Article Text

Abstract
Introduction The National Institute for Health and Care Excellence (NICE) plays a central role in the NHS. We distill knowledge of best practice from the best available sources of evidence and share this across the health and care system, typically in the form of recommendations. We want to ensure that this knowledge is shared in a form that supports improved decision making by professionals working together with patients, leading to improved outcomes. Understanding the role of computable knowledge in the context of a learning health system is therefore of deep interest to NICE.
Methods The Agency for Healthcare Research and Quality (AHRQ) 4 levels of knowledge have been used as a framework to review current NICE products and services and envisage how they may need to evolve.
Discussion NICE is mostly still at level 1 of the AHRQ knowledge hierarchy but aspires to work towards structured and computable products. The NHS Long Term Plan makes clear that the wider health and care system is seeking to drive up interoperability with standards for data exchange at the heart of this. NICE Connect is the name given to NICE’s ambition to change in order to keep pace with changing technologies, advances in guideline development and analytical methods and the shifting needs of the system, and to ensure that it can sustainably and efficiently manage its portfolio of guidance. It is seen as crucial that NICE Connect and the wider Mobilising Computable Biomedical Knowledge (MCBK) agenda align for either of them to truly succeed.
- health care
- information management
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
This paper aims to capture a perspective on the Mobilising Computable Biomedical Knowledge (MCBK) movement from the position of the National Institute for Health and Care Excellence (NICE) as a national guideline developer in the UK. The paper captures the views presented by NICE, and subsequent discussion, at the inaugural MCBK UK workshop that took place in October 2019.
NICE is the independent organisation responsible for providing evidence-based guidance on health and social care.1 Internationally renowned for the rigorous and transparent processes and methods employed to develop our guidance, NICE plays an active role in a range of research projects to develop and improve our methodologies.
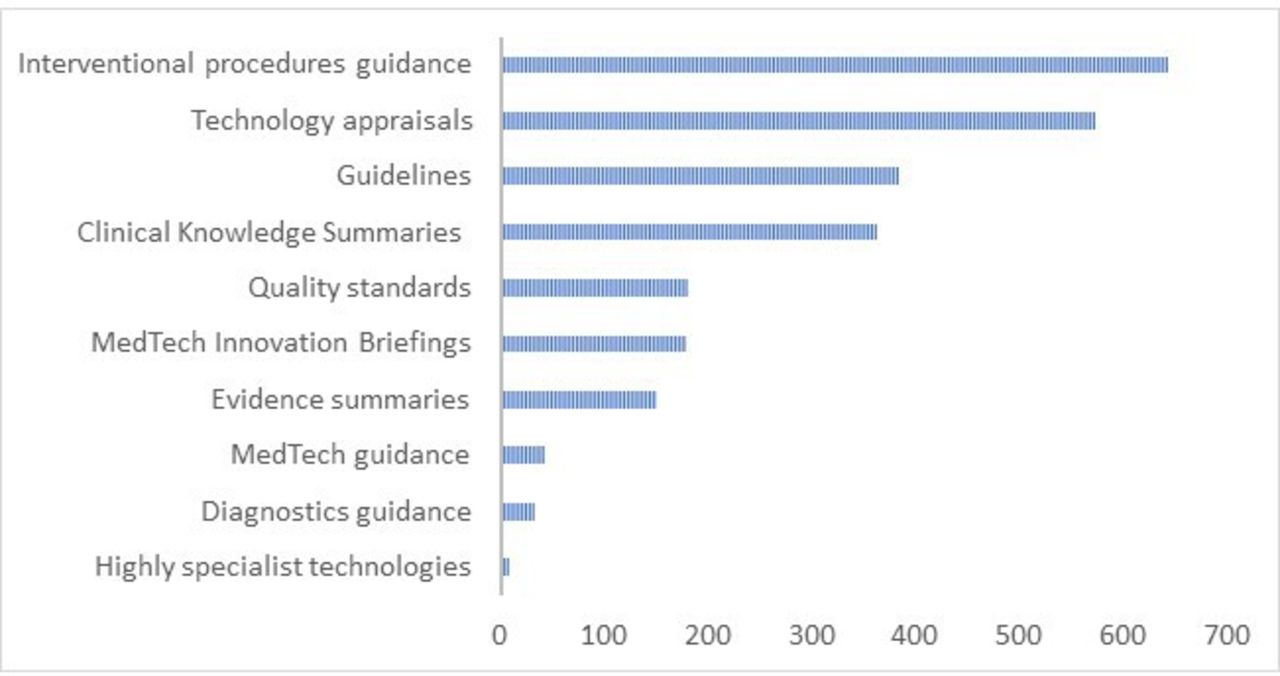
NICE was established 20 years ago and during that time its scope has broadened substantially to encompass clinical, public health and social care guidance—often seeking to bring these areas together in support of joined-up care. Figure 1 provides an overview of the array of different products produced by NICE to date.
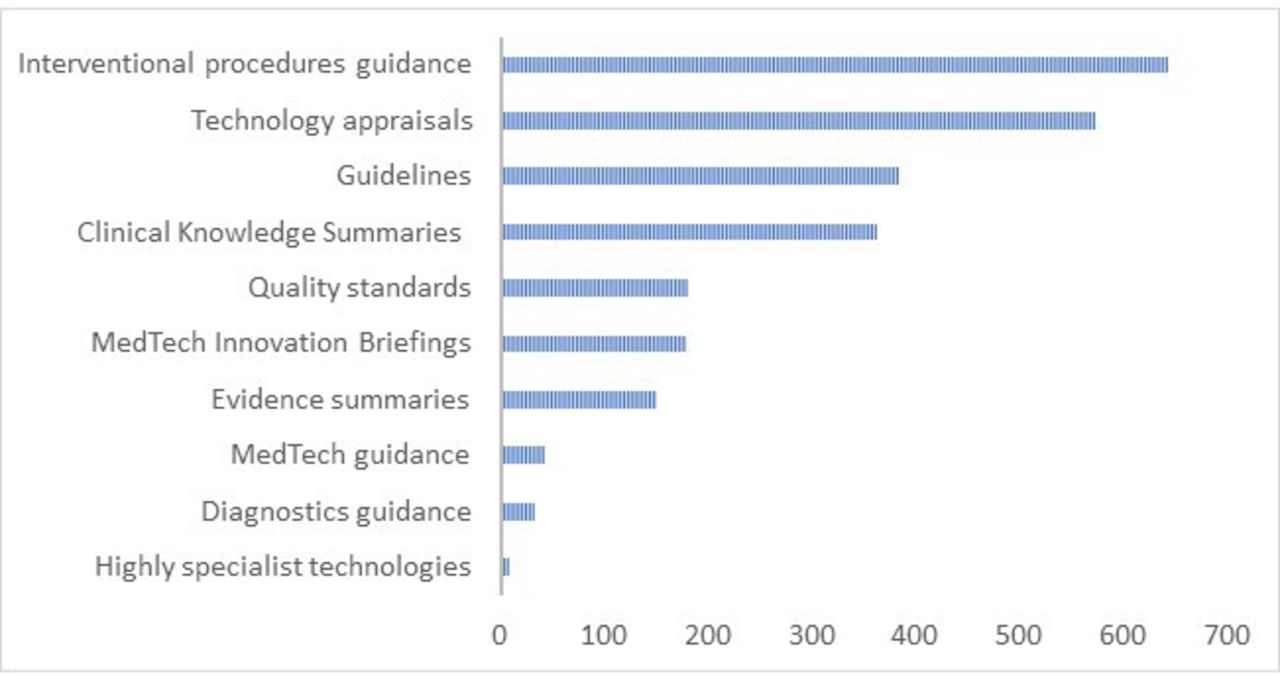
Over 20 years the National Institute for Health and Care Excellence (NICE) has produced over 2550 separate products. Although clinical guidelines represent a significant part of NICE’s corpus they are not the most numerous.
This broad remit places NICE in a unique position when considering the development of knowledge for use within the health and care system. It provides a unique perspective on the shared needs of front-line staff making decisions in these different domains, and enables a greater understanding of the challenges caused by increasing multi-morbidities. There are many different types of evidence that need to be considered when developing actionable recommendations—for example, the kind of evidence and analytical methods used to develop social care recommendations is different to the evidence and methods used when assessing drugs and devices. NICE has a unique perspective on these different methods and how they may need to be modified where computable recommendations are required.
It is worth reflecting on the fact that most decision support and computable knowledge research work conducted outside of NICE to date has focused primarily on clinical decision support, and has built on the long tradition of coding and classifying clinical conditions and developing single-topic-based guidance. NICE is well positioned to broaden the focus of this work away from individual conditions and to consider polypharmacy, multi-morbidities and the wider health and care system.
NICE’s broad portfolio also represents a challenge for computable knowledge research—by not having a narrow clinical focus, as is the case for many organisations developing guidelines, the vocabularies for coding all guidance content and the technical systems developed in the clinical space will not meet all of NICE’s needs. There is no complete solution NICE can adopt or take ‘off the shelf’ and therefore a collection of different tools and approaches will be required to address the challenges created by the breadth of NICE’s work. Having a single organisation that understands these challenges will provide a rich opportunity for driving MCBK research and developments.
Methods
The Agency for Healthcare Research and Quality (AHRQ) 4 levels of knowledge (see figure 2) have been used to consider the current NICE products and services and envisage how they may need to evolve.

{kind=link}
{kind=link}
An interpretation of the four knowledge levels set out by the Agency for Healthcare Research and Quality (AHRQ).6
In addition NICE has previously commissioned work to map at a high level the decision support vendor market, the ways in which they use NICE guidance and their aspirations for improving their ability for consuming guidelines to improve the user experience associated with clinical decision making in the future.
Throughout 2019 NICE has subsequently conducted a number of interviews and workshops to explore the immediate needs and aspirations of several decision support vendors and developers of decision support tools. This has not been an exhaustive study but has enabled NICE to understand and begin to plan further work to meet the needs of decision support system developers.
Discussion
NICE is primarily still at level 1 of the AHRQ knowledge hierarchy, producing much of its content as narrative text that, in computing terms, is unstructured.
However, there are many who believe that guidelines need to be produced in a computable form and many different approaches to this have been explored historically.2 3 NICE does not think it is sustainable to continue producing only narrative guidance. Presenting NICE’s recommendations—and the evidence underpinning them—in a more structured way is vital for NICE to meet the growing challenge of maintaining (surveillance and updating) the knowledge encapsulated in guidelines. In addition, the notion of retrospectively ‘adding structure’ to an unstructured guideline is often inefficient and potentially unsafe. At the point a guideline is written, often a committee will produce algorithms and models to aid the development of recommendations, but these algorithms are not always published in a format that is suitable for users of guidance. If the guidance is then converted to an executable algorithmic form many of the algorithmic steps have to come from the interpretation of the narrative recommendations, effectively reverse engineering back to the algorithms used by the committee. The notion of ‘closing the gap’ between a guideline development committee and those who produce executable guidance, even considering models of ‘co-production’, offers an opportunity to increase efficiency and reduce misinterpretation when creating computable forms of clinical knowledge.
Over its 20 year lifespan NICE has moved from primarily print outputs to primarily digital, via the NICE website and syndication services, demonstrating its ability to keep pace with the opportunities and expectations that come from a changing digital environment. In recent years NICE has been working to increase the level of formal structure applied to its guidance. The focus for much of this time, however, has been on a shift to semi-structured information primarily to support internal content management needs as well as the tagging and restructuring of content to enable alternative presentations of content on NICE’s own website(s).
Through this work NICE has identified that adding structure and standard clinical codes to its guidelines, even to a semi-structured level, has significant methodological implications and an impact on the steps required to develop guidance. This in turn is intrinsically linked with the technologies required to support the development process.
For both internally and externally motivated reasons NICE therefore recognises the importance of adding structure to all of its content at least to level 2 of the AHRQ knowledge levels, and in some areas to levels 3 and 4. However, to do this the processes, methods, technologies and skills used to develop NICE guidance will need to change. This will not happen quickly, but it is essential to start.
The NHS Long Term Plan makes clear that the wider health and care system is seeking to drive up interoperability with standards for data exchange at the heart of this. This improved sharing of data is required to improve decision making and measure improvements to ensure better outcomes. Implicit in this is the need to derive knowledge from data and to also ensure that this knowledge can be shared efficiently and safely across the health and care system.
NICE understands that structured data and structured knowledge are crucial to enable the concepts of a continually learning healthcare system. As a key provider of knowledge, primarily in the form of actionable recommendations, NICE is in a unique position to help shape and drive the adoption of formally structured ways of delivering knowledge to the system and to begin providing knowledge in this way.
Technically there are challenges of agreeing which existing formalisms, coding and information standards for representing clinical knowledge could be used to share knowledge effectively between systems, and where there are gaps, filling these by extending these standards or, if necessary, working to develop entirely new standards. Practically there are questions about who has responsibility for applying codes and interpreting guidance. Who is liable when something goes wrong? Is it the guideline producer, or those who have interpreted restructured and coded a guideline and then delivered that information to the point of decision making, or the decision maker themselves?
Issues of risk and responsibility become still more complex when third party developers of decision support systems are involved in the dissemination of guidance. In simple terms there is agreement from most parties that there are issues of safety and issues of inefficiency in sharing guidelines or recommendations from guideline producer to decision support providers. There is also agreement and much research that demonstrates increased structure and coding are a fundamental part of the solution to these issues.3–5 There is, however, little clarity currently for NICE or others across the system on what levels of structure and coding are actually needed, who would apply this structure, and what certainty there is across the system that this would actually improve uptake of guidance and improve patient outcomes. In short, the business case for NICE and others across the system to invest in fully computable guidelines remains unclear. This makes it very difficult for anyone to move forwards—this stalemate therefore needs to be addressed as a priority. This challenge is not new,3 but opportunities provided by novel technologies, alignment across the system regarding approach and the growing need for action present new opportunities to tackle the problem. NICE is keen to help in this regard as part of its ‘NICE Connect’ programme.
NICE Connect is a multiyear project underway at NICE, to transform how we produce and present our guidance. Launched in response to user feedback and an increasingly large and complex portfolio of guidance and other products, NICE Connect outlines a vision for the future that builds on NICE’s place as an international leader in evidence synthesis, guidance development and technology evaluation. NICE’s offer to the heath and care system will be developed and improved, with advice integrated along care pathways, accessible to users wherever and whenever they need it, and always up to date.
In the future, recommendations will be short, focused and framed within questions that are important to practitioners and the public. Further detail will be accessible through layers of information, including evidence summaries where needed to support shared decision making. The changes will be carefully balanced with the needs and constraints set out by the scientific methods used to analyse and summarise evidence and develop recommendations.
Improvements will also be made to the way in which NICE engages with its stakeholders, streamlining processes for registering an interest in a guidance topic, commenting on draft recommendations, and applying to join a committee.
Ensuring that new forms of evidence and data analytics capability is further developed to enable NICE to plug evidence gaps and work more effectively with sources of unstructured ‘real world’ data will also be core to NICE Connect.
Within NICE there is now clear recognition that content design and service design based on user centred design approaches will help to deliver on the needs of the wider system. Rather than creating many different guidelines and supporting products that overlap and can appear disjointed on NICE’s website, NICE will deliver an improved user experience, enabling users to easily find and act on guidance when and where they need it. Ensuring—where possible and appropriate—that guidelines are available in computable form will be an important part of this.
This ambition from NICE offers a very exciting opportunity when aligned to the MCBK agenda to drive a different kind of structured knowledge across the NHS, to further improve decision making and ultimately to improve outcomes for patients and other users of the system. It is crucial that these two initiatives align for either of them to truly succeed.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.