Article Text

Abstract
Objective To assess the feasibility of Pare de fumar conosco, a web-based smoking cessation decision-making tool, among patients with chronic conditions in Brazil.
Methods We recruited 85 Brazilian smokers in two clinical centres for chronic conditions to complete Pare de fumar conosco. Outcome measures included interest in using smoking cessation resources and self-reported 7-day point prevalence abstinence 12 weeks following the intervention.
Results The average age of participants was 54.2 years old (SD=10.5) and 77.9% had not completed high school. All participants were daily smokers and the majority smoked ≥11 cigarettes per day (63.5%). Pre–post intervention interest in using pharmacotherapy and group counselling significantly increased (82.4% vs 22.4%, p≤0.0001; and 85.9% vs 21.2%, p≤0.0001, respectively). At 12 weeks, eight participants (9.4%) reported 7-day point prevalence abstinence using intention-to-treat analysis (35.2% follow-up rate).
Conclusion The Pare de fumar conosco smoking cessation web-based tool significantly increased interest in pharmacotherapy and behavioural counselling. Additional testing as a formal randomised clinical trial appears warranted.
- smoking
- smoking cessation
- eHealth
- Brazil
- global health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Tobacco use is the leading cause of death and one of the top causes of morbidity worldwide.1 Although the overall prevalence of smoking has been declining, the net number of smokers continued to increase over the past three decades, particularly in low-income and middle-income countries (LMICs).2 In order to change this trend, public health efforts must increase the reach and effectiveness of tobacco cessation interventions, especially in LMICs, where the burden of tobacco-related diseases is greater.3
Brazil is a world leader in comprehensive tobacco control and has achieved a dramatic decline in smoking rates from 34.8% in 1989 to 15% in 2014.4 Tobacco control efforts in Brazil include implementation of taxes, smoke-free policies, national smoking cessation campaigns through the mass media and prominent health warnings on cigarette packages,4 5 as recommended by WHO’s Framework Convention on Tobacco Control.6 Regardless, Brazil still has 21.9 million tobacco users, and in 2015 was listed among the top 10 countries with the largest number of total smokers.4 7
In 1989, Brazil implemented a universal healthcare system—Sistema Único de Saúde (SUS)—including a national smoking cessation programme administered by the Instituto Nacional de Câncer.8 The smoking cessation programme is guided by the Brazilian clinical practice guideline Abordagem e tratamento do fumante (Approach and Treatment for Smokers),8 a publication based on the US clinical guidelines.9 Brazil’s guideline recommends combining pharmacotherapy (nicotine replacement therapy, varenicline and/or bupropion) and in-person behavioural counselling for smoking cessation.8 While SUS provides coverage for both pharmacotherapy and behavioural counselling, these smoking cessation resources remain underused.10 Group counselling was recommended in order to reach and treat a large number of smokers at the same time. There is, however, a long-waiting list for treatment services.11 12 The 2011 Global Adult Tobacco Survey in Brazil found that 45.6% of current smokers attempt to quit, but only 57.8% were advised to quit by a healthcare provider, and only 21.0% used pharmacotherapy or counselling.13
A population-based study conducted in Brazil found that 1 in 10 patients being treated for chronic diseases smoked cigarettes.14 Although most of these patients had been advised to quit (87%), very few received evidence-based tobacco treatment; only 9.4% used behavioural counselling and 6.3% used pharmacotherapy in the past. Overcoming the burden of tobacco use among Brazilian smokers in treatment for chronic health conditions demands affordable, accessible and effective solutions.
Existing evidence support the efficacy of web-based interventions to promote and support smoking cessation.15 Web-based interventions capitalise on the rapidly growing adoption of smartphones and tablets to disseminate effective smoking cessation interventions to a broader audience compared with in-person treatment.16 Despite the potential of web-based interventions to improve smoking cessation, it has not yet been evaluated nor used in Brazil.12 17 Carlini et al assessed the coverage and the quality of web-based interventions available in Portuguese.18 Thirteen web-based interventions were found and analysed. The majority of the interventions did not contain evidence-based information (eg, statements about smoking cessation medications not being helpful to quit smoking, recommendations about continuing smoking if smokers were unsure about the benefits of quitting, suggestions on simply enjoying a cigarette in the event of a relapse, etc), were not interactive and did not offer follow-up support. Another limitation found in this analysis was the lack of financial disclosure as well as no guarantee of privacy concerning users’ information.
Decision-making tools have been shown to improve patients’ knowledge, enhance their ability to solve conflicts and bring clarity regarding treatment options.19–21 Previous studies have analysed the effects of web-based smoking cessation decision-making tools in the USA22–24 and Netherlands.25 Most of these studies were grounded on the theory of planned behaviour.22 23 25 These studies have found that the use of decision-making tools improves smokers’ motivation to quit, increases pharmacotherapy use and increases abstinence rates. The aim of this study is to assess the feasibility of a web-based smoking cessation decision-making tool among Brazilian smokers in treatment for chronic health conditions.
Methods
Subjects and setting
This one-arm feasibility study was implemented at two healthcare centres in the state of Minas Gerais between September 2014 and February 2015: (1) Centro HIPERDIA Minas de Juiz de Fora (CHM-JF), Fundação IMEPEN, Universidade Federal de Juiz de Fora and (2) Serviço de Controle da Hipertensão, Diabetes e Obesidade (SCHDO), da Prefeitura Municipal de Juiz de Fora. CHM-JF and SCHDO are two healthcare centres that provide SUS-sponsored services for people in the general public who have chronic conditions including hypertension, diabetes, kidney disease and obesity. These healthcare centres were selected because they both had internet access and provided smoking cessation services (pharmacotherapy and group counselling).
A research assistant recruited participants in the waiting rooms. Eligible participants (1) were ≥18 years of age, (2) identified themselves as smokers, (3) had a phone number and (4) were willing to complete a baseline and 12 weeks follow-up assessments. Written informed consent was obtained from each participant at baseline.
Intervention
Pare de fumar conosco (Stop smoking with us; www.imepen.com/decidete) was adapted from an existing web-based decision-making tool for smoking cessation developed in English and Spanish for use among Latinos in the USA24 and Mexico.26–28 A panel of Brazilian healthcare professionals adapted the content of the tool to the resources, perceptions and sociocultural characteristics of Brazilian smokers. Adaptations of the intervention included the utilisation of the validated scales for nicotine dependence in Portuguese (eg, the adapted version of the Fagerström Test for Nicotine Dependence for Brazilian smokers29 and the Issa Situational Smoking Score30) and the recordings of new videos displaying a local landmark.
Pare de fumar conosco draws on principles from the social cognitive theory, comprising motivational messages, behavioural change support and pharmacotherapy use (nicotine replacement therapy and bupropion). The software was developed to help participants tailor their quit plan and identify the‘how’, ‘when’ and ‘where’ of quitting smoking. The software used an open source relational database management system based on Structured Query Language and Hypertext Preprocessor language. The decision-making tool contained videos featuring a professional actor guiding smokers through the programme, as well as a testimonial from a former smoker. The software also collected sociodemographic information, smoking behaviours and nicotine dependence. It used these data to provide personalised content regarding cessation treatments (pharmacotherapy and counselling). The software combined animations and audios to overcome low literacy barriers and increase interactivity.
The use of Pare de fumar conosco took approximately 15–25 min per participant to complete. The tool was connected to a wireless printer that printed two forms. The first form provided participants with their own reported reasons for quitting, level of tobacco dependence, treatment preferences and behavioural strategies. This form also suggested the participants to discuss their quit plan with their healthcare provider. The second form contained a report for the healthcare provider with a summary of the participant’s smoking behaviours, desired strategies for quitting and suggestions for how the provider could help the participant quit.
Participants who opted to set a quit date were invited to attend an in-person meeting at the healthcare centre to learn about the clinic’s smoking cessation programme. The programme consisted of free group-counselling sessions and free pharmacotherapy (nicotine replacement therapy or bupropion) if indicated (only for participants who smoked 10 or more cigarettes per day).31 The sessions consisted of intense cognitive–behavioural therapy, which included behavioural skills training.31 The programme was structured in 4 weekly 90 min sessions, followed by 12 monthly sessions, until the completion of 1 year of treatment.31
Measures
Baseline data were collected through the decision-making tool and included sociodemographic variables such as age, gender, educational level and contact information. At the beginning of the tool, participants were asked if they were interest in using smoking cessation pharmacotherapy and/or in participating in a behavioural counselling. Moreover, participants were asked to rate their interest and confidence in quitting smoking using an analogical scale from 0 to 10. Other variables assessed at baseline included nicotine dependence, assessed using the Fagerström Test for Nicotine Dependence29 as well as Issa Situational Smoking Score,30 number of cigarettes smoked per day, previous quit attempts, previous use of pharmacotherapy and counselling, and depression.32 At the end of the tool, participants were asked to set a quit date and select treatment preferences (pharmacotherapy and counselling).
Immediately after using of the tool, research staff conducted an assessment on participants’ interest in using smoking cessation pharmacotherapy and in behavioural counselling. Moreover, participants were asked to rate their interest and confidence in quitting smoking using an analogical scale from 0 to 10. Research staff conducted a follow-up assessment over the phone 12 weeks after the utilisation of the decision-making tool. Data collected at follow-up included self-reported 7-day point prevalence abstinence and utilisation of group counselling.
Analysis
Simple frequencies and percentages were calculated for categorical variables including the number and percentage of smokers who used and completed the decision-making tool. For continuous variables, means and SD were obtained. χ2 tests and paired t-tests were used to examine differences between categorical and continuous outcomes, respectively. Following the new recommendations from American Statistical Association and other research initiatives,33–35 we did not assume any threshold for statistical significance, and p values were interpreted as the probability for the observed difference, given the null hypotheses (the probability to observe the difference by chance). Abstinence rates were reported in an intention-to-treat manner, which included all participants in the analysis and counted all participants who could not be reached for follow-up as smokers. Participation in the group-counselling programme was also reported in an intention-to-treat manner, which included all participants in the analysis and counted all participants who could not be reached for follow-up as not having participated in the programme.
Results
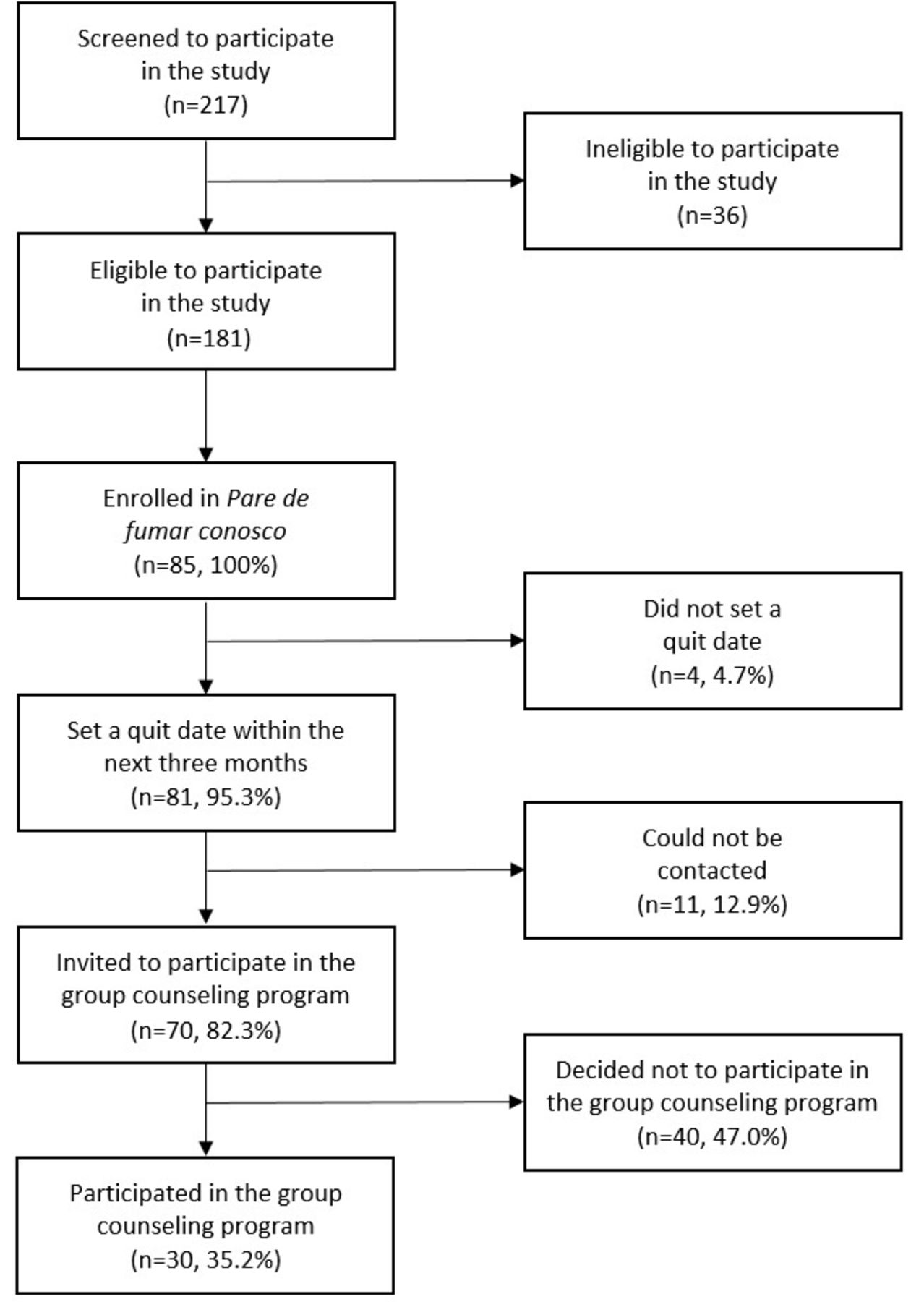
A total of 217 subjects were screened, 181 were eligible to participate and 85 agreed to participate and complete the follow-up assessment (see figure 1). As described in table 1, participants’ average age was 54.2 years (SD=10.5), 54.1% were women and 77.9% had not completed high school. All participants were daily smokers and the majority smoked 11 or more cigarettes per day (63.5%). More than half of the participants (58.8%) had high nicotine dependence on the Fagerström test, but moderate dependence on the Issa test (67.1%). Half of the participants screened positive for depression (50.6%) and made a quit attempt in the previous year (57.7%).
Sociodemographic characteristics of the sample
{kind=link}
Study flow chart.
After utilisation of the tool, 81 participants (95.3%) set a quit-date. Table 2 presents the results prior to, and immediately after, completing the tool. Utilisation of the web-based decision-making tool significantly increased almost fourfold the interest in using pharmacotherapy (82.4% vs 22.4%; p≤0.0001) and group counselling (85.9% vs 21.2%; p≤0.0001). Moreover, the tool significantly increased confidence in quitting smoking among participants (x̅=7.8 vs x̅=7.0; p=0.02), although the difference was small. Finally, the tool also increased interest in quitting smoking (x̅=8.7 vs x̅=8.6), although this was not significant, given the high p value and the small difference observed.
Interest and confidence in quitting smoking prior and immediately after the intervention (n=85)
Of the 81 participants that set a quit date, 70 (86.4%) were reached to receive an invitation to the in-person meeting to learn about the group counselling programme. The remaining 11 participants could not be contacted due to wrong or not valid contact information (provided by participants as they completed the tool).
Thirty participants completed the 12-week follow-up survey (35.2% follow-up rate). Using intention-to-treat analysis, eight participants (9.4%) reported 7-day point prevalence abstinence. All participants who completed the 12-week follow-up survey reported participating in the group-counselling programme: 35.2% using intention-to-treat analysis.
Discussion
To the best of our knowledge, this is the first study assessing a smoking cessation decision-making tool in Brazil. Pare de fumar conosco significantly increased interest in pharmacotherapy and behavioural counselling, and significantly increased confidence in quitting among Brazilian smokers.
Brazil has implemented comprehensive tobacco control policies, including government-sponsored smoking cessation programme for the public.4 5 8 However, these programmes face limitations. Approximately 40% of the Brazilian smokers do not receive adequate advice from healthcare providers to quit smoking.13 Also, many Brazilian smokers appear to be unaware of available treatments, or do not know how effective the treatments are.36 37 As a result, the smoking cessation programmes offered by SUS are underused.10 If widely implemented, Pare de fumar conosco could better enable healthcare clinics in Brazil to reach smokers and offer treatment.
Consistent with the studies that have analysed the effects of web-based smoking cessation decision-making tools in the USA and Mexico, Pare de fumar conosco increased interest in using pharmacotherapy and group counselling.24 26–28 However, cessation rate at 12 weeks was lower in this study (9.4% vs 19.1% in Mexico and 11.8% in the USA). Conducting the study in healthcare centres for chronic conditions could account for the low cessation rate. The study in Mexico was conducted in two primary healthcare settings, and the study in the USA was conducted in safety-net clinics and health fairs. This result highlights the need for future research to focus on the implementation of web-based tools in multiple healthcare settings and among certain populations, including smokers with chronic conditions.
As only 46.9% (85/181) of eligible smokers agreed to participate in the study, further evaluation on the barriers and facilitators to reach and recruit Brazilian smokers into clinic-based cessation studies is needed. One of the reasons smokers were not able to enrol in the study was lack of time due to having multiple medical appointments in 1 day. Pare de fumar conosco needs to be better aligned with clinical appointments and workflow processes to improve the reach of the intervention.
This study has some limitations that should be considered when interpreting the findings. First, retention rate at 12 weeks was low (35.2%). As 77.9% of participants had not completed high school, economic factors could account for the low retention rate. Brazilians who have not completed basic education often work multiple jobs with varying schedules and may not have the freedom to attend group-counselling sessions and schedule follow-up appointments. This suggests a need for developing innovative strategies to deliver treatment and conduct follow-up assessments that specifically target and address the need and preferences of low educated individuals participating in smoking cessation studies. Moreover, as 50.6% of participants screened positive for depression, depressed mood could also account for the low retention rate. Studies conducted in the USA have shown that participants with greater depression are more likely to drop out from smoking cessation treatment.38–40 Future studies should assess depression as a predictor of retention in smoking cessation treatment among Brazilian smokers. Another factor that could account for the low retention rate was the lack of incentives for study visits (eg, reimbursing participants for their travel and time). Providing payment for completion of research assessments can increase the likelihood that outcome data will be obtained.41 A second limitation of the study, as with many smoking cessation clinical trials, was that the inclusion criteria excluded those smokers who did not define themselves as a smoker, which may inadvertently have excluded many light and non-daily smokers.42 Even so, one-third of the sample met criteria for light smoking (smoke 10 or less cigarettes per day). Third, biomarkers were not used to verify smoking status, making it possible that actual quitting rates were lower.43 Fourth, we did not assess chronic conditions that participants had. Fifth, as 30.6% and 58.8% of participants had moderate and high nicotine dependence, it remains unknown whether these preliminary results (eg, interest in using smoking cessation resources and 7-day point prevalence abstinence at 12 weeks) can be generalised to Brazilian smokers with low and no nicotine dependence. Finally, this study was conducted at two clinics with wireless internet capacity; many healthcare clinics in Brazil still lack high speed internet connections, especially in rural areas.
Future studies should link Pare de fumar conosco to other counselling resources (eg, telephone quit-lines or text message-based interventions) that can be tailored to information provided by participants using the tool, such as smoking behaviours and characteristics. Evidence suggests that the potential for text messages to deliver smoking cessation treatment may be even greater among hard-to-reach and socioeconomically disadvantage populations,44 like the one assessed in this study. Cruvinel et al showed the feasibility of a hybrid telephone and text messaging counselling intervention among postdischarge hospitalised smokers in Brazil.45 This hybrid intervention was well accepted by participants and resulted in noteworthy retention and cessation rates at 12 weeks.
Conclusion
Pare de fumar conosco is the first smoking cessation decision-making tool to be developed in Portuguese and conducted in Brazil. The decision-making tool significantly increased interest in pharmacotherapy and behavioural counselling. Our findings demonstrate the feasibility of a web-based tool to support treatment engagement among Brazilian smokers. Additional testing as a formal randomised clinical trial, taking into account the results of this feasibility study (eg, reach of the intervention and linkage to other counselling resources), appears warranted to better understand the outcomes of Pare de fumar conosco. Future research should explore the relationship between smoking behaviour and the presence of chronic illness.
References
Footnotes
Contributors APC, FABC, AGdSG, EFCB and KPR contributed to the conception and design of the work. AGdSG and MAF contributed to the data collection. FABC and TDBF contributed to the data analysis. APC, FC-B, FABC and KPR contributed to the writing of the final revised manuscript.
Funding This study was funded by Fundação de Amparo a Pesquisa do Estado de Minas Gerais (FAPEMIG) under grant APQ-03603-13.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Human Subjects Committee of the University Hospital, Federal University of Juiz de Fora (HU/UFJF) approved and monitored the study procedures (protocol 24883413.5.0000.5133).
Provenance and peer review Not commissioned; externally peer reviewed.