Article Text

Abstract
Objective To measure lookup rates of externally held primary care records accessed in emergency care and identify patient characteristics, conditions and potential consequences associated with access.
Measures Rates of primary care record access and re-presentation to the emergency department (ED) within 30 days and hospital admission.
Design A retrospective observational study of 77 181 ED presentations over 4 years and 9 months, analysing 8184 index presentations in which patients’ primary care records were accessed from the ED. Data were compared with 17 449 randomly selected index control presentations. Analysis included propensity score matching for age and triage categories.
Results 6.3% of overall ED presentations triggered a lookup (rising to 8.3% in year 5); 83.1% of patients were only looked up once and 16.9% of patients looked up on multiple occasions. Lookup patients were on average 25 years older (z=−9.180, p<0.001, r=0.43). Patients with more urgent triage classifications had their records accessed more frequently (z=−36.47, p<0.001, r=0.23). Record access was associated with a significant but negligible increase in hospital admission (χ2 (1, n=13 120)=98.385, p<0.001, phi=0.087) and readmission within 30 days (χ2 (1, n=13 120)=86.288, p<0.001, phi=0.081).
Discussion Emergency care clinicians access primary care records more frequently for older patients or those in higher triage categories. Increased levels of inpatient admission and re-presentation within 30 days are likely linked to age and triage categories.
Conclusion Further studies should focus on the impact of record access on clinical and process outcomes and which record elements have the most utility to shape clinical decisions.
- health care
- information management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
What is already known?
Provision of access for emergency department (ED) clinicians to patients’ past primary care records is a common justification for investment in shared electronic health record (SEHR) systems.
There are little data available on rates of SEHR access by ED clinicians, the circumstances in which access occurs or for which patients it is accessed.
What does this paper add?
Primary care record access over 4 years and 9 months by ED clinicians demonstrates that primary care records are routinely accessed when available via SEHR systems.
Primary care records are more frequently accessed for older patients, those presenting in higher triage categories and for patients presenting with specific conditions such as confusion, collapse/fall, postictal seizures, heart palpitations or chest pain as well as in situations in which no specific presenting condition could be identified.
Patients whose primary care records were accessed accounted for a disproportionately high percentage of overall ED presentations.
Background
A shared electronic health record (SEHR) system is distinguished by its availability to multiple healthcare providers, typically working from different institutions across a health service. SEHRs are intended to facilitate clinician access to previous medical history (PMH) and improve patient care or reduce the cost of care.1 A primary reason for building an SEHR system is to ensure important patient information is available for unscheduled care such as medical emergencies.2 3
Our previous review of SEHR use during unscheduled care found that while many SEHRs were large in scale and serviced many millions of patients, reported record utilisation rates by clinicians were variable.4 Higher record access rates were found in USA and Israeli healthcare maintenance organisations (16%–30%). Lower rates were reported for nation-scale systems (1.5%–2%) or when data exchange occurred between disparate provider systems.5 6 No studies in that review reported on clinical outcomes or patient safety, and no economic studies of SEHR access during unscheduled care were available.
Recent studies of US health information exchange systems (HIEs) have produced some evidence that accessing PMH may reduce the rate of admission from the emergency department (ED) and reduce the number of investigations required.7–10 Such results may not generalise, however, because of the structure and scope of primary care and ED in the USA, which is strongly influenced by funding model and a relatively small primary care system by international standards.11 12 In the USA, PMH availability is determined by which healthcare providers elect to join a Regional Health Information Organization (RHIO) and upload patient data into an HIE.10 13 Other nations have a more inclusive whole of population approach, often possible because of a strong public health system.10
Given the lack of evidence on SEHR system usage or impact outside the USA, we undertook a study to measure the rate of PMH access in a New Zealand emergency care setting, the attributes of patients for whom records were accessed, and sought to assess the association between record access and patient disposition after presentation to the ED.
Methods
Study design
An observational study was undertaken of patients presenting to EDs. Patients for whom a primary care record had been accessed during presentation on one or more occasions were compared with a matched cohort who had never had a primary care record accessed.
Setting and population
The Hawke’s Bay District Health Board (HBDHB) hospital ED is the only ED servicing the region. The Hawke’s Bay Region has a population of 151 179 people, 23% of whom are Māori (the indigenous people of New Zealand), which is higher than the New Zealand national average (14.9%) and 3% are Pasifika (Pacific Island peoples), which is lower than the national average (7.4%).14 The population is clustered in two major cities (Napier and Hastings), which have a combined population of 122 217 comprising 80.8% of the region’s population. Household income in the Hawke’s Bay is 83% of the New Zealand average and 22 000 people live in poverty.15
Clinical information systems
HBDHB uses ‘CareInsight’, a stand-alone web-based clinical information system that enables ED clinicians to connect directly to all general practice and after-hours care provider records within the HBDHB region. Once a presenting patient has been allocated a triage category,16 an ED clinician (doctor or nurse) then makes the decision to access the patient’s primary care records after gaining patient consent.
Access to primary care records takes less than a minute, yielding a problem-oriented record with primary care history including all prescriptions, pathology and radiology results, as well as summaries of inpatient and outpatient hospital visits and specialist reports.
Primary care records
Primary care records were available electronically for 97.5% of the local population (97.9% for Māori and 90.9% for Pasifika).17 The information available to ED clinicians from the primary care record is largely that seen by general practitioners (GPs) and includes recent history, problem list, medications, pathology and radiology test results, specialist letters and hospital discharge summaries. ED physicians use a patient’s National Health Identifier number to obtain a list all of the GP or after-hours clinic visits a patient has made within the previous 6 months and can then view each visit’s data. The record lookup system requires an ED clinician to confirm patient consent or to give a short written explanation of why obtaining consent was not possible.
Measures
We analysed each patient’s presenting condition, age, triage category, socioeconomic status (New Zealand Deprivation Index),18 gender and ethnicity, and whether there was an admission to hospital as an inpatient or re-presentation to the ED within 1 month of initial ED presentation. The New Zealand Deprivation Index is a measure of socioeconomic deprivation on a scale from 1 (least deprived) to 10 (most deprived) and is determined by the patient’s address.
Statistical methods
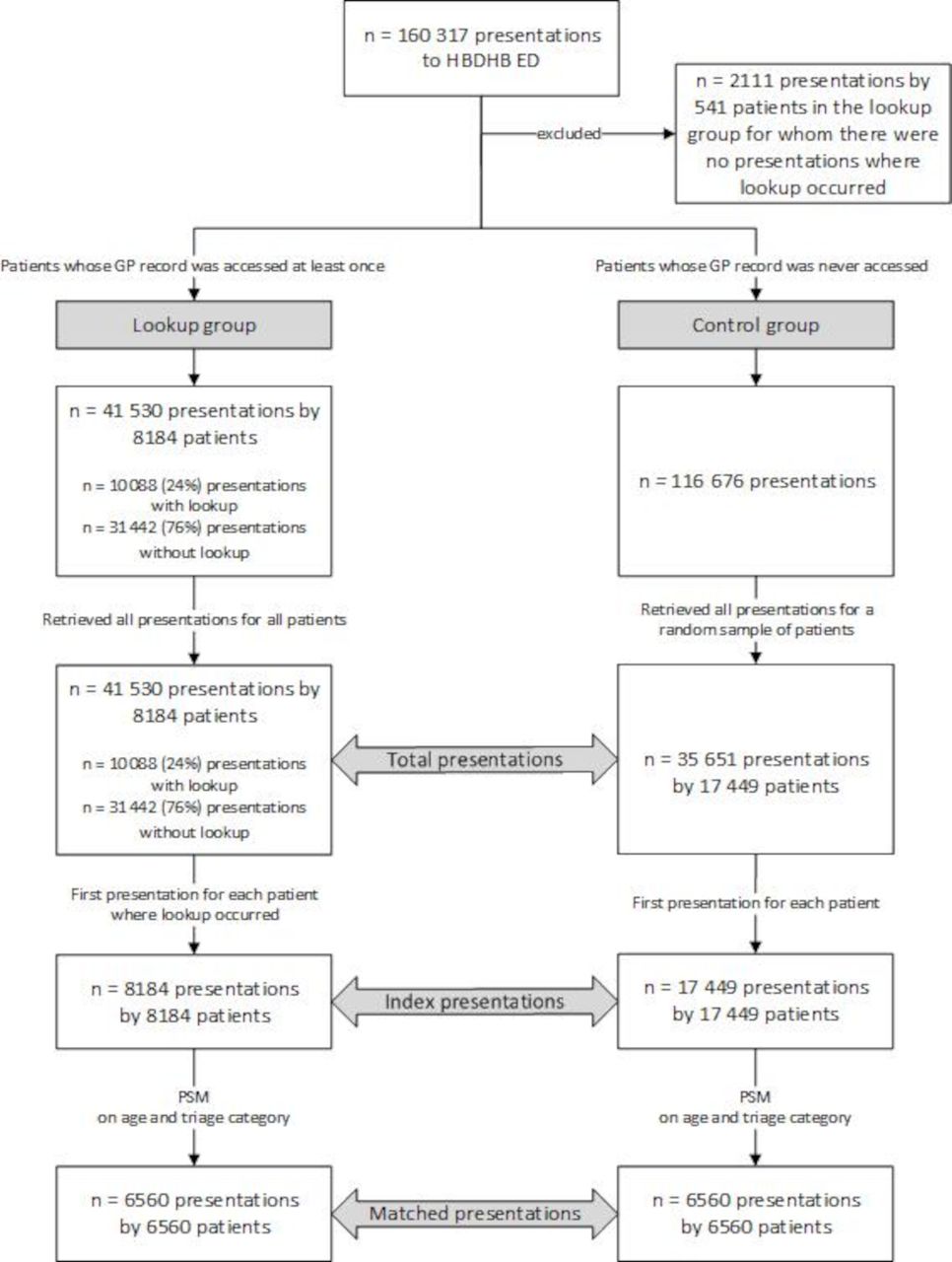
Data were extracted from the HBDHB’s ED management system for all patients presenting over 4 years and 9 months from 1 July 2011 to 31 March 2016. A different ED database recorded whether a primary care record was accessed during the ED presentation. Five hundred and forty-one patients who presented 2111 times were identified as ‘lookup’ patients, but no lookup had occurred, and these records were excluded from further analysis. Only the first or ‘index presentation’ for each patient was used for analysis to avoid clustering effects from some patients presenting multiple times. Primary care records were accessed 10 088 times, including 8184 index ED presentations for the lookup patients. A randomly selected control (or non-lookup) group of 35 652 ED presentations from 17 449 patients (approximately double the number of patients as the lookup group) was created from a total pool of 116 676 ED presentations where no primary care record lookup occurred. Among these controls, 17 449 were index presentations (see figure 1). The deprivation index was not recorded for 298 of the index presentations and these cases were excluded from any analyses that used the deprivation index.

Data selection process for lookup and control groups showing three levels of presentation: total, index and matched. ED, emergency department; HBDHB, Hawke’s Bay District Health Board; PSM,propensity score matching.
Statistical analysis was undertaken using IBM SPSS Statistics V.25. To determine if there were any differences in patient characteristics between lookup and non-lookup patients, χ2 tests were undertaken for gender, ethnicity and presenting conditions. Mann-Whitney U non-parametric tests were used for the ordinal and continuous variables of deprivation index, triage category and age.
To determine whether there was a relationship between lookup and admission or lookup and re-presentation to the ED, propensity score matching (PSM) was used to create matched pairs, correcting for age and triage category.
We undertook sampling without replacement with a 1:1 matching ratio (lookup:non-lookup) to preserve independence of observations. Calliper matching was used, with a maximum calliper distance of 0.001. In all, 6560 lookup and control patients were matched (see matched presentations in figure 1). One thousand six hundred and twenty-four lookup patients could not be matched because no similar non-lookup patient could be found using the propensity score. Non-matched presentations were excluded from further analysis.
To understand which presenting conditions were more likely to be looked up, we calculated relative risk ratios for each presentation condition compared with all other conditions.
Results
There were 25 633 patients in the analysis who made a total of 77 181 presentations. Eight thousand one hundred and eighty-four of these patients (31.9%) had their primary care record accessed at least once and presented a total of 41 530 times to ED (53.8% of the presentations). Median number of presentations were higher for patients who had a primary care record lookup (median 3 presentations, IQR 2–6) compared with the control group (median 1, IQR 1–2; Mann-Whitney U: z=−65.035, p<0.001, r=0.4).
Primary care records were accessed in 6.3% of all presentations; of these, 83.1% (n=6800) were for patients who were looked up once, 12.8% (n=1048) were for patients looked up twice and 16.9% (n=336) were for patients who were looked up between 3 and 11 times.
Total ED presentations grew from 31 000 in 2012 to 35 500 in 2015, a change of 12.9% over the 4 full years of the study (figure 2). In comparison, the primary care record lookup rate was 899 in 2012 (4.9%) and 3081 in 2015 (8.3%). Primary care records were looked up for 10 088 ED presentations over the 4 years and 9 months period of the study, including 8184 index presentations. The 35 652 control presentations included 17 449 index presentations. Lookup patients were on average 25 years older than control patients with a median age for lookup patients of 65 (IQR 47–78) compared with 32 (IQR 14–55) for control patients, with a medium effect size (z=−69.180, p<0.001, r=0.43). Overall, 53.4% of lookup patients were female compared with 48.6% of control patients (table 1). While the gender differences were significant, the effect size was negligible (χ2 (1, n=25 633)=51.671, p<0.001, phi=0.045). The New Zealand Deprivation Index groups patients according to their socioeconomic status, irrespective of ethnicity. The deprivation index for control group patients was not significantly different from the lookup group (n=25 335): z=−1.767, p=0.077.
Differences in demographic and triage category variables between control and lookup groups
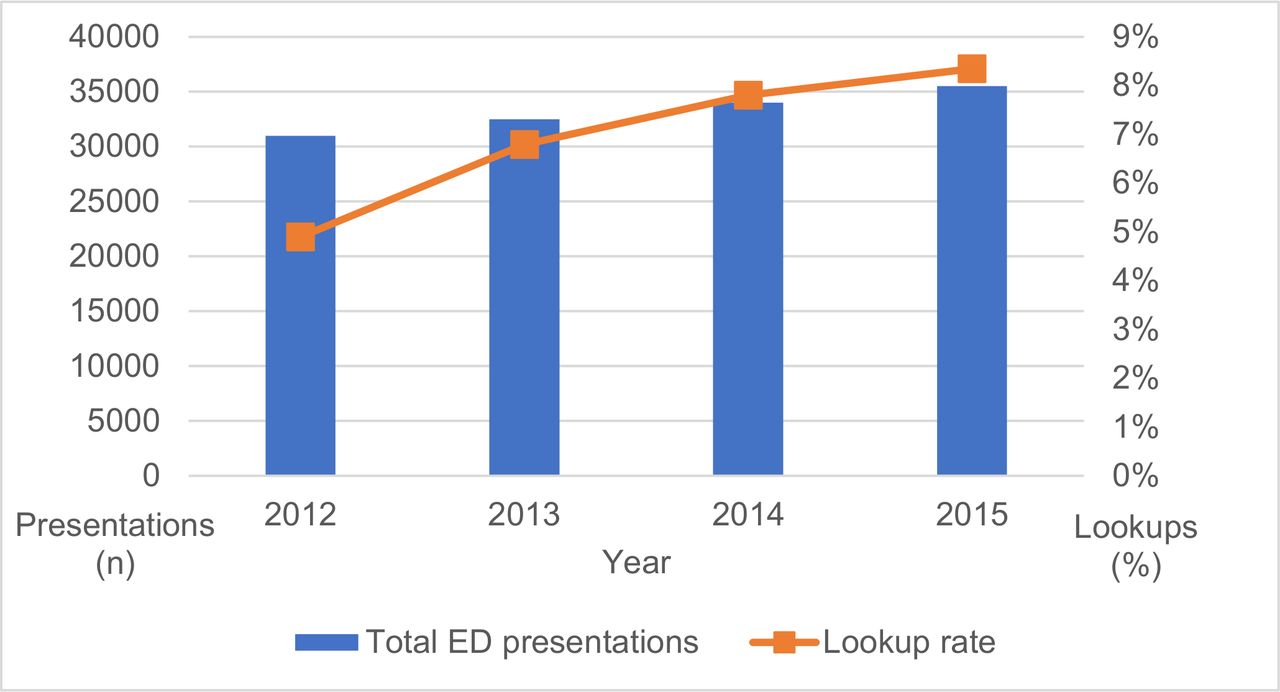
Lookups as a proportion of emergency department (ED) presentations (full years only to remove any seasonal effects introduced by use of partial years).
Māori and Pasifika patients were looked up less frequently than other patients (Māori, 22.4% lookup, 29.3% control; Pasifika, 3.5% lookup, 5.2% control). The relationship between ethnicity and lookup was significant, with Māori and Pasifika patients looked up less frequently, but the effect size was negligible: χ2 (2, n=25 633)=192.775, p<0.001, phi=0.087.
Patients in the lookup group were allocated to a more urgent triage category (figure 3) compared with the non-lookup group, indicating greater severity of problems (table 1; z=−36.47, p<0.001, r=0.23). The median triage category of the lookup group was 3 (urgent), IQR 4 (semiurgent) to 2 (emergency). The median triage category for the control group was 4 (semiurgent), IQR 4 (semiurgent) to 3 (urgent).

{kind=link}
{kind=link}
{kind=link}
Distribution of triage categories among index visit patients with and without primary care record access. Resus, resuscitation.
There was a significant difference in the proportion of patients looked up for different presenting conditions (χ2 (39, n=25 593)=2583.5, p<0.001, phi=0.32). The presenting conditions with the highest relative risk ratios (lookup vs control) for lookup were confusion, collapse fall, cardiac arrest, seizure postictal, medical other, heart palpitations and chest pain (table 2). The five presenting conditions with the lowest relative risk were injury upper limb, eye problem, multiple injuries, head injury and injury lower limb (table 2).
Differences in presenting condition variables between control and lookup groups ranked by relative risk ratio
A further group of presenting conditions notable for their lower than expected lookup rates was a group of specialised presentations in areas such as ophthalmology, dental, paediatric issues and early pregnancy problems.
Patients who were looked up were significantly and meaningfully (ie, had an effect size of small or greater) different from those who were not, in two characteristics: they were older and presented with more urgent triage categories. Consequently, we sought to control for the effect of age and triage using PSM to develop a better understanding of how lookup impacted dispositional outcomes.
Disposition outcomes were different between the matched lookup and control groups, but effect sizes for these differences were less than small. Compared with 56.5% of the control group, 64.6% of the lookup group were admitted to hospital (χ2 (1, n=13 120)=98.385, p<0.001, phi=0.087). Compared with 12.1% of the control group, 18.6% of the lookup group re-presented to ED within 30 days (χ2 (1, n=13 120)=86.288, p<0.001, phi=0.081).
Discussion
This study of primary care records in an ED demonstrates that such records are routinely used, that their usage is growing with time and that usage patterns suggest specific circumstances and patient groups where such records may be of specific value.
We undertook a study to measure the rate of PMH access in a New Zealand emergency care setting, the attributes of patients for whom records were accessed and sought to assess the association between record access and patient disposition after presentation to the ED. We found that primary care records were accessed in 6.3% of all presentations, with the majority (83.1%) of these being for patients who were only looked up once. Record access rates were higher for older patients and slightly lower than expected for Māori and Pasifika in this population. No difference was seen based on socioeconomic status. The group of patients whose primary care records were looked up during one or more ED presentations (31.9% of patients) accounted for a disproportionately large number of overall ED presentations (53.8%), making them greater consumers of ED services than control group patients.
Records were accessed at more than double the expected rate for the highest two triage categories and well below the expected rate for semiurgent and non-urgent cases. The five presenting conditions with the highest lookup rate (confusion, collapse/fall, cardiac arrest, seizure postictal and medical other) had a high triage category. This suggests that ED clinicians may have specific information needs that make it worthwhile searching primary care records for these patients. The five presenting conditions with the lowest lookup rate were associated with trauma (injury upper limb, eye problem, multiple injuries, head injury, injury lower limb), suggesting primary care records had less to offer when historical data had little influence on immediate management.
This study also revealed significant differences with less than small effect sizes in the disposition outcomes of patients matched for age and triage category depending on whether a primary care record was accessed. Patients with a primary care record access were more likely to be admitted to hospital (64.6% vs 56.5%) and more likely re-present to ED within 30 days (18.6% vs 12.1%). Research on the relationship between triage category and hospitalisation rates for older patients is inconclusive. Age alone may play a significant role in explaining higher hospitalisation rates among the elderly.21 More generally, this study was unable to look at downstream patient outcomes such as morbidity and mortality. It was also unable to study other events that might change because of information contained in a primary care record such as medication errors, prescription and investigation rates. Several recent US studies have suggested that accessing PMH from the ED can reduce service utilisation for some patient groups and thus yield cost savings.7–10 22 Consequently, future studies of SEHR access are needed to determine if there is any impact on clinical outcomes and process outcomes such as pathology and radiology service utilisation.
Use of the primary care record lookup capability was not mandated at the study site. Consequently, this study provides a useful perspective on patient characteristics and presenting conditions associated with emergency clinicians’ decisions to access primary care records. Many reasons may influence a clinician to access a record system, including perceived clinical need, usability of the system, expectation that useful information will be found and awareness of the existence of the system.8 22–24 As this study did not focus on such technology acceptance and utilisation factors, we are unable to say whether the observed rates of usage of the primary care system in the studied ED would be representative of rates in other regions in New Zealand or indeed in other countries.
The key implication for policy and practice is that clinicians are accessing primary care records in ED for specific types of patient, namely, those who are older or have a greater acuity of illness. Consequently, rather than creating general purpose shared records, it may make more sense to focus on the information needs associated with managing such patients and crafting a more targeted set of patient data and data access methods.
Limitations
While this study covers 4 years and 9 months of hospital data for 77 181 ED presentations, it is observational and retrospective. Observed event frequencies may be influenced by variables not available in the dataset, and such confounding may bias these frequencies in a way that hides their true underlying rates. Matching was based on observed differences between lookup and control patients. Accordingly, we used PSM to control for triage category and age. However, the possibility of unmeasured confounders cannot be excluded.
The causal relationship (if any) between primary care record access and hospital admission or re-presentation cannot be unpacked using the data from this study. For example, we cannot say whether record access increased the likelihood of admission because it supplied new data triggering admission or simply whether those conditions for which admission is more likely had increased information needs, which triggered a record access.
Another potential source of bias was that the ED data did not record whether unsuccessful lookups occurred when no primary care record was available. It is therefore possible that some patients in the control group should have been in the lookup group. However, such patients are likely in the minority as 97.5% of patients in the region had a general practice held electronic patient record and all of these records were accessible 24 hours a day. We did not collect data in this study to identify which parts of the primary care record were the focus of any given access.
Conclusion
Having access to primary care records appears to be a capability that ED clinicians find useful in emergency situations. Emergency care clinicians will access primary care records if they are available and appear to do so more frequently for patients who are older or are in higher triage categories. The majority of patients who are looked up only have their primary care record accessed once. As primary care records appear to be frequently accessed in emergency settings and thus seem of value to clinicians, further studies should focus on making the information held by primary care providers more useful to external parties; in particular, making the specific information needed easier to obtain and utilise within the external parties’ own electronic medical record systems.
Acknowledgments
The authors are grateful to the staff of the HBDHB, in particular, Dr Mark Barlow, Head of the Emergency Department, Sandy Brown, Head Emergency Department Nurse, Ann Speden, Chief Information Officer and Darren Thompson, Information Analyst. They are also grateful to statistician Craig McKinley who introduced them to the technique of PSM.
Footnotes
Contributors TCB conceived this research and designed and conducted the study with guidance from and under the supervision of EC and DL. TCB drafted the manuscript with input from all authors. All authors provided revisions for intellectual content. All authors have read and approved the final manuscript. All three authors contributed a significant amount of effort to this work.
Funding This study was supported by the NHMRC Centre for Research Excellence in eHealth (APP1032664).
Competing interests Until early 2019, TCB was a director and shareholder of HealthLink Ltd, one of the two companies that jointly provide the CareInsight shared electronic health records system to HBDHB. TCB has no current financial interest or connection to HealthLink Ltd.
Patient consent for publication Not required.
Ethics approval The research was conducted in accordance with protocols approved by the Macquarie University Human Research Ethics Committee (Reference number 5201500980) and was given approval by HBDHB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. We will provide anonymised data if requested to do so by a reputable organisation.