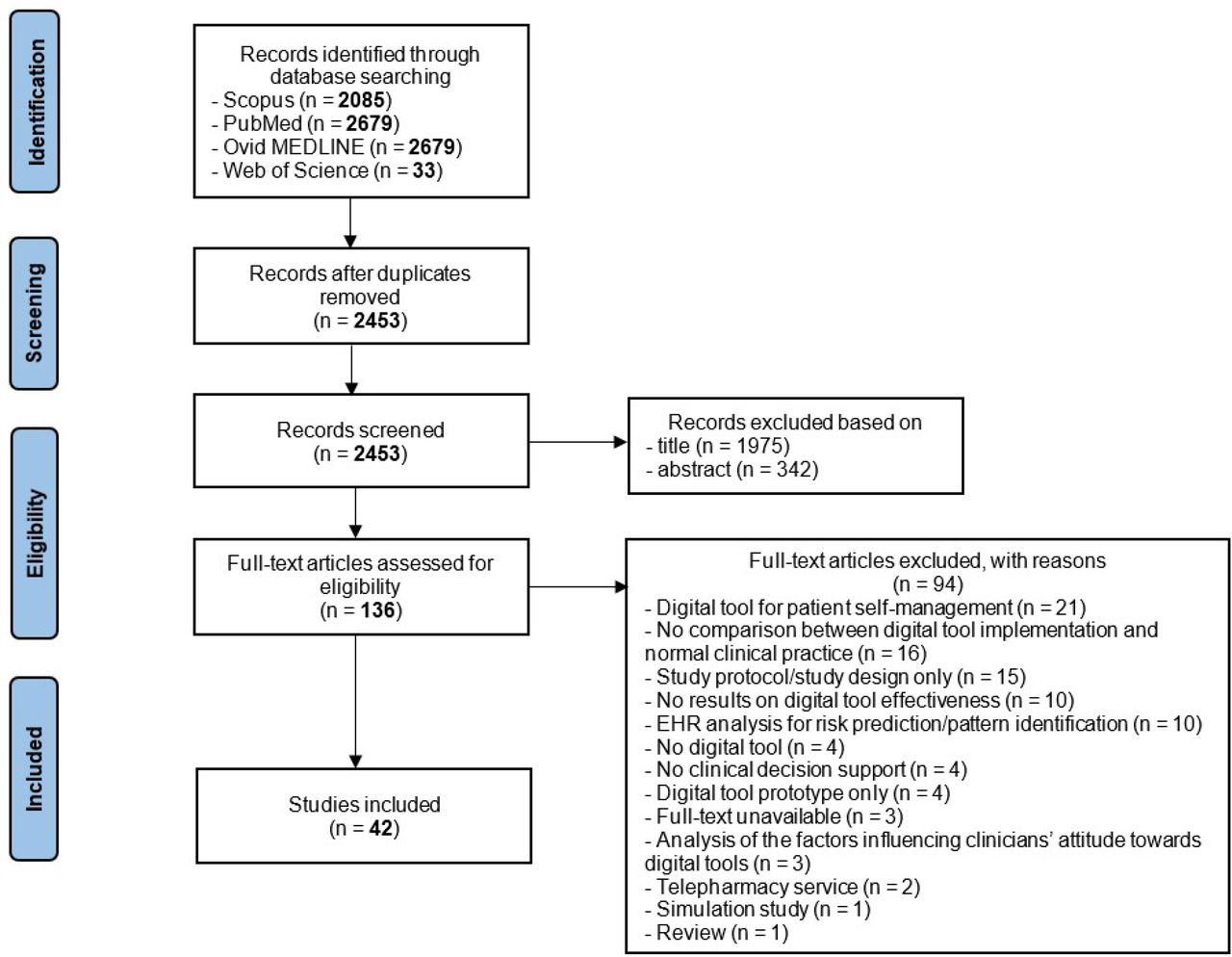
The search identified 7476 articles eligible for screening. After removing duplicates, 2453 articles were available for title and abstract screening. During title screening, 1975 articles were excluded either because they were of the wrong publication types or lacked a digital tool to support clinical decision; 478 articles were considered to be relevant for abstract screening. This number was further reduced for the reasons given in table 1. After assessing the eligibility of the remaining 136 articles, 42 articles were included in the review. The screening and eligibility-checking process is described in figure 2.
{kind=link}
{kind=link}
PRISMA flowchart for article selection and review. EHR, electronic health record; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Only seven studies (16.7%) were implemented in more than one setting; 19 (45.2%) were developed in the USA, with the remaining CDSSs being implemented in Canada (4; 9.5%), Australia (3; 7.1%), the Netherlands (3; 7.1%), the United Kingdom (3; 7.1%), China (2; 4.8%), Germany (1; 2.4%), Italy (1; 2.4%), Ireland (1; 2.4%), Norway (1; 2.4%), Austria (1; 2.4%), Switzerland (1; 2.6%), Pakistan (1; 2.4%) and South Korea (1; 2.4%). Table 2 summarises the main characteristics of the studies included in the analysis.
Characteristics of the studies included in the analysis
Overview of results
The main setting of the studies analysed was hospital wards, followed by GP clinics and the emergency department. The selected studies focused on the management of various conditions, the most common being the treatment of hospitalised patients and the treatment of children and adolescents. Of the included studies, 40.5% (17 studies) were randomised controlled trials (RCTs), 31.0% (13) before-and-after studies, 23.8% (10) retrospective observational studies and 4.8% (2) non-controlled clinical trials and quasi-experimental design studies.
There were no substantial differences between the number of CDSSs implemented for the management of drug-related problems (22 studies; 52.4%) and that of CDSSs employed to manage problems related to the disease (20; 47.6%). Most of the systems used in the selected studies were knowledge-based CDSSs (35 studies; 83.3%), containing either rules based on globally recognised criteria, such as the Beers criteria and the Screening Tool of Older Persons’ Prescriptions (STOPP)17 18 or rules based on international guidelines. Several platforms for delivering clinical decision support were used, but more than half (22 studies; 52.4%) were CDSSs integrated with existing databases, such as EHRs and/or other hospital electronic devices.
Patient complexity was classified into three levels based on patients’ baseline characteristics.
Study description and reported outcomes
The major primary outcome defined by the analysed studies is summarised in table 3. The outcomes are classified according to the level on which they had the greatest impact: patient level, clinician level and healthcare setting level.
Major primary outcome measures of the analysed studies
Twenty-five out of 42 studies achieved their primary outcome with significant differences between the control group and the intervention group, demonstrating the usefulness of CDSSs in improving clinical practice. The online supplemental materials include the characteristics of each study analysed (S2) and a figure representing the process for conducting effective studies (S3).
Successful studies, that is, those in which the CDSSs were proven to be effective in supporting clinical practice, showed some substantial differences from studies where the CDSSs either failed to support clinical practice (12; 28.6%) or produced uncertain results (5; 11.9%). These latter included studies in which, despite the potential positive effects of CDSSs, the outcomes were not achieved due to study limitations that were highlighted by the authors themselves (ie, short study period, non-homogeneous case–control samples, poorly defined outcomes, non-significant differences between groups).
Discussion
To the best of our knowledge, this is the first scoping review which attempts to identify the characteristics of studies in which different types of CDSSs were used to effectively support clinical decision in different settings. Previous scoping reviews have focused on CDSSs for medication review, rare-disease diagnosis, non-knowledge-based clinical decision support tools and on CDSSs to be used in nursing homes.6 19–21
In most of the studies analysed, the implementation of CDSSs in clinical practice improved disease management, increasing the number of PIMs detected, reducing the number of patients who experienced adverse outcomes and enhancing the prescription of appropriate treatments. This aspect is particularly important for certain categories of patients, such as complex patients that suffer from multiple chronic diseases, who often need their (poly)therapy to be reconciled due to the high number of medications that are coprescribed by different specialists. For example, McDonald et al22 have demonstrated that the inclusion of an electronic decision support tool for deprescribing (MedSafer) in primary care increased the proportion of PIMs that were deprescribed at hospital discharge. MedSafer is able to identify inappropriate medications according to the Beers criteria, the STOPP and the Choosing Wisely list17 18 23 as well as providing tapering instructions for medications such as benzodiazepines. Another study by Fried et al24 has shown that integrating the Tool to Reduce Inappropriate Medication (TRIM) into EHRs was associated with improvements in shared decision-making and reduced medication reconciliation errors. TRIM evaluates prescription appropriateness based on the potential overtreatment of diabetes mellitus and hypertension in the elderly, the Beers and the STOPP criteria, inappropriate renal dosing and patient reports of adverse medication effects.
The main finding of this review is the identification of the characteristics that are most likely associated with positive and negative outcomes, identified by comparing successful and unsuccessful studies. Hospital wards were the most common setting in all studies analysed, although there were substantial differences in the types of patients enrolled: most successful studies first involved the enrolment of hospitalised patients, of children and adolescents and of patients with infectious diseases, while most of the unsuccessful or inconclusive studies were carried out in geriatric wards. In most successful and unsuccessful studies, CDSSs were intended to be used by multidisciplinary teams operating within a single hospital or clinical centre, underlining the importance of the participation of different healthcare professionals in improving the management of complex patients. The presence of a multidisciplinary team in the clinical decision process facilitated the sharing of information between healthcare professionals; in addition, belonging to a single hospital or clinical centre may have made relationships easier. On the other hand, a large proportion of interventions including multicentre settings proved to be unsuccessful, suggesting that geographical distance may not have favoured multidisciplinary collaboration. Two important differences were found regarding the aim and study design of the studies analysed. First, CDSSs used in successful studies mostly had the aim of managing disease-related problems, whereas the use of CDSSs to support deprescription and/or the appropriate use of drugs was more frequent in unsuccessful and inconclusive studies. Second, most of RCTs produced either unsuccessful or inconclusive studies. This supports the conclusion that case–control studies are likely to fail to demonstrate the efficacy of CDSSs, as it is difficult to enrol comparable samples in terms of patient complexity.
As expected, the use of rule-based CDSSs that were integrated into existing software prevailed with similar proportions in all studies, since these are the simplest and fastest systems to be develop and use.
Baseline patient complexity was a further characteristic that was assessed qualitatively. Patients enrolled in successful studies generally appeared to be more complex at baseline as they had more coprescribed drugs, required enteral nutrition or the prescription of drugs with high risk of interactions or had impaired renal function and infectious diseases. This highlights that the use of CDSSs may especially support the management of complex patients at risk of adverse outcomes. Moreover, optimising the treatment of more complex patients offers greater benefits in terms of both economy and patient well-being, thus improving the quality of care.25
The participation of a pharmacist in interventions was also evaluated. Most successful studies included the pharmacist as part of the multidisciplinary team or as the principal investigator, while most of the unsuccessful and uncertain studies did not involve this professional figure; therefore, it is possible to hypothesise that the participation of a pharmacist in interventions could favour more positive outcomes. In support of this hypothesis, numerous studies demonstrated the role of pharmacists in reducing medication errors thanks to their special expertise and in providing education to other healthcare professionals.26 27
Finally, education of healthcare professionals and patient engagement were considered. Most successful studies (56.0%) included a preintervention period of education and training for healthcare professionals involved in the use of the CDSS, while only 35.3% of the unsuccessful studies included it; this aspect could, therefore, favour the usability of CDSSs. A general lack of activities to improve patient engagement was observed in all the selected studies: the absence of a summary report for the patient and of follow-up after the intervention in most studies represent a limit that should be overcome in the future by including the level of patient involvement as an outcome.
To evaluate the use of CDSSs at the national level, an assessment of the studies implemented in Italy was made. Despite Italy has a large proportion of elderly suffering from multimorbidity,28 29 only a few tools have been made available to support clinical decision compared with other countries. Only one Italian study conducted by Moja et al30 proved useful in supporting clinical practice, while three publications were excluded in the last selection phase for the following reasons: in the study conducted by Traina et al,31 the CDSS NavFarma was effectively used to reconcile the therapy of a group of elderly patients without being compared with a control group; in the second excluded study, Cattaneo et al32 used the CDSS INTERcheck to assess the risk of drug–drug interactions and PIMs in patients with COVID-19 at hospital discharge; the last excluded study33 described the design of a platform (Pneulytics) for the remote monitoring and management of patients with chronic obstructive pulmonary disease.
Based on these findings, the most feasible study design aimed at successfully improving the quality of care with the support of CDSSs gaining significant evidence of outcomes consists in a pre–post intervention study involving hospitalised patients with one or more chronic diseases and a complex situation at baseline, polymedicated and most at risk of adverse outcomes. Considering the length of studies with positive outcomes, at least a 1-year study period including both intervention and preintervention periods should allow differences to be observed in terms of prescriptive appropriateness, frequency and severity of symptoms and, more generally, of disease management. Therefore, enrolled patients should preferably have a life expectancy longer than 1 year to allow for adequate periods of observation before and after CDSS implementation. In order to enable comparison of different studies, authors should identify measurable and quantifiable outcomes at each stage of the study. The ideal CDSS should be easy to use, make information readily available and be integrated into the computerised systems of the healthcare facility where the study is performed, so as to reduce analysis time and the possibility of errors during data transfer. Moreover, studies should include a time for sharing the specific expertise of the different healthcare professionals involved in patient management, including pharmacists, in order to achieve the best possible outcome; active patient engagement in the management of their condition also appears to be associated with better outcomes.
Data on AI-CDSSs are still too limited to make a case for their superiority—or inferiority—over traditional CDSSs.
Strengths and limitations
The main strength of this review is the number of databases queried, along with the inclusion of all types of studies regardless of their focus. This revealed a large number of studies eligible for analysis to identify as many characteristics associated with positive outcome as possible.
The main limitations are the lack of unambiguous taxonomy to describe digital tools that support clinical decision and of recognised recommendations for conducting such studies. For example, some of the studies analysed lacked a description of the data that were entered into the system or did not indicate the end user. The choice to include studies that lacked complete information on the CDSS was made in order to select the largest number of CDSSs that have been used in a real-world healthcare setting.
On one hand, the heterogeneity of the studies has made it difficult for us to compare the different studies and devices (hence, the scoping review), while, on the other, it granted us a global view of the use of CDSSs worldwide.
Another limitation can be found in the absence of a focus on a specific patient category, which made it difficult to assess consistency with previous reviews.
Conclusions
To sum up, 25 (59.5%) of the selected studies proved effective in supporting clinical practice and improving treatment outcomes in different healthcare scenarios. However, the evidence reported does not allow robust conclusions on the effect of CDSSs in real clinical practice to be drawn, both due to the high variability of the interventions implemented and the limited number of CDSSs found.
From the results of this analysis, an initial version of a checklist was created that could be used to refine the design of studies aimed at evaluating the use of CDSSs:
Prefer studies with a pre–post intervention scheme.
Enrol population with complex morbidity and medication regimen at baseline but adequate life expectancy; one hospital setting (one or more wards) should be preferred for subject enrolment.
Plan interprofessional collaboration and pharmacist involvement.
Integrate a user-friendly CDSS with the healthcare facility’s computerised systems with information sharing capability among healthcare professionals.
Take into consideration active patient engagement and education of the healthcare professionals involved (contribution still uncertain).
Further research
There is a considerable need for studies that may demonstrate the usefulness of CDSSs in reducing medical errors and improving the quality of care. A possible solution is to promote the use of this checklist to plan studies conducted with CDSSs that may prove effective. Moreover, it would be desirable to validate the checklist and keep it updated according to the latest evidence.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed equally to this work.
Funding This work was supported by funds from the Università degli Studi di Torino, Ricerca Locale Ex 60% 2021 to C. Cena. Grant/award number: not applicable.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.