Article Text

Abstract
Objective To explore emergency department (ED) and urgent care (UC) clinicians’ perceptions of digital access to patients’ past medical history (PMH).
Methods An online survey compared anticipated and actual value of access to digital PMH. UTAUT2 (Unified Theory of Acceptance and Use of Technology 2) was used to assess technology acceptance. Quantitative data were analysed using Mann-Whitney U tests and qualitative data were analysed using a general inductive approach.
Results 33 responses were received. 94% (16/17) of respondents with PMH access said they valued their PMH system and all respondents with no digital PMH access (100%; 16/16) said they believed access would be valuable. Both groups indicated a high level of technology acceptance across all UTAUT2 dimensions. Free-text responses suggested improvements such as increasing the number of patient records available, standardisation of information presentation, increased system reliability, expanded access to information and validation by authoritative/trusted sources.
Discussion Non-PMH respondents’ expectations were closely matched with the benefits obtained by PMH respondents. High levels of technology acceptance indicated a strong willingness to adopt. Clinicians appeared clear about the improvements they would like for PMH content and access. Policy implications include the need to focus on higher levels of patient participation, and increasing the breadth and depth of information and processes to ensure patient record curation and stewardship.
Conclusion There appears to be strong clinician support for digital access to PMH in ED and UC; however, current systems appear to have many shortcomings.
- Access to Information
- Electronic Health Records
- Health information exchange
- Emergency Service, Hospital
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Access to Information
- Electronic Health Records
- Health information exchange
- Emergency Service, Hospital
What is already known on this topic
Providing emergency department (ED) and urgent care (UC) access to patients’ past medical history (PMH) is often a key justification for large investments in shared electronic health records (SEHR) systems.
ED and UC clinicians have not accessed PMH to the extent that SEHR system implementers hoped they would.
There are a range of SEHR and PMH access systems in use that vary in design and effectiveness.
PMH access is higher for specific groups such as older or sicker patients.
What this study adds
Clinicians value being able to obtain high-quality PMH via an SEHR.
To be useful in a range of circumstances, PMH needs to provide a succinct summary of a patient’s health status, current treatment regime and access to a wide spectrum of detailed PMH data relevant to the presentation.
ED and UC clinicians want to obtain PMH via a trusted clinical source.
By better understanding the attributes that ED and UC clinicians value, we can clarify high-value SEHR use cases and designs.
High levels of technology acceptance indicate a strong willingness to put in effort to adopt SEHR.
How this study might affect research, practice and/or policy
Health system leaders should be encouraged to develop SEHR systems in close consultation with ED and UC clinicians.
Designing SEHR/PMH access systems enabling curation by a trusted source will increase the level of use.
Effort put into standardising the representation of source data is likely to increase utilisation.
Background
A shared electronic health record (SEHR) system is distinguished by its availability to multiple healthcare providers, typically working from different institutions across health services. SEHRs are intended to facilitate clinician access to past medical history (PMH) to improve patient care and/or reduce the cost of care.1 A primary reason for building an SEHR system is to ensure that important patient information is available for unscheduled care such as medical emergencies.2 3
Our previous review of SEHR use during unscheduled care found that while many SEHRs were large in scale and serviced many millions of patients, reported record utilisation rates by clinicians were variable but low.4 Higher record access rates were found in USA and Israeli healthcare maintenance organisations (16%–30%). Lower rates were reported for nation-scale systems (1.5%–2%) or when data exchange occurred between disparate provider systems. Our subsequent study of SEHR access in a hospital emergency department (ED) demonstrated that records were routinely used and usage was growing over time.5 Usage patterns revealed the highest rates for specific groups such as older or sicker patients.
It seems therefore that there are use cases where SEHR access is of higher value, and as a corollary, there should be SEHR designs that are more acceptable because they optimise support for those use cases. To clarify high-value SEHR use cases and designs, we undertook a survey of ED and urgent care (UC) clinicians across Australia and New Zealand. The study compared clinicians’ experiences using an SEHR to access PMH to those of clinicians with no current access, and explored technology adoption levers and specific design attributes that may make SEHR access most useful. We also explored related questions, including the value of accessing PMH during the COVID-19 (SARS-CoV-2) pandemic, of accessing advance care directives (ACDs), as well as the potential risks of using PMH, and specifically, whether accessing such data introduces a framing bias that negatively influences clinician decision making.6
Typically, an individual’s perceptions of a new technology change after exposure to it. In this study, we sought to compare the expectations of ED and UC clinicians without access to their patients’ PMH to the experiences of those clinicians that did have access.
Methods
Study design
We surveyed ED and UC clinicians practising in Australia and New Zealand.
Responses from ED and UC clinicians who reported having access to SEHR systems containing patients’ PMH respondents were compared with those of clinicians who reported that they had no access (non-PMH respondents). Analysis groups were based on self-reported access to SEHR.
We compared the anticipated versus perceived actual overall value of access to patients’ PMH and the anticipated and actual perceived value by patient age, triage category and presenting condition. We compared the anticipated versus perceived actual value of separate sections of the patient record (demographic data, medications, pathology, problem list) and information from additional external sources.
Setting and study participants
Participants were members of either The Australian College of Emergency Medicine, the registration body for all Australian and New Zealand ED doctors; or The Royal New Zealand College for Urgent Care, the registration body for New Zealand’s UC doctors.
Procedure
Permission to survey college members was granted by their respective research committees. Advertisements were placed in the electronic newsletters of each organisation. The advertisements contained an electronic link to the survey.
A Qualtrics survey containing 35 multiple-choice questions using a 5-point Likert symmetric agree–disagree scale, with another eight questions inviting written responses was created (see online supplemental appendix 1). Wording was tailored to reflect whether respondents had or did not have access to an SEHR. The survey was conducted from 8 February 2021 to 15 September 2021.
Supplemental material
Analysis
Survey data were exported from Qualtrics into SPSS V.26 and analysed using Mann-Whitney U tests to report a median value and IQR for each comparison. Differences were considered to be statistically different when p<0.05.
Free-text answers were analysed using a general inductive approach,7 to condense response data into a brief summary form and identify common themes from the data.
Measures
We captured each respondent’s age, gender, length of time in practice, region, and whether they were working in a rural, regional or urban setting.
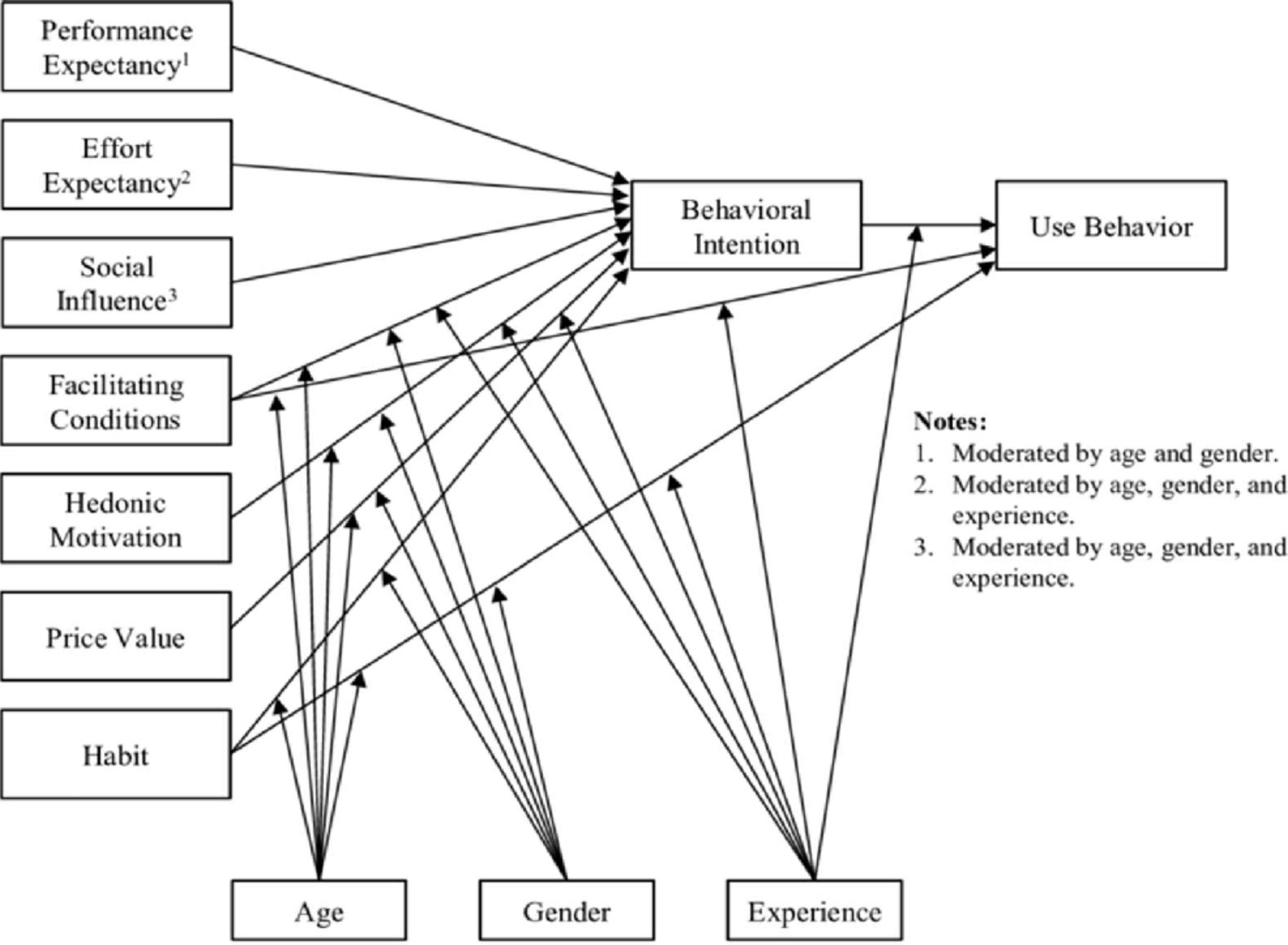
A set of technology acceptance questions within the survey were designed using UTAUT27 (the Unified Theory of Acceptance and Use of Technology 2) framework (see figure 1). UTAUT2 is used to identify users’ behavioural intentions in relation to a new technology.
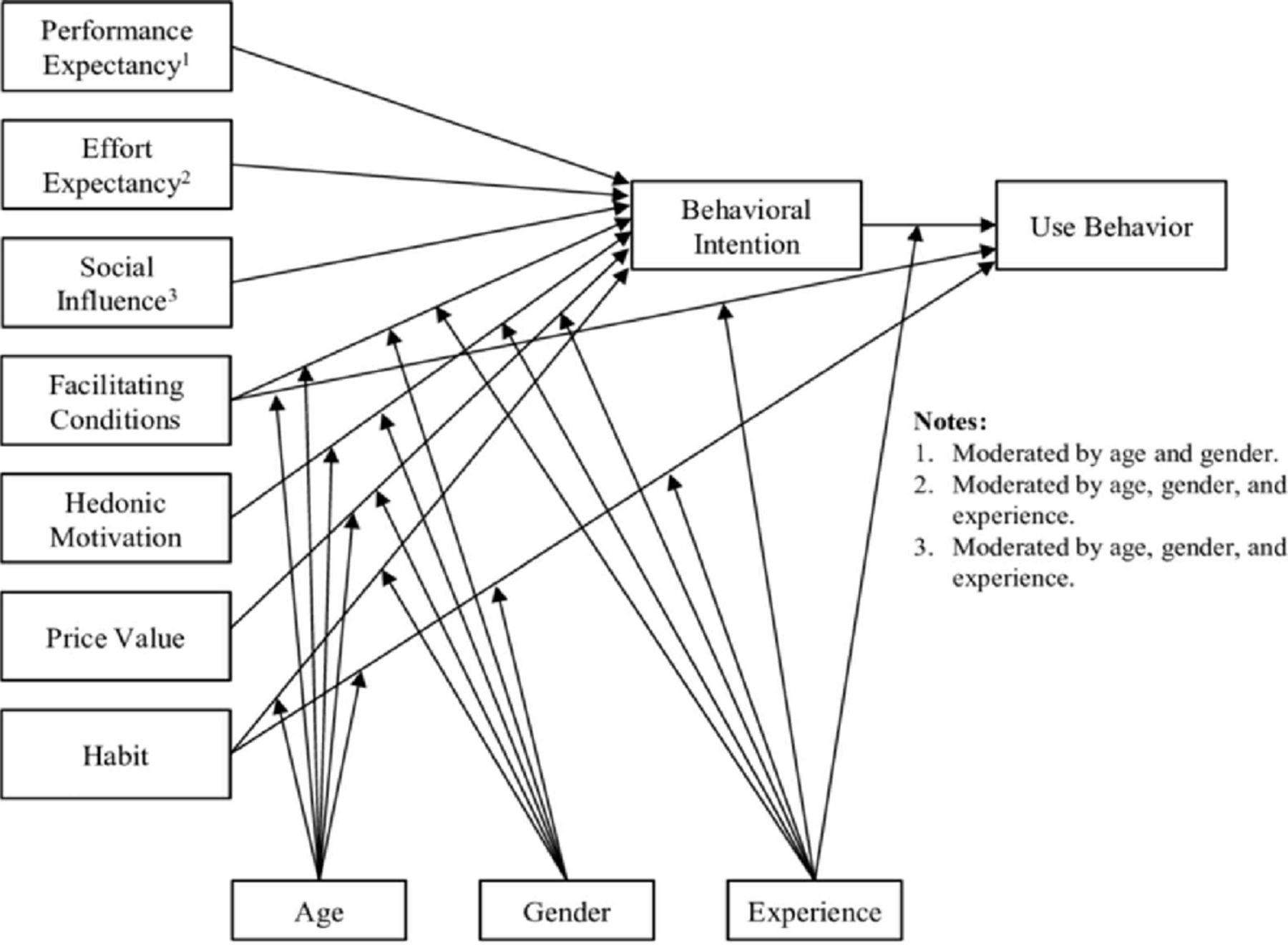
The Unified Theory of Acceptance and Use of Technology 2 (from Venkatesh et al 8reproduced courtesy of MIS Quarterly).
We compared respondents with and without access to PMH, including their behavioural intention to use an SEHR for PMH access, the perceived value of such access, and the different circumstances or clinical condition types for which they would access PMH. Acceptance questions were designed to measure the seven UTAUT2 factors that influence the uptake of new technology: performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, price/value and habit.8 (see online supplemental appendix 2).
Supplemental material
Respondents were given eight free-text questions inviting them to suggest potential PMH system capabilities and improvements to their existing systems. We also sought respondents’ views on a small set of questions including accessing ACDs via an SEHR and the risk of framing bias when accessing an SEHR. A framing bias occurs when the manner of information presentation influences its interpretation.5 We finally explored the likely value of accessing PMH during a pandemic.
Results
We obtained responses from 33 ED and UC clinicians from New Zealand and Australia during the COVID-19 pandemic. 18 respondents were female, 14 male and 1 respondent did not state a gender. Five respondents practised in rural locations, 5 in provincial centres and 23 practised in an urban setting.
Sixteen respondents said that they had no source of PMH (non-PMH respondents), and 17 respondents indicated they accessed PMH via one of a variety of regional or national SEHR systems (PMH respondents).
Of the 17 respondents who reported having access to SEHR, 53% (n=9) reported using their SEHR system to look at PMH for more than 60% of their patients and 35% (6/17) reported obtaining PMH for more than 80% of patients. Most PMH respondents said their SEHR system was highly valuable (59%; n=10), while 35% (n=6) said it was somewhat valuable (see table 1). All non-PMH respondents (100%; n=16) said that they believed PMH access would be valuable. Non-PHM respondents were uniformly of the view that PMH access would be highly valuable, whereas PMH respondents were more diverse in their assessment, with responses not equally distributed between the groups despite having the same median (non-PMH: Mdn=5, n=16 vs PMH: Mdn=5, n=17, p=0.005, r=0.449).
PMH respondents’ views regarding the value of their existing PMH system
We asked non-PMH respondents whether they would only rely on PMH if they knew it to be up to date and accurate. 75% (12/16) agreed or strongly agreed. However, 12.5% (2/16) were neutral and 25% (4/16) of non-PMH respondents disagreed, saying they would review any available information, regardless of whether they had concerns about its completeness or accuracy.
We saw the following statistically significant differences:
More non-PMH respondents expected PMH to be valuable for treating eye problems: (non-PMH: Mdn=4, n=16 vs PMH: Mdn=3, n=17, p=0.040, r=0.36) and for treating head injuries: (non-PMH: Mdn=5, n=16 vs PMH: Mdn=3, n=17, p=0.011, r=0.44).
More non-PMH respondents expected PMH to be valuable for adult patients: (non-PMH: Mdn=5, n=16 vs PMH: Mdn=4, n=17, p=0.043, r=0.35).
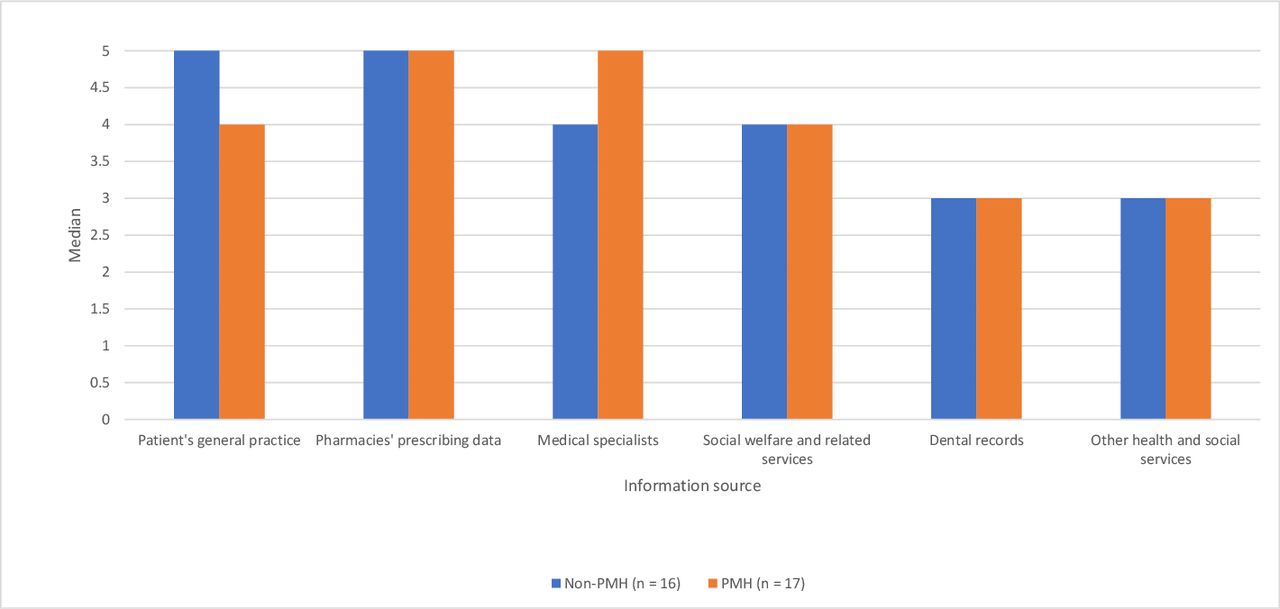
More non-PMH respondents wanted to access general practice-held data: (non-PMH: Mdn=5, n=16 vs PMH: Mdn=4, n=17, p=0.040, r=0.36) (see figure 2).
We saw no statistical differences between PMH and non-PMH respondents’ perceptions of value for most conditions, patient age groups, history types and history sources (see table 2).

{kind=link}
{kind=link}
A comparison of non-PMH and PMH respondents’ views of the value of access to external information sources. Responses are on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). PMH, past medical history.
Comparison of non-PMH and PMH respondents’ views of PMH access
PMH respondents’ reduced assessment of the value of PMH for treating adult patients confirms our earlier finding that PMH respondents found SEHR most useful when treating elderly patients and infants.
Non-PMH and PMH respondents were positive about the value of PMH in managing a patient suspected of exposure to infection during a pandemic and had similar estimates of the proportion of patients’ records they would expect to look up (see table 2).
All non-PMH respondents believed access to ACDs would be valuable: (M=4.53, SD=0.000). PMH respondents also saw value in having access to ACDs: (M=3.12, SD=0.857).
UTAUT2 analysis
Our UTAUT2 analysis showed that non-PMH and PMH respondents had largely similar responses to the acceptability of digital PMH access across all seven technology acceptance factors. PMH respondents found PMH access to be valuable. Non-PMH users’ similarly positive assessments of the likely benefits mean that they are likely to expend considerable effort to adopt PMH-access technology once it becomes available.
There was a considerable alignment of views and only two exceptions to that: non-PMH respondents believed their colleagues would be more supportive of PMH use: (non-PMH: Mdn=4.5, N=16 vs PMH: Mdn=4, n=17, p=0.023, r=0.40) and non-PMH respondents were more positive about the level of economic value of PMH to their organisations: (non-PMH: Mdn=5, n=16 vs PMH: Mdn=4, n=17, p=0.021, r=0.40) (see table 3).
Comparison of PMH and non-PMH respondents’ views on technology adoption factors (UTAUT 2)
Free-text responses
Free-text responses from PMH and non-PMH respondents are presented in Appendix 3. Five key themes emerged after analysis:
Reach: Respondents indicated a desire for more patients to have accessible PMH, thus improving the likelihood of locating a record. One respondent stated: ‘Many patients do not have a record.’ Other respondents reported difficulties finding records because they were held on multiple different unconnected regional systems. A respondent stated: ‘There is no significant communication between regions, that is, the electronic data records are separated amongst the different regions.’
Ease of use: Ease of use was a common issue: ‘Information needs to be quickly and easily accessible, and in a format that is useable, that is, summarised, with option to expand out any diagnoses/areas for investigation results, specialist opinions, management, medications.’ Several respondents indicated frustration, with one saying ‘Too many clicks, too slow to load. Information (is) spread across too many different systems that don't talk to each other in real-time or to other hospitals/healthcare systems.”
Value of information: Some respondents expressed a need to increase the value of the information available, that is, increasing the depth, breadth and quality of information in a PMH. One respondent stated: ‘The information available needs to include all aspects including mental health. These are often separate which can lead to errors.’ Another respondent commented: ‘It must be up to date or you are basing decisions on old information. This is especially relevant with medication information.’ Some clinicians wanted general information about a patient’s health and current treatment, whereas others had specific interests in a very wide range of detailed aspects of a patient’s health.
Integrity of information: The fourth theme was the need to be able to rely on information provided by an SEHR, with one respondent saying: ‘Curation of PMH is essential to the usefulness of any system designed to help ED clinicians, but what is critical is; who does it?—It’s a fairly high-end cognitive task and so can’t be automated or easily contracted out. It needs someone with a thorough understanding of the situation.’
Respondents indicated that while any information they can access is likely to have some value, they wish to be able to rely on information they obtain as being completely trustworthy and able to be acted on with absolute certainty: ‘In practice the best approach is to get information from someone at a reasonably high level who has put the effort in to understanding the situation for purposes other than providing a summary.’
The risk of framing bias: In the free-text responses, respondents indicated various views regarding potential risks arising from forming incorrect assumptions based on reliance on PMH. However, several respondents commented that that while availability of a patient’s PMH can lead to bias, the benefits of having access to PMH far outweigh the risks of being without it.
“I think the risks are lower than current risks of not having access to this information.”
“PMH can lead to bias but I think benefit far outweighs risk.”
“Less information is associated with significant risk.”
“I feel the errors would be worse by NOT knowing the information”.
Respondents listed 29 categories of PMH they would like to have made accessible via an SEHR . These included:
Previous radiology, pathology.
Hospital summaries.
Medication history.
Direct access to GP notes.
Patient’s goals of care.
Preferred language.
Next of kin’s name and contact details.
Care planning information/advance directives.
Enduring power of attorney.
Information from external services such as methadone clinics, drug addiction services, aboriginal medical services.
Previous ED presentations or hospital admissions.
Records held by nursing homes and palliative care services.
Data on conditions treated and/or surgeries performed in private hospitals.
See full list in online supplemental appendix 3.
Supplemental material
Discussion
ED clinicians and UC clinicians are aware that their lack of knowledge about a presenting patient’s healthcare status and previous and current treatment history is a challenge for many patient encounters.9 While many studies demonstrate that clinicians complain of burnout associated with the use of electronic health records,10 11 respondents in this study indicated that access to high-quality SEHR data and digital PMH was valuable and worth accessing.
PMH respondents’ reduced assessment of the value of PMH for treating adult patients confirms our earlier finding that PMH respondents found SEHR most useful when treating elderly patients and infants.5
Developing PMH access via SEHR systems has been one of the main objectives of most national health systems over the past three decades. However, few national-scale or regional PMH systems have been reported doing so successfully. The largest and most expensive attempt was the UK Government’s Summary Care Record (SCR) programme. Key problems hampered the SCR, including a lack of accurate and relevant data, ongoing system integration issues and interoperability problems, and lack of trust by patients over the privacy and security of their sensitive data. Privacy fears, concerns about the accuracy and relevance of data, and challenges to SEHR integration remain live issues in this study.
Typically, an individual’s expectations for a new technology change after exposure to it. In this study, ED and UC clinicians’ responses showed that clinicians without access to their patients’ PMH had very similar expectations and objectives to those who do.
Both groups’ responses indicated that they wanted access to an SEHR that provided a robust, easily accessible, up-to-date general picture of a patient’s health status and treatment, from which they could access links to far more detailed information when needed. In addition, clinicians want PMH data presented in a uniform format that is easy to navigate and interpret and that comes from an authoritative and trusted source.
Respondents identified multiple improvements to their existing PMH access including broadening access to include more patients, making them more dependable and easier to use, while providing access to a greater breadth and depth of information and the need to develop processes that enable patient record curation and stewardship.
While incremental improvements can be made on a case-by-case basis, a more focused and systemic approach to SEHR design for PMH may be needed. Unscheduled care represents a clear use case for SEHRs, where system use is not to record activity but to inform decisions, and this difference is likely to have specific design implications.12
This echoes earlier work. Fries stressed the importance of standardised presentation to improve the speed and ease with which clinical data could be reviewed and acted on.13 Whiting-O'Keefe et al demonstrated the utility of methodological patient record summarisation versus less rigorously structured record formats.14
Given the pressures on healthcare systems and the level of resources spent to date on patient record sharing, it is surprising that more progress has not been made. ED and UC clinicians are still a long way away from having consistent and reliable access to patients’ PMH, which is information that almost always exists already, somewhere, buried deep in a healthcare system.
The price of this inadequacy appears significant. The direct costs are potentially huge, with many countries spending billions of dollars on these systems. However, the opportunity costs are likely even greater. Health system efficiency and patients’ quality of life could both be greatly improved if patients’ PMH could be shared more effectively.9 15
Limitations
This study was undertaken throughout 2020 and 2021 when Australia and New Zealand were affected by the worldwide COVID-19 global pandemic. All hospital EDs and UC clinics were under considerable pressure during this period. Despite considerable efforts by The Royal Australasian College for Emergency Medicine and The Royal New Zealand College of Urgent Care, the survey response rate was lower than anticipated. Accordingly, the results may have limited generalisability to the population of ED and UC clinicians throughout New Zealand and Australia. However, we identified the need to create readily accessible and completely reliable patient record data sets; findings which can be further explored in future research. Such research might provide insights that would enable us to build PMH access systems that will become indispensable within ED and UC settings.
Conclusion
There is strong clinician support for access to ED and UC patients’ PMH. ED and UC clinicians know what they would like to see in a PMH system, with both non-PMH and PMH respondents’ views closely aligned. Designing electronic record systems specifically optimised for ED and UC decision support appears to be both needed and likely to come with significant benefits.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Macquarie University HREC (Australian Human Research Ethics Committees) Approval number: 52020905322939. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are grateful to the executive officers and staff of The Royal Australasian College for Emergency Medicine and The Royal New Zealand College of Urgent Care.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TCB conceived this research and designed and conducted the study with guidance from, and under the supervision of, EC and DL. TCB drafted the manuscript with input from all authors. All authors provided revisions for intellectual content. All authors read and approved the final manuscript. TCB is the guarantor.
Funding This review was supported by the NHMRC Centre for Research Excellence in eHealth (APP1032664).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.