Article Text

Abstract
Objectives This study aimed to evaluate the effect of the phone reminder system on patient-centred TB treatment adherence during continuation phase, where patients are responsible for taking medication at home.
Methods We conducted a two-arm randomised controlled trial on adult patients with TB during the continuation phase. In the intervention arm, patients received routine care plus phone-based weekly pill refilling and daily medication reminders. In the control arm, participants received only routine care. A covariate adaptive randomisation technique was used to balance covariates during allocation. The primary outcome was adherence to patient-centred TB treatment, and secondary outcomes included provider–patient relationship and treatment outcomes. We applied per-protocol and intention-to-treat analysis techniques.
Results We randomised 306 patients to intervention (n=152) and control (n=154) groups. Adherence to patient-centred TB treatment was 79% (110/139) in intervention and 66.4% (95/143) in control groups, with relative risk (RR) (95% lower CI) (RR=1.632 (1.162 to ∞); p=0.018, one tailed). Good provider–patient relationship was 73.3% (102/139) in intervention group and 52.4% (75/143) in control group, p=0.0001. TB treatment success was 89.5% (136/152) in intervention group and 85.1% (131/154) in control group, p=0.1238.
Conclusions Mobile phone-based weekly refilling with daily medication reminder system improved adherence to patient-centred TB treatment and provider–patient relationship; however, there was no significant effect on treatment success.
Trial registration number Pan African Clinical Trials Registry (PACTR201901552202539).
- medical informatics
- patient care
Data availability statement
All data relevant to the study are included in the article. The protocol is published and available in the same journal (BMJ Health & Care Informatics).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
What is already known?
mHealth technologies overcome barriers against access and quality of health care.
Virtually-observed (video) therapy improves patient’s adherence to tuberculosis (TB) treatment.
Interactive text messaging found effective but only for patients who can read and write.
Phone-reminder systems commonly applied for daily TB medication, but refilling paid less attention.
What does this paper adds?
A one-way, combined text and graphic reminder system could engage non-educated TB patients in resource limited settings.
Integrating both daily medication and weekly pill-refilling reminders could improve adherence to patient-centered TB treatment.
Background
Globally, non-adherence to tuberculosis (TB) treatment has been a major challenge affected by an interplay of factors, including healthcare team and system-related, socioeconomic, condition-related, therapy-related and patient-related factors.1 2 Patients’ failure to adhere to TB treatment results in poor treatment outcomes like drug resistance, relapse and death.3–5 In Ethiopia, non-adherence to TB treatment remained a major challenge due to several reasons.6–9 Studies reported that poor provider–patient relationship, poor knowledge towards TB and its treatment, distance to the health facility, competing employment, family commitments and adverse clinical experiences were common reasons for non-adherence to TB treatment.10 11 One of Northwest Ethiopia’s studies reported that forgetfulness accounted for 34% of patient’s reasons for non-adherence to TB treatment.6 12
Studies show that non-adherence to TB treatment worsens during the continuation phase, where patients took the responsibility of managing their TB treatment at home (patient-centred treatment).12 13 Unlike the intensive phase, patients in the continuation phase are responsible for refilling their pills weekly at the nearby clinic and taking their pills at home under community supporters’ observation. However, community supporters may be busy with their own routine business and find it difficult to remind and follow patients for such a long period. Hence, implementing digital health technology could improve patient adherence to TB treatment.
Digital health interventions, including mobile health (mHealth), have now brought attention to the strategy to end the global TB epidemic by 2035.14 As an opportunity, mobile cellular penetration in Africa and other regions of the world has been estimated to grow more than ever.15 In Ethiopia, mobile subscriptions have reached more than 46 million.16 Evidence showed that mobile technologies had been found useful for resource-limited countries to overcome barriers against access to healthcare and the quality of care delivery.17 The WHO has already established its global task force on digital health to support the development of digital health innovations in global efforts to improve TB care and prevention.18
Evidence indicated that mHealth technology is a feasible, acceptable and promising solution to improve patient adherence to TB treatments in different settings.19–24 Previous studies used video (virtually)-observed therapy,21 25–29 which could not be widely feasible for many resource-limited settings. Some studies used medication reminder systems but focused on daily medication reminders and paid less attention to pill-refilling reminders, though refilling is equally important for patient adherence to TB treatment. Most studies used only text messaging and excluded patients who cannot read and write text messages.20 21 23 24 One study applied both text and graphic reminders but was limited only to daily medication reminders and the follow-up period was for 2 months.30 Our study engaged both illiterate and literate patients using simple graphics and text messages for weekly pill refilling, and daily medication reminder runs for 4-month continuation phase. We hypothesised that in addition to routine care, applying a daily medication reminder with weekly pill-refilling reminders could improve patient-centred TB treatment adherence.
Methods
We used Consolidated Standards of Reporting Trials to report the study’s findings.31 The details of the methods have been described in the protocol.32
Trial design
We implemented a two-arm randomised controlled trial (RCT) to evaluate the effect of weekly pill refilling and daily medication reminder systems on patient’s adherence to patient-centred medication, provider–patient relationships and treatment outcomes.
Participants and setting
The study population includes all adult, drug-sensitive and new patients with TB on the continuation phase at health centres and hospitals in Central Gondar Zone and Gondar town administration. These included eight districts from Central Gondar Zone and Gondar town administration. The districts include Gondar Zuria, Tach Armachio, Wegera, East Dembia, West Belesa, Takusa, East Belesa, Alefa and Gondar town administration. The study area consists of 74 functional public health facilities (health centres and hospitals) serving more than 2.9 million people overall in the area. Eligibility criteria include all new drug-sensitive patients enrolled in continuation phase, aged 18 years and above, who own mobile phone, willing and able to provide informed consent. The study excluded patients with no/limited mobile networks at their home, enrolled in multidrug-resistant TB, and already enrolled in another study that could affect the study’s outcomes. To reduce attrition bias, we excluded patients who planned and decided to transfer to another health facility.
Interventions
We developed a web-based reminder system tailoring the local context, piloted the prototype and published it before implementation.33 The basic features of the system include patient registration, scheduling reminders, visualisation and generating reports. This trial was implemented using the web-based reminder system. Development of the system followed a waterfall technique34 with stakeholders’ involvement, including TB focal care providers, information technology and health informatics experts.
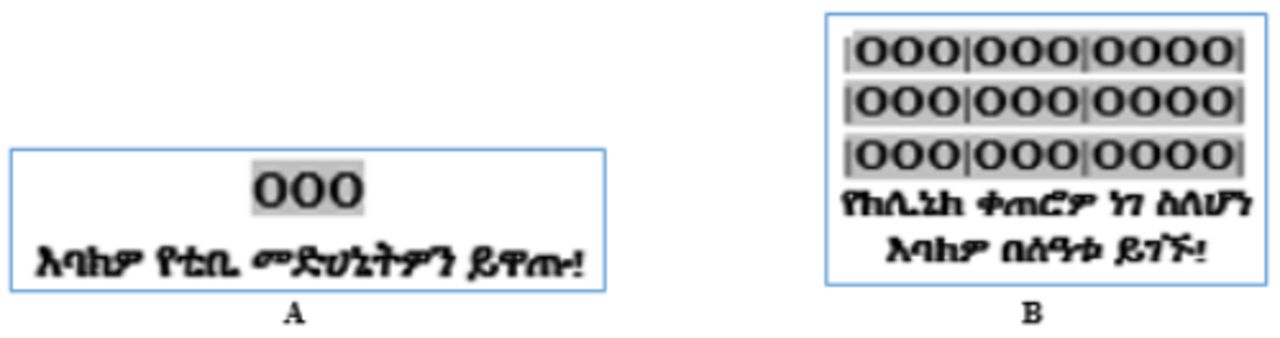
Participants in the intervention arm, in addition to routine care, received weekly pill refilling and daily medication reminders using graphics-based and text messages in the local language (Amharic). The graphic reminder was intended to engage illiterate patients who cannot read text messages. In figure 1, ‘A’ represented pills for daily medication followed by Amharic text to mean ‘Please take your pills’; while ‘B’ represented a strip of pills to refill followed by Amharic text to mean ‘your clinic appointment is tomorrow, please come on time’.

Graphic and text message (Amharic) to remind daily medication and weekly pill refilling, Northwest Ethiopia, 2020.
Before initiating the intervention, each participant on the intervention arm received a face-to-face orientation on the use of graphic and text messages for 5 min during enrolment. Immediately after enrolment, a welcoming message was sent to the patients in the intervention group, which aimed to improve their engagement in the treatment through motivation. Medication reminders were sent every day from 07:30 to 08:00 to remind the conventional time (08:30) for taking daily TB pills; whereas pill-refilling reminder was sent a day before the due date (appointment date) from 18:30 to 19:00. The intervention was provided for 4 months of the continuation phase.
Routine care
The control arm received only routine care. Routine care in continuation phase TB treatment means patients take their daily medication at home with the help of TB treatment supporters (TTS). TTS is either a health extension worker (community health worker), family member, neighbour, workmate or community figure trained to observe, educate and remind patients for the optimal TB treatment administration at home.35
Outcomes
The primary outcome of the study was adherence to patient-centred TB medication during the continuation phase. During the continuation phase, we measured adherence to TB treatment using the shorter form, 11-item Adherence to Refill and Medication Scale (ARMS).36 37 The items include the following:
How often do you forget to take your TB medicine?
How often do you decide not to take your TB medicine?
How often do you forget to get prescriptions filled?
How often do you run out of TB medicine?
How often do you skip a dose of your TB medicine before you go to the doctor?
How often do you miss taking your TB medicine when you feel better?
How often do you miss taking your TB medicine when you feel sick?
How often do you miss taking your TB medicine when you are careless?
How often do you change your TB medicines’ dose to suit your needs (like when you take more or fewer pills than you’re supposed to)?
How often do you put off refilling your TB medicines because they cost too much money?
How often do you plan ahead and refill your medicines before they run out?
The original ARMS tool consists of 12 items, including two subscales, an 8-item medication-taking subscale and a 4-item refill subscale.36 One of the items, ‘How often do you forget to take your medicine when you are supposed to take it more than once a day?’ was not relevant to TB medication since TB pills often are taken once a day. Each of the items was structured as a Likert scale with responses of ‘none’, ‘some’, ‘most’, or ‘all’ of the time, which were given values from 1 to 4.
As a secondary outcome, treatment success rate (TSR) was assessed. According to the WHO TB treatment guideline, treatment outcomes are measured as TSR, which is defined as the sum of patients with TB cured and/or completed their treatment. Cured is a patient with pulmonary TB with bacteriologically confirmed TB at the beginning of treatment which was smear or culture negative in the last month of treatment and on at least one previous occasion. Treatment completed is a patient with TB who completed treatment without evidence of failure but with no record to show that sputum smear or culture results in the last month of treatment and on at least one previous occasion were negative, either because tests were not done or because results are unavailable. Defaulted is a patient whose treatment was interrupted for 2 consecutive months or more. Treatment failure is a patient with TB whose sputum smear or culture is positive at month 5 or later during treatment. While death is a patient with TB who dies for any reason before starting or during the course of treatment.38
It was also planned to measure patient attendance to TB clinics39 ; however, it was not analysed because the weekly appointment scheme was not consistently practised by TB clinics. From our observation, some TB clinics appoint patients every 2 weeks, some every month, and some others allow family/treatment supporters to refill on the patient’s behalf. One of the reasons for the inconsistency was during the rainy season, patients were not willing to come every week. Patients used to delegate their treatment supporter during social events (like funerals) and whenever feeling sick.
As an additional analysis, we assessed the provider–patient relationship using a 7-item provider–patient relationship questionnaire adapted from previous studies.11 40 The items include patients’ satisfaction with the care provided, patient’s trust in care provider, frequency of phone call to the patient, the convenience of appointments, frequency of calls by the patient to care provider, patient feeling shame to question, and patients’ perceived compassionate and caring provider. It aimed to evaluate the effect of the intervention on smoothing the relationship between patients and care providers, as the provider–patient relationship was a factor affecting adherence to TB treatment.10 11 40
Sample size and sampling procedure
We calculated the sample size using STATA V.14 considering the assumption of superiority design. The sample size in the published protocol was 262.32 It was calculated using the proportion of adherence (p) from other similar studies and applying power (β=80%).9 The sample size was recomputed using our baseline proportion of patient adherence to TB treatment during the continuation phase (p1=64.2%) and p2=79.2% considering 15% minimum detectable effect size. The total sample size was 324 (162 in each study arm), considering α=5%, power (β=90%) and 10% attrition rate. The study tried to involve urban and rural settings to ensure representativeness in both hard-to-reach and urban settings. Eligible patients were recruited from 22 health facilities (15 health centres and 7 hospitals) using an open cohort from 15 July to 8 November 2019.
Randomisation, allocation and blinding
The participants’ eligibility was assessed and they were recruited using enrolment guides during the intensive phase aimed to initiate the intervention immediately at the start of the continuation phase. The study used a covariate adaptive randomisation (minimisation technique) to control and balance covariates’ influence on the study outcome.41 Simple randomisation (lottery method) was applied at the beginning for allocating the first subjects at each arm and in the middle when the subsequent patient’s characteristics appear not important to minimise imbalances across the covariate groups. Otherwise, every subsequent patient was assigned to the groups with an imbalance across the covariate groups using a minimisation algorithm. The covariates, including participants’ educational status (able and unable to read and write), sex (male, female), residence (urban, rural) and type of facility (health centre and hospital), were considered during randomisation. The research assistant provided an identification number to identify participants and carried out the randomisation process using a covariate algorithm. To reduce information contamination, we planned to include one, if more than one patient attending TB treatment from a household; however, the situation did not happen. The outcome assessors (care providers in TB clinic and endline data collectors) did not participate in patient enrolment, and endline data were collected using participant codes to mask each participant’s randomisation status purposely to reduce detection bias. The study participants have not masked due to the intervention’s nature that a study subject requires overt participation.
Data collection
Baseline data were captured using a participant enrolment guide from eligible patients during recruitment. Endline data were collected using phone-call interviews and patient registers in TB clinics at the end of 4-month follow-up (after completing the treatment course). In the protocol, we planned to conduct a face-to-face interview; however, data were collected using a phone-call technique due to the COVID-19-related movement restrictions. Training was provided for data collectors to reduce measurement bias related to the phone-call interview.
TB treatment outcomes were collected using checklists from registers in TB clinics. Endline data were collected from 20 January to 24 April 2020.
Statistical analysis
We used EpiData V.3.1 software for data entry and exported it to STATA V.14 for analysis. The family wealth index was calculated using principal component analysis technique.42 The study applied per-protocol analysis to evaluate patients’ adherence to patient-centred TB treatment using ARMS with 11 items dichotomised as 11 or >11. The provider–patient relationship was ascertained and dichotomised using a median score. Intention to treat was applied to evaluate treatment success. Absolute difference (AD) was computed to evaluate changes of outcome variables among intervention and control groups. Log-binomial regression was used to estimate the adjusted effect size controlling other variables. As a superiority design trial, we computed a one-sided hypothesis testing. Superiority tests were often computed as one sided in which the alternative and null hypotheses are reported as one of the study arms is better by more than a stated margin. Hence, we reported the lower bound of 95% CI with a one-sided p value.43
Result
Recruitment and patient flow
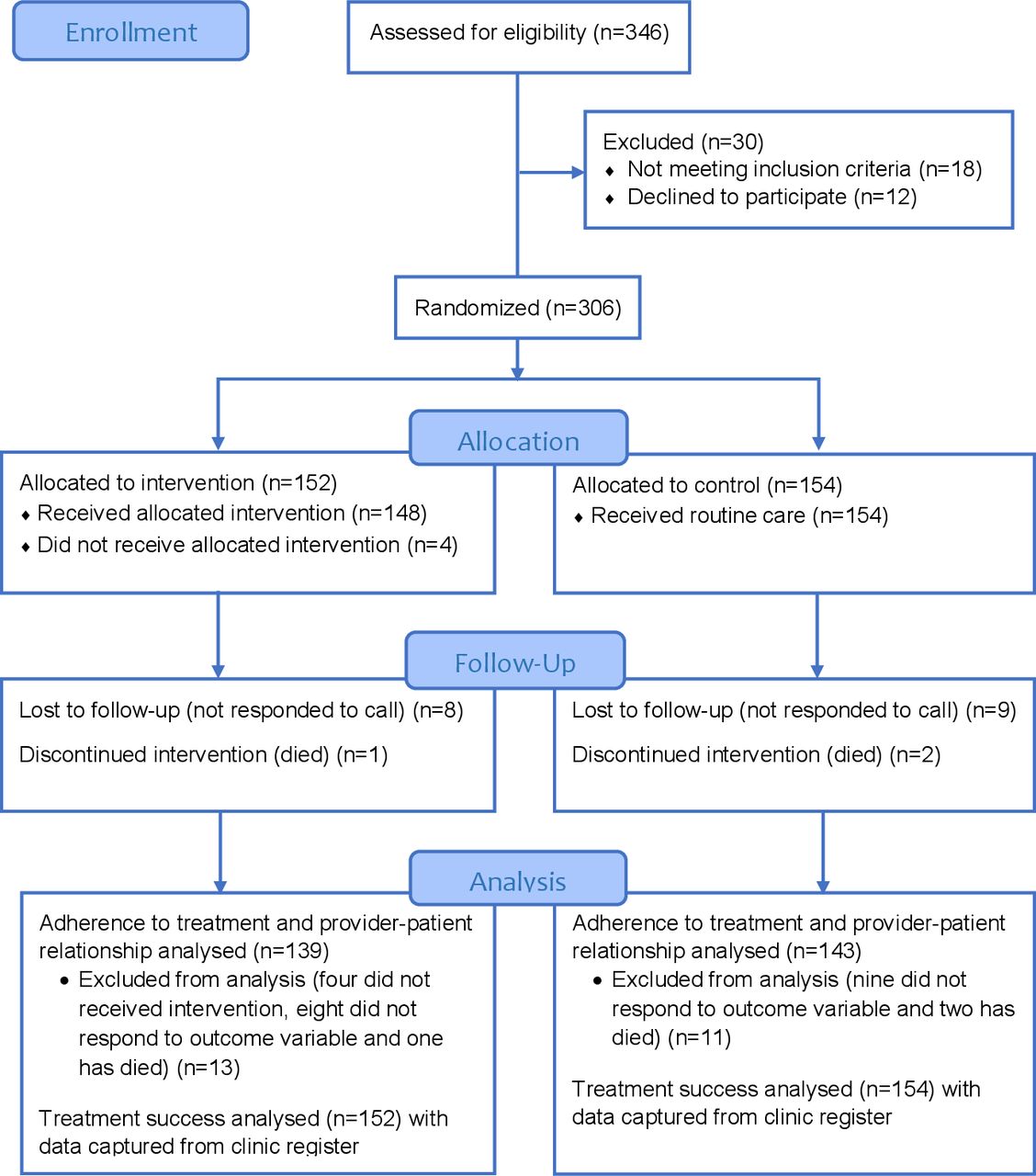
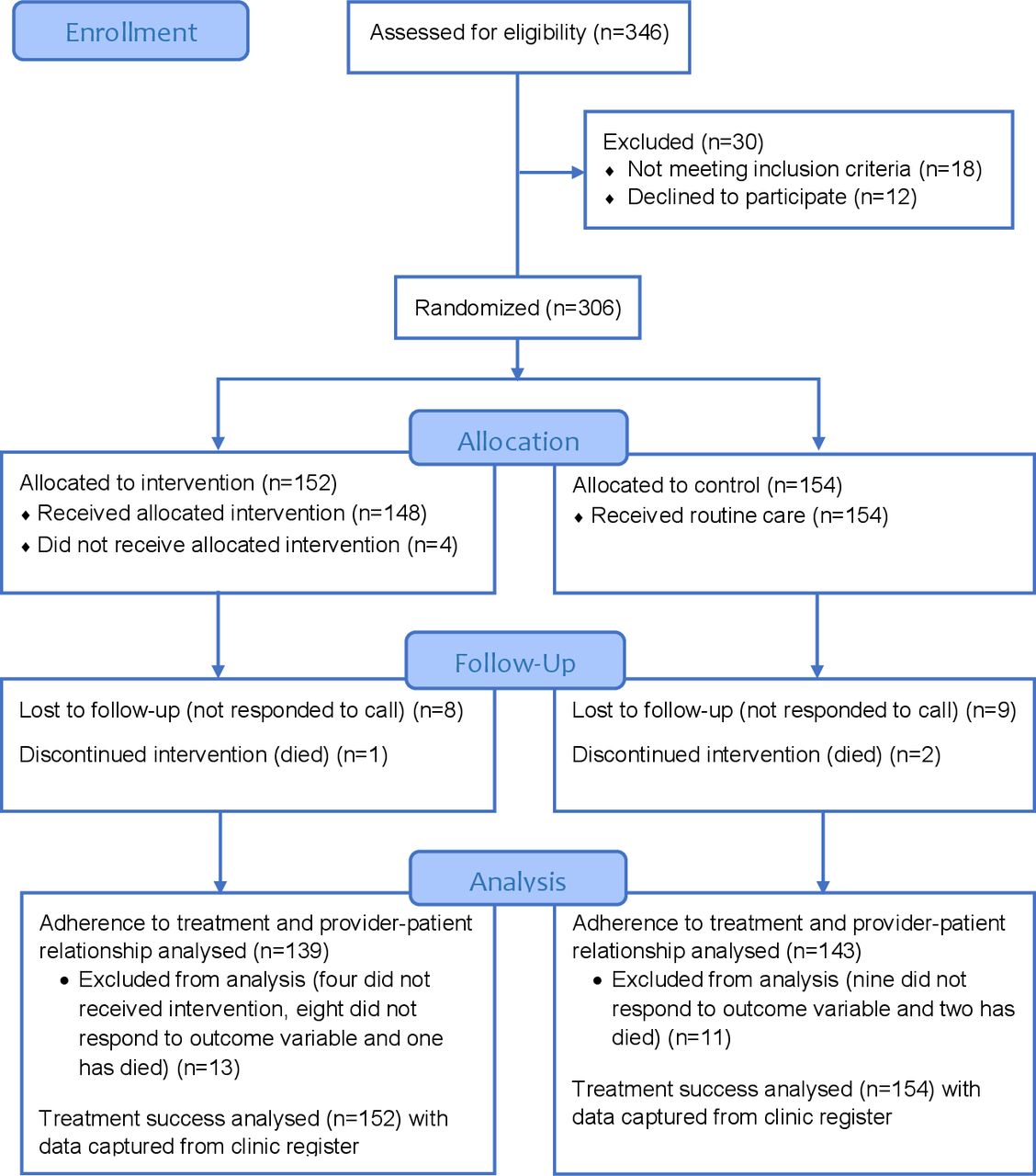
Three hundred forty-six patients were assessed for their eligibility to be included in the study from 23 July to 8 November 2019. Of them, we communicated with 318 potentially eligible patients, and 12 declined to participate in the study. Hence, we randomly allocated 306 eligible patients: 152 in intervention group and 154 in control group. Adherence to TB medication and provider–patient relationships were assessed using 282 participants (139 intervention group and 143 control group). The rest 3 (1 in intervention group and 2 in control group) died, 4 patients from the intervention group did not receive messages at all, 17 (8 in intervention group and 9 in control group) did not respond to the phone call-based endline assessment. We captured TB treatment outcomes for all 306 participants from facility records (figure 2).
{kind=link}
{kind=link}
The flow diagram of patient recruitment, intervention, follow-up and analysis.
Baseline data
The study included 306 (152 intervention and 154 control) participants for analysis. The majority of participants, 83 (54.6%) in the intervention group and 86 (55.8%) in the control group, were aged between 18 and 29 years. Of the total participants, 84 (55.3%) in the intervention group and 75 (48.7%) in the control group were men. According to the type of facility, 116 (76.3%) in the intervention group and 105 (68.2%) in the control group were enrolled in hospitals. Participants’ residence indicated that 115 (75.7%) in the intervention group and 117 (76%) in the control group were urban dwellers (table 1).
Baseline characteristics of participants, n=306 (152 intervention, 154 control), Northwest Ethiopia, 2020
Estimated effect size
Adherence to patient-centered TB treatment
Adherence to patient-centred TB treatment was found: 79.1% (110/139) in intervention group and 66.4% (95/143) in control group. The AD was 12.7%. The difference was statistically significant with one-tailed p=0.0083 (table 2).
The absolute differences (ADs) of patient adherence, treatment success and provider–patient relationships among intervention and control groups, Northwest Ethiopia, 2020
TB treatment success
The treatment success rate was computed as the sum of the rate of cure and treatment completion. The cure rate was 22% (33/152) of patients in the intervention group and 16% (24/154) in control group. About 67% (102/152) in intervention group and 70% (108/154) in control group have completed their treatment. Overall, the treatment success rate was 89.5% (136/152) in intervention group and 85.1% (131/154) in control group. The AD in the rate of treatment success between intervention and control groups was 4.4%. The Fisher’s exact test showed no significant difference in treatment success between intervention and control groups (p=0.1238).
About 2.6% (4/152) in intervention group and 1.3% (2/154) in control group were lost to follow-up. Transferred out was 7.2% (11/152) in intervention and 10.4% (16/154) in the control group. Treatment fuilure showed 0.7% (1/152) in intervention group and 1.3% (2/154) in control group. Death accounted 0.7% (1/152) patient in intervention group and 1.3% (2/154) in control group (table 2).
Provider–patient relationship
The provider–patient relationship was analysed as an additional variable considering its potential alter by the intervention. The finding has shown that 73.3% (102/139) of patients in the intervention group and 52.4% (75/143) in control group reported a good relationship with care providers in TB clinics. The AD between intervention and control groups was 20.9%, p=0.0001 (table 2).
Multivariable analysis
We run the adjusted log-binomial regression analysis to calculate the adjusted relative risk (RR) holding other covariates constant. We analysed the data using both two-tailed and one-tailed tests. A two-tailed test was conducted for baseline characteristics. A one-sided test was analysed for the intervention and control groups, where a superiority hypothesis was formulated.
The finding has shown that the intervention had a significant association with patient adherence to patient-centred TB treatment with one-tailed RR (95% upper CI) (RR=1.632 (2.294); p 0.018). All other covariates have no significant association with adherence to patient-centred TB treatment (table 3).
A multivariable analysis of covariates associated with patient adherence to home-based TB treatment, n=282 (139 intervention, 143 control), Northwest Ethiopia, 2020
Discussion
In this trial, a mobile phone-based reminder system improved adherence to patient-centred TB treatment and the provider–patient relationship compared with standard practice alone. The treatment success rate was also marginally higher in the intervention than in the control group; however, the difference was not statistically significant.
The AD of adherence to patient-centred TB treatment between intervention and control groups was statistically significant. However, it was not clinically significant as the difference was lower than the 15% minimum detectable effect size considered during sample size determination. It implies that further studies are needed with a bigger sample size to confirm its clinical impact. The study has shown that patient adherence was significantly higher among patients who received phone reminders than patients under routine care group. Similarly, in a study in Malaysia, the mean adherence was significantly higher in the short message service (SMS) intervention group compared with the control group after 6 months of follow-up.44 A similar study in China also revealed that a daily SMS reminder system has significantly improved adherence to TB medication.45 A study in Tanzania also indicated that graphics-based reminders improved patient’s adherence to TB treatment.46 Besides, a pooled analysis of evidence indicated that SMS had significantly improved adherence to tuberculosis treatment as compared with participants without mobile phone-based interventions.19
On the other hand, previous RCT studies in Cameroon, Argentina, China and Pakistan reported that patients who received SMS reminders showed improved adherence to TB treatment; however, the difference was not statistically significant.20 47–49 The variation may arise because most of the previous studies used pill count as a measure of adherence to TB medications which leads to bias since pill count was known to distort adherence to TB treatment.50 In this study, the measurement of adherence involved both refilling and medication questions that measure patients’ intentional and unintentional practices towards TB treatment.36 Unlike other studies, our intervention consists of a one-time welcoming message, a combined text and graphic reminder messages for weekly pill refilling, and daily medication with 5 min orientation for participants in the intervention group to understand messages; whereas most of the previous studies focused merely on daily medication reminders.
The study indicated that the proportion of treatment success was higher in the intervention group than in the control group; however, the difference was not statistically significant. Similarly, studies in South Africa, Cameroon and Pakistan showed that daily SMS reminders did not increase treatment success.47 49 51 However, one study in Thailand indicated that TB treatment success rates in the phone call reminder group were significantly higher. Similarly, a systematic review and meta-analysis indicated that the phone reminder system has a modest effect on the treatment success rate.22 It implies that large sample studies could be needed to detect a reminder system’s small effect size on TB treatment success rate.
In this study, patients in the intervention group have reported a better relationship with TB focal care providers as compared with patients in the routine care group. Likewise, studies in Lesotho, Mozambique and India indicated that SMS reminder systems are perceived to improve health communication quality between patients and care providers. Several studies also reported that mHealth tools could enhance patients’ motivation to be engaged in their medication.52–56 In this study, the provider–patient relationship was assessed using questions including patients’ trust in the care provider, not being afraid of asking about the service, making a call to and receiving a call from the provider, feeling happy with clinic appointment and providers taking time and care. Therefore, the finding implies that patients could feel cared for and build trust in the healthcare provider and the health system in general.
The current study applied one-way messaging using a combined text and graphic messages to engage both educated and non-educated patients. This was due to a reasonably higher proportion of patients in the study area who could not read and write. Despite this, other studies have proposed that two-way interactive messaging could significantly affect medication adherence.57 58 It could not be appropriate in such contexts as some of the study participants could not read and write texts.
Implication to research and practice
This study was the first of its kind in Ethiopia that could initiate similar studies to improve TB care and treatment. More RCTs are needed considering other messaging schemes like voice and video messages and a combination of different types. Studies are also needed to address the different and complex contexts in Ethiopia. It also required exploring acceptability, feasibility and implementation challenges of the system for TB treatment support. Our study tried to address the mHealth system from the patient side for adherence support. It also needed to evaluate the mHealth system’s effect from the care provider’s perspective whether it improves healthcare delivery.
A cost-effectiveness analysis is required for the intervention considering the complex contexts and the need to understand the underlying barriers of implementation before scaling up to routine practice. Despite this, mHealth technologies were generally suggested as cost-effective solutions to resolve communication barriers in the developing world.59 The previous study suggested that a graphics-based medication reminder system was more beneficial, cost-effective and accepted for use by most patients, including those with limited education.46
Limitations
This study applied a patient self-reported adherence to TB treatment that could underestimate the problem due to recall and social desirability biases.60 We tried to validate the instrument prior to actual data collection to overcome the social desirability biases. The composite items of the tool could trigger memory and responses that could reduce both recall and social desirability biases. This study included only patients who own a mobile phone that could affect the study findings’ generalisability to the study area’s general population. Studies indicated that phone sharing was a common practice in the study area.61 This study, however, did not apply this approach as phone sharing could not allow absolute access and use of the phone by the patients. The small sample size and considerably higher lost to follow-up of study participants could reduce the power of the test. This study did not evaluate the effect of the intervention on the sputum conversion rate on the 5th month, perceiving that needs the reminder system to involve care providers than patients.
Conclusion
In this study, daily medication reminders with a weekly refilling reminder system significantly improved patients’ adherence to TB treatment during the continuation phase. Patients in the intervention group also reported a better relationship with healthcare providers. The treatment success rate showed improvement in the intervention group; however, the effect was not statistically significant. Further studies to evaluate the intervention’s cost-effectiveness and underlying barriers considering the different and complex contexts would be important.
Data availability statement
All data relevant to the study are included in the article. The protocol is published and available in the same journal (BMJ Health & Care Informatics).
Ethics statements
Ethics approval
Ethical clearance was obtained from the Institutional Review Board (IRB) of the University of Gondar with an approval number O/V/P/RCS/05/1077/2018. The research assistant followed an enrolment guide to discuss participants’ rights and responsibilities, possible harms and benefits of participating in the study. After checking participants’ understanding of the trial, written informed consent was obtained from study participants. The study prohibited patient identifiers during data collection, storage and dissemination.
Acknowledgments
We would like to acknowledge the SEARCH (NORPART) Project for facilitating the student exchange for sharing research experiences at the University of Oslo. The authors are grateful to DDCF for covering the data collection cost of this study. We are also grateful to data collectors and TB focal care providers for their dedication to data collection and facilitation.
References
Footnotes
Contributors KDG, BT and KAG contributed to conception and study design. KDG, RL, BT and KAG participated in the analysis and write-up. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.