Article Text

Abstract
Background Person-generated health data (PGHD) are produced by people when they use health information technologies. People who use PGHD may experience changes in their health and care process, such as engagement with their own healthcare, and their sense of social support and connectedness. Research into evaluating those reported effects has not kept up; thus, a method for measuring PGHD outcomes was previously designed and applied to the exemplar case of Kinect-based stroke rehabilitation systems. A key step of the method ensures that the patient’s voice is included. Allowing stroke survivors to participate in the development and evaluation of health services and treatment can inform healthcare providers on decisions about stroke care, and thereby improve health outcomes.
Objective This paper presents the perspectives of stroke survivors and clinicians on the anticipated effects of stroke survivors’ use of PGHD from a poststroke simulated rehabilitation technology.
Methods This study gathered the perspectives of stroke survivors and clinicians through three focus groups and three interviews, recruited for convenience. Participants were also asked questions intended to encourage them to comment on the initial items of the patient-reported outcome measure-PGHD. Deductive thematic analysis was performed.
Results This paper has further demonstrated that outcomes of using PGHD can be measured. For instance, stroke survivors described that using PGHD could result in positive, negative and nil effects on their health behaviours. Survivors and clinicians had varying perspectives in three of the six themes presented, and emphasise the importance of allowing stroke survivors to participate in the evaluation of digital health services.
- BMJ health informatics
- health care
- patient care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
What is already known?
Measuring health outcomes resulting from patients' use of their person-generated health data (PGHD) through patient-reported outcome measures (PROMs) could provide a standardised approach to evaluating and improving health information technologies.
A PROM-PGHD Development Method was previously demonstrated for the case study of a type of stroke rehabilitation systems, resulting in a preliminary item bank of PROM-PGHD.
Allowing stroke survivors to participate in the development and evaluation of health services and treatment can inform healthcare providers on decisions about stroke care, and thereby improve health outcomes.
What does this paper add?
To improve the preliminary item bank, this paper gathered perspectives of stroke survivors and clinicians on the anticipated effects on stroke survivors when they use PGHD from a poststroke simulated rehabilitation technology.
This paper has further demonstrated that outcomes of using PGHD can be measured. For instance, stroke survivors described that using PGHD could result in positive, negative and nil effects on their health behaviours.
This paper confirmed that patients and clinicians could have varying perspectives about health care, emphasising the necessity of using participatory methods in the design, development and evaluation of health information technologies.
Background
Person-generated health data (PGHD) are produced by people when they use health information technologies (HITs) such as activity tracking devices and applications, and simulated rehabilitation technologies, to monitor their health outside of a clinical setting. People may also record and analyse their PGHD for themselves, which includes wellness and other biometric data.1–3 It has been reported that people who use PGHD have changes in their engagement with their own healthcare, their relationship with their healthcare providers and their sense of social support and connectedness.4–11 Thus, PGHD utilisation promotes participatory health.
Research into evaluating those reported effects, however, has not kept up,1 2 12 and there is a need for a systematic way of measuring health outcomes for people who access and use their PGHD.1 13 14 In response, a method for developing patient-reported outcome measures (PROMs) using PGHD, called the PROM-PGHD Development Method, was designed by the authors.15 16 Using PROMs has also been suggested as a way to standardise the measurement of PGHD outcomes and strengthen the empirical evidence around PGHD.3
PROMs allow people to self-report their health status or experience with an illness or treatment, without the need for additional clinician interpretation of the report.17–19 A patient-reported outcome may indicate status at a single point of time, or be compared with previous patient-reported outcomes to show changes over time.17 20 PROMs enable patients to participate in improving the evidence base of a variety of HITs, as patients contribute to more precise evaluation of the effects of those technologies.21 The value of using PROMs to standardise evaluation of health status for increased quality of healthcare provision is marked by key projects around the world.22 23
Similar to how PROMs may be used in conjunction with other health indicators,22 PROMs-PGHD can complement existing patient-reported or clinician-reported outcomes of interventions or monitoring plans involving HITs. PROMs-PGHD can measure health outcomes or status as a result of people accessing, using and reporting their own PGHD. This would allow people to participate in evaluation of HITs, and the effects of using health data they generate themselves.15
The PROM-PGHD Development Method was applied to the exemplar case of Kinect-based stroke rehabilitation systems (K-SRS).15 The complexity of care involved in stroke, and its high global burden make it an important area for implementing rehabilitation systems.24 25 Barriers to access and availability, such as cost and distance, necessitate more convenient and practical rehabilitation options for stroke survivors.26 Simulated rehabilitation technologies such as K-SRS offer stroke survivors an alternative, effective option to perform simulated activities of daily living (ADL).27 Moreover, they allow for a more consistent and semicontrolled process of monitoring and evaluating survivors’ therapeutic progress.27 28 For instance, U.S. Food and Drug Administration (FDA) approved Jintronix provides users with games that simulate clinical exercises,29 30 and produces PGHD.2 Benefits of such systems to stroke therapy have been reported.27 28 31 32 Therefore, measuring PGHD outcomes in K-SRS is an important use case.2
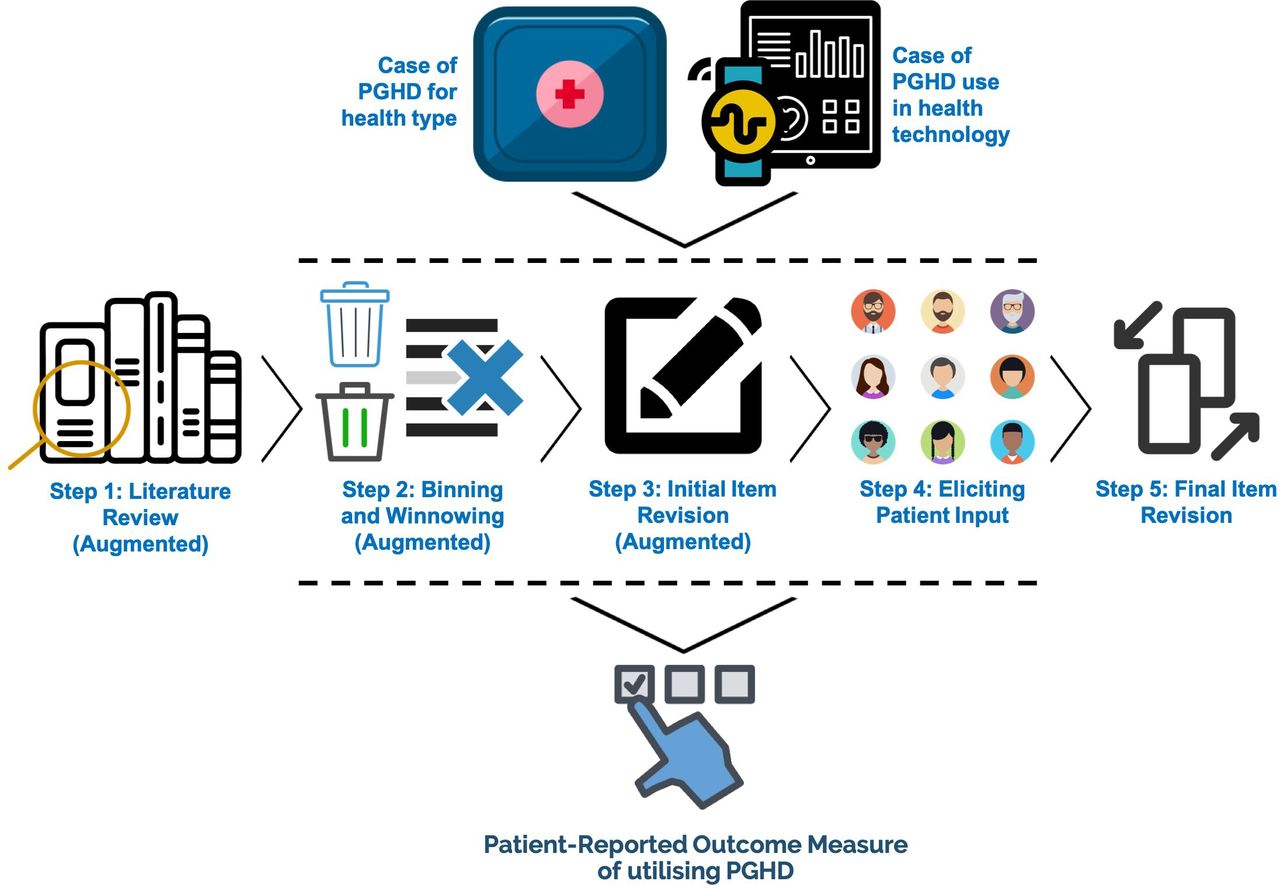
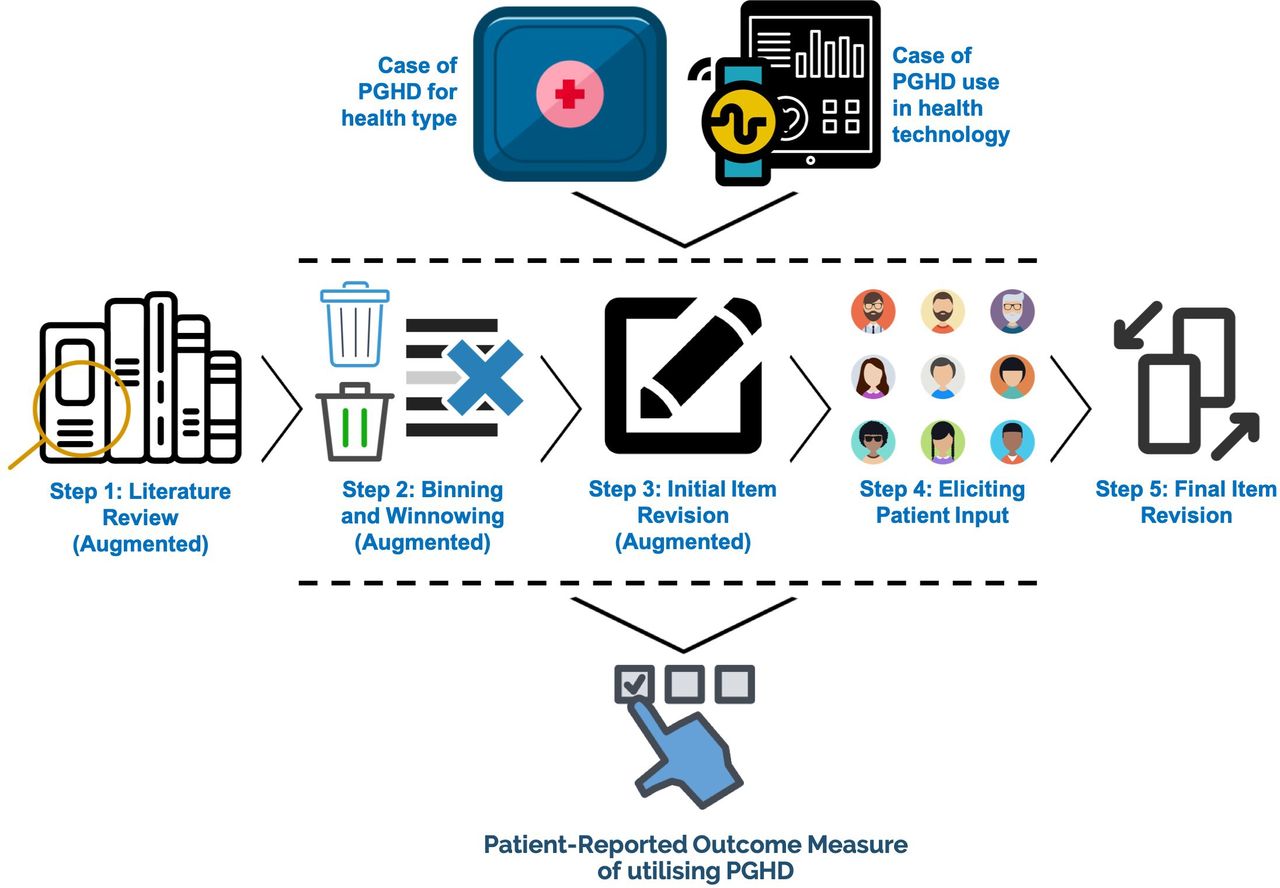
A key step of the PROM-PGHD Development Method ensures that the patient’s voice is included through focus groups and/or semistructured interviews.15 This allows the target cohort to provide feedback on the initial items of the PROM-PGHD. It also allows developers to understand the thinking processes and vocabulary of the target cohort, and to identify any measurement areas that are not covered by the PROM-PGHD’s initial item bank. This would bridge current gaps between the initial items and the target domain to be measured.15 For reference, the PROM-PGHD Development Method is illustrated in figure 1 (previously published in Ref. 16).
{kind=link}
The steps of the patient-reported outcome measure using person-generated health data (PROM-PGHD) development method. This figure illustrates the process followed in developing a PROM-PGHD. This was previously published in Ref.16
Allowing stroke survivors to participate in the development and evaluation of health services and treatment has been shown to inform healthcare providers on decisions about stroke care, and thereby improve health outcomes.33 In particular, qualitative activities such as focus groups and interviews can be valuable in revealing aspects of stroke survivors’ healthcare and rehabilitation process that is most important to them, such as types of therapy they think are most effective33 and factors that will help motivate them to perform therapeutic exercises over the long term.34 Additionally, stroke survivors may also provide direct insights into considerations that would enable a stroke self-management programme to be effective,35 such as their readiness, support and collaborations needed for them to successfully self-manage their care.36 This also includes stroke survivors’ complex, changing nature of self-management where their carers could be either encouraging or constraining37; the influence of interpersonal care practices on their overall recovery38; and primary rehabilitation outcomes they want to achieve.33
Eliciting the input of stroke survivors is particularly important because there could be differences in their perspectives and that of their care providers, regarding treatment and management. For instance, differences in stroke survivors and their therapists’ understanding of self-management and accompanying barriers could result in conflicting expectations of the role that patients and their therapists have of each other. This could undermine the success of self-management strategies.39 Desired health outcomes from physical activities such as structured exercises and ADL could also differ between stroke survivors and those of health professionals involved in their rehabilitation. While the former may value the outcome of participation in personally meaningful activities, resulting in a continued sense of self-poststroke, clinicians may value the outcome of functional or physical movement which may not be as personally meaningful for the stroke survivors.40 These differences may also present challenges to the design and evaluation of HITs that produce PGHD. For example, a ‘tension’ between the needs and preferences of patients with surgical site infections and their care providers has been documented, and has implications for the design and implementation of a web-based wound management application that produce PGHD.8
Objective
This paper presents the perspectives of stroke survivors and clinicians on the anticipated effects of stroke survivors’ use of PGHD from a poststroke simulated rehabilitation technology.
Methods
As part of the PROM-PGHD development method, focus groups were conducted with stroke survivors and clinicians, or semistructured interviews for those who could not agree on a similar day or time with others.
This study was conducted as part of a larger research project, in order to refine the preliminary item bank of a PROM-PGHD.15 16 Other activities to develop the PROM-PGHD are reported elsewhere, including in Refs. 2 13 15. Earlier discussions with a different cohort of stroke survivors13 are discussed briefly in the Results section to show parallels and variety of how PGHD may affect health outcomes.
The presentation of this paper was largely guided by recommendations for qualitative research in eHealth.41 The procedure for conducting the discussions is outlined in online supplementary appendix 1.
Supplemental material
Setting
Participants were recruited from two sites in Australia: Headway ABI in Queensland and a large metropolitan hospital in Melbourne, Victoria. Headway ABI is a not-for-profit outpatient clinic providing rehabilitation services to people who have an acquired brain injury. Their clients usually come from the cities of Brisbane and Gold Coast. The metropolitan Melbourne hospital is a tertiary and quaternary health service, and specialises in areas such as cancer, infectious diseases and rehabilitation.
As far as the authors know, Headway ABI is the only health and fitness centre in Australia where Jintronix-simulated rehabilitation services are available to stroke survivors. Thus, participants recruited through Headway would be the only ones in Australia who would have voluntarily opted to use Jintronix as part of their ongoing therapy.
Participants
The researchers aimed to include two groups: stroke survivors themselves, and physiotherapists who had experience of working with such clients. At Headway ABI, only one client was available to be recruited. We aimed to also include staff but this did not occur because of their limited availability.
Headway ABI
Eligible stroke survivors were adults who used Jintronix, an FDA-approved,29 30 simulated rehabilitation system using a leading body-tracking technology, Kinect,42 as part of usual outpatient therapy provided by Headway ABI. They were eligible if they had not used any other stroke rehabilitation software, for example, an exercise platform using consumer technology Nintendo Wii,43 were proficient in English, and did not have any mental, visual or verbal medical conditions that may impact their participation. Eligible participants were identified by a staff, who initiated first contact with potential participants, and collected their consent to release contact information to the authors, that is, email, or telephone/mobile number. After receiving the details of eligible participants, GLD contacted the eligible participants to discuss the project, invite them to participate and secure their verbal consent.
Only one stroke survivor (age group 60–64) could be recruited from Headway ABI. The exact age is concealed as per BMJ requirement. The semistructured interview was conducted through a Zoom video call. It had been 5 months since her last stroke, and 4 years since her first.
Melbourne health service
Eligible stroke survivors were adults who underwent usual therapy provided by the Melbourne health service, have not used any other stroke rehabilitation software, were proficient in English and did not have any cognitive, visual or speech impairments that impacted their participation. Eligible participants were identified by a clinician collaborator from the Melbourne health service. The collaborator initiated first contact with potential participants, to gather potential interest. After receiving the contact information of participants, GLD and FB contacted the eligible participants to discuss the project, and invite them to participate. Eligible physiotherapists were those who provided therapeutic services to stroke survivors, and had not used any other stroke rehabilitation software.
All participant focus groups and interviews were conducted at a rehabilitation campus of the Melbourne health service. Five clinicians were able to participate in a focus group, conducted in January 2019. The most experienced clinician had 37 years of experience, with 35 of those working with stroke survivors. The least experienced had 2 years, with 1 year working with stroke survivors. Table 1 presents each clinician’s number of years working as a physiotherapist, and with stroke survivors. Meanwhile, four stroke survivors were able to participate in two separate focus groups; and another two stroke survivors participated in semistructured interviews. All focus groups and interviews with stroke survivors occurred in April and May 2019. The oldest was within the age group of 75–79 years old, and it was 11.5 years since their first stroke. The youngest was within the age group of 55–59 years old, and it was 2 years since their first stroke. Table 1 shows each survivor’s age groups and number of years since their first stroke. Their exact ages are concealed as per BMJ requirement.
Clinicians’ length of experience, and stroke survivors’ age groups and years since stroke
Data analysis
Approximately 7 hours comprising three focus groups and three interviews were transcribed verbatim by GLD. All transcriptions were rechecked for accuracy, and deidentified. The transcriptions, data management and coding were conducted using NVivo V.11 (QSR International Pty, Melbourne, Australia).
Deductive thematic analysis was initially conducted independently by GLD, KG and MM on a selection of transcripts. Themes were previously derived deductively from the identified PGHD effects from the literature.15 Once common understanding was achieved for how themes are applied, GLD proceeded to analyse the rest of the transcripts. GLD initially listened through the recordings again, while simultaneously reading through the transcripts in order to familiarise himself with them. Throughout this process, codes were initially applied to texts, where relevant. Afterwards, GLD proceeded to go through the transcripts again to apply codes, and double check the initial codes applied. A coding journal was used to clarify contentious quotes with KG and MM. Afterwards, all coded transcripts were independently checked by KG and MM. Any disagreements with the codes applied were discussed over two coding meetings, and subsequently resolved.
Additional information on conducting the discussions is outlined in online supplementary appendix 1.
Results
The results are summarised and categorised below as subheadings according to the different themes.15 Throughout the coding process, however, a sixth theme on relationship with family and carers emerged and is presented below.
As earlier discussed, stroke survivors’ perspectives on health-related aspects could be different from those of care providers, which might produce tensions8 that could undermine the success of self-management strategies39 and the technologies that support them.8 Therefore, any variations in the perspectives of stroke survivors and the clinicians are also important, and described briefly.
To see more description of the health effects including example quotes, see online supplementary appendix 2.
Supplemental material
Health-related behaviours
This section summarises the different effects that PGHD utilisation may have on health-related behaviours of stroke survivors, which were raised during the discussions (table 2). It also briefly discusses how the perspectives of stroke survivors and clinicians are similar. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on health-related behaviours of stroke survivors
Similar perspectives
Stroke survivors and clinicians recruited through the Melbourne hospital health service reported positive and negative potential effects of PGHD use on their health behaviours. Additionally, survivors described neutral potential effects of PGHD on their health behaviours. The stroke survivor from Headway (‘Site 2 survivor’) did not have any comment relevant to the theme.
Feelings about health status
This section summarises the different effects that PGHD utilisation may have on stroke survivors’ feelings about their health status, that were raised during the discussions (table 3). It also briefly discusses how the perspectives of stroke survivors and clinicians are similar. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on stroke survivors’ feelings about their health status
Similar perspectives
Participants reported that using PGHD could result in positive, negative and neutral effects on survivors’ feelings about their health status. These feelings were differentiated from the previous theme because they did not specifically describe actions that indicate changes in behaviour, that is, undergoing more exercises, or changing movement actions to improve performance.
New theme: relationship with family and carer/s
This section summarises the different effects that PGHD utilisation may have on stroke survivors’ relationship with their family and carer/s, that were raised during the discussions (table 4). It also briefly discusses how the perspectives of stroke survivors and clinicians are similar. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on stroke survivors’ relationship with family and carer/s
Similar perspectives
Clinicians and survivors felt that PGHD may generally have positive effects on the relationship of stroke survivors and their family.
Interest in care processes
This section summarises the different effects that PGHD utilisation may have on stroke survivors’ interest in their care processes, which were raised during the discussions (table 5). It also briefly discusses how the perspectives of stroke survivors and clinicians vary. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on stroke survivors’ interest in their care processes
Varying perspectives
While clinicians largely discussed how PGHD could potentially increase stroke survivors’ interest in how their exercises contributed to their therapy progress, survivors also discussed their interest in knowing their recovery progress for self-management of energy, and in improving their movement and performance. All participant groups described interest about the care or system processes, as a result of seeing PGHD.
Personal care goals
This section summarises the different effects that PGHD utilisation may have on stroke survivors’ personal care goals, which were raised during the discussions (table 6). It also briefly discusses how the perspectives of stroke survivors and clinicians vary. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on stroke survivors’ personal care goals
Varying perspectives
All participants described how PGHD could potentially motivate stroke survivors to improve their therapy performance, although one clinician perceived otherwise. Additionally, a survivor felt that PGHD might help them form new goals, although a clinician disagreed.
Relationship with care provider/s
This section summarises the different effects that PGHD utilisation may have on stroke survivors’ relationship with their care provider/s, which were raised during the discussions (table 7). It also briefly discusses how the perspectives of stroke survivors and clinicians vary. To see more description of the health effects including example quotes, see online supplementary appendix 2.
Discussed person-generated health data (PGHD) utilisation effects on stroke survivors’ relationship with their care provider/s
Varying perspectives
Clinicians and stroke survivors agreed that PGHD could potentially prompt survivors to contact their therapists to ask what they could do better. However, while clinicians shared that PGHD will need to be discussed with survivors to help them understand, survivors stressed that they would want to see their PGHD regardless, and may even be prompted to ask their therapists what happens to the PGHD they produce. Additionally, some survivors may be prompted to ask what their therapists are doing incorrectly with regards to the treatment they receive, and whether their therapists are happy with their progress.
Discussion
This study is the first to gather and compare the perspectives of stroke survivors and clinicians, in order to develop a PROM-PGHD for a simulated rehabilitation system. The perceived PGHD potential outcomes described by site 1 survivors who received a demonstration of Jintronix were mostly similar to those reported by the site 2 survivor, who has used Jintronix in a real-life, voluntary, outpatient setting. Moreover, as earlier described, this paper is part of a larger study, and there were significant parallels to the results of this study to the experiences of stroke survivors who have used Jintronix for 8 weeks in a Randomised Controlled Trial, reported previously.13 This indicates that the technology demonstration provided to the site 1 cohort, coupled with their lived experience with stroke, was a valuable way of gathering perspectives about the potential effects of PGHD utilisation.
Stroke survivors and clinicians had varying perspectives in three of the six themes presented. This puts emphasis on the importance of allowing stroke survivors to participate in the evaluation of digital health services. Consideration of how their perspectives differ with that of clinicians has relevance to the success of patient self-management strategies,39 and to the design and evaluation of PGHD technologies.8 44
The findings show that stroke survivors are interested in their PGHD to better self-manage their energy during therapy, something that clinicians did not raise in the discussions. Moreover, while clinicians expect survivors to contact them in order to understand how their PGHD relates to their therapy, survivors would prefer to have the opportunity to understand it for themselves. Stroke survivors would prefer to have access to all of their PGHD, so that their therapy process is open and transparent. This highlights the differences that patients and clinicians could have in their understanding of self-management strategies, which could lead to conflicting expectations in the roles that patients and their clinicians have of each other.39
Interestingly, while it has been suggested that clinicians valued functional or physical movement outcomes more than patient gains in ADL,40 the clinicians we spoke to understood that survivors personally valued how their therapy contributed to an improved performance of ADL. As such, they seek to tailor their therapy based on the ADL goals of their clients. This indicates that while patients and clinicians may indeed have varying perspectives,39 the potential for tensions to occur between the needs and preferences of patients and their care providers8 could be reduced through a similar understanding of health treatment goals.
This paper has further demonstrated that outcomes of utilising PGHD can be measured.13 For instance, stroke survivors described that using PGHD could result in positive, negative and nil effects on their health behaviours. PGHD use also has the potential to increase feelings of self-awareness about their health. Additionally, the potential for survivors’ interest to change over time from detailed PGHD towards a big picture view, that is, whether they are improving or their treatment needs to change, is indicative of the fact that a ‘one size fits all’ approach to HIT design will not be beneficial.35
The reported PGHD utilisation outcomes would directly inform the development of a PROM-PGHD for K-SRS, of which this paper is a key step.15 16 For example, it might be necessary to remove or revise items that sounded negative, for example, ‘I felt blue or sad’. Such items may evoke negative thoughts or feelings from survivors and may thus pose a risk. Items that asked survivors if they felt sad or pessimistic could be revised to ask, using a scale, to what extent they felt happy or not happy. The process of revising the preliminary PROM-PGHD is step 5 in the development process, and is fully reported elsewhere.
The PGHD utilisation outcomes gathered in this study could also help inform healthcare providers on decisions about stroke care, for example, understanding which health outcomes are personally important for stroke survivors, and how survivors can be motivated to perform their exercises for the long term.33 34 This is particularly relevant in the area of poststroke simulated rehabilitation technologies, where there is a dearth of studies that engage survivors in their own healthcare.2
Limitations
While FB comoderated some of the discussions, most were moderated by GLD. This introduces the risk of eliciting a narrower array of themes and ideas; however, an advantage to this method is that the chance of thematic saturation is increased, as GLD learnt relevant themes as the discussions progressed19; and meant that the moderation of the discussions was consistent.
It should also be noted that in our sample, only the participant from Headway had voluntarily used the case K-SRS in an outpatient setting. However, that person’s perspectives were similar to the site 1 survivors, indicating that the technology demonstration provided to the site 1 cohort, coupled with their lived experience with stroke was a valuable way of gathering perspectives about the potential effects of PGHD utilisation. This highlights the strength of qualitative data collection activities in identifying patient-reported outcomes of a health domain of interest.19 Moreover, our sample, recruited for convenience, and consisting of stroke survivors who had no significant residual visual, verbal or cognitive impairments is not representative, nor was it ever meant to represent all stroke survivors; it was meant to elicit the input of stroke survivors to guide the development of the PROM-PGHD, which will be further refined and validated.23
Conclusion
This paper has described how utilisation of PGHD from a key K-SRS may affect health outcomes of stroke survivors, in the words of survivors themselves and concerned clinicians. It has confirmed that perspectives of patients and clinicians may vary, emphasising the necessity of using participatory methods in the design, development and evaluation of HITs. The findings have direct implications for the development of a PROM-PGHD for K-SRS, which will be further refined and validated.
Acknowledgments
The authors would like to acknowledge the staff of the metropolitan Melbourne health service and Headway ABI. GLD would like to acknowledge the Melbourne School of Engineering through which his research scholarship is provided; and his organisational sponsor, Newman College (University of Melbourne).
References
Footnotes
Twitter @IkeeDee
Contributors GLD contributed to the study planning and design, ethics applications, organisational collaborations, data collection, analysis and interpretation, and writing of the manuscript. FB contributed to the study design, ethics applications, organisational collaborations, data collection, data interpretation and manuscript revision. MM contributed to the study design, ethics applications, data interpretation and manuscript revision. KG contributed to the study design, ethics applications, and manuscript revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Granted through signed consent forms. Recruitment through the Melbourne health service was approved by the relevant Health Human Research Ethics Committee (AU RED HREC: HREC/17/Austin/492). Recruitment of participants through Headway ABI was approved by the University of Melbourne Medicine and Dentistry Human Ethics Sub-Committee (ID: 1852259.1).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.