Article Text

Abstract
Background Office workers spend a high percentage of their time sitting, often in long periods of time. Research suggests that it is healthier to break these long bouts into shorter periods by being physically active.
Objective We evaluated the effect of a context-aware activity coach, called the PEARL app, an mHealth intervention that provides activity suggestions, based on a physical activity prediction model, consisting of past and current physical activity and digital agendas.
Method Fifteen office workers, aged 50+, participated in an intervention study in which they used the intervention for 1 week, preceded by a 1-week baseline period. Measurements were taken before and after the intervention period.
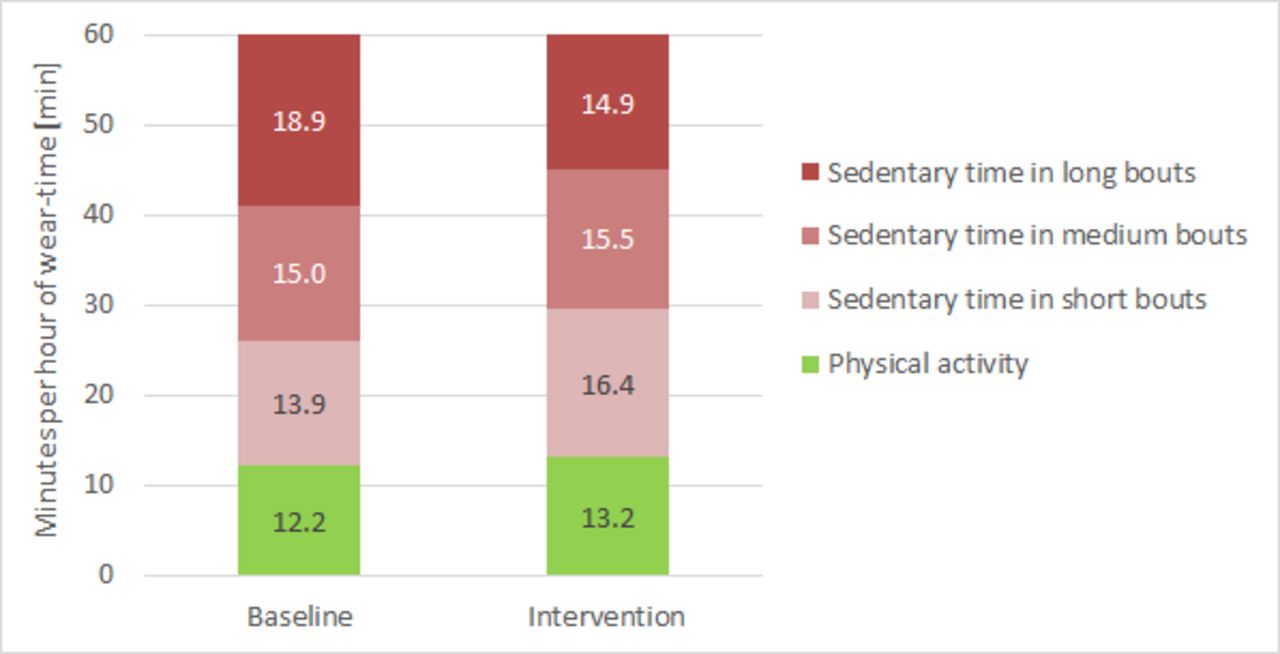
Results 107 days of data from 14 participants were analysed. Total sedentary time was not reduced as a result of using the intervention (baseline vs intervention: 47.8±3.6 vs 46.8±3.0, n.s.). When using the intervention, participants reduced their total time spent in long sitting bouts (≥45 min) from 19.3 to 14.4 min per hour of wear time (p<0.05). Participants indicated that the main value of the intervention lies in creating awareness about their personal sedentary behaviour pattern.
Conclusion An mHealth service has the potential to improve the sedentary behaviour of older office workers, especially for breaking up long sedentary periods. Focusing on total sedentary time as an outcome of an intervention, aimed at reducing sedentary behaviour, is too simplistic. One should take into account both the duration and the number of bouts when determining the effect.
- sedentary behaviour
- physical activity
- pattern
- break
- bout
- wearable sensor
- mHealth
- intervention
- office workers
- awareness
- added value
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- sedentary behaviour
- physical activity
- pattern
- break
- bout
- wearable sensor
- mHealth
- intervention
- office workers
- awareness
- added value
Summary
What is already known?
Prolonged sitting is a health risk.
Reducing the average time of a period of sitting has only recently been recognised as an important goal.
Digital interventions have been found to be promising means to improve sedentary behaviour in the office.
What does this study add?
Implementation of a context-aware activity coach among older employees leads to a replacement of longer bouts of sedentary behaviour by shorter bouts.
Employees think that the main value of the coach lies in creating awareness about their personal sedentary behaviour pattern.
The best measure for describing a sitting pattern is the total time in various bout durations.
Our study shows that a context-aware activity coach can successfully withhold older office workers from long periods of sitting.
Background
Prolonged sitting is a health risk1–3 as prolonged sitting periods are associated with higher waist circumference, body mass index, and triglyceride and blood glucose levels.4 In industrialised countries, most working adults spend a high proportion of their waking hours in sedentary occupations seated at a desk. Clemes et al5 identified that for British older office workers, the percentage of wear time spent sedentary is 68% on work days (vs 60% of non-work days); Thorp et al6 even found that Australian office workers were sedentary for 76% of their working hours, of which almost half of this time is accumulated in prolonged sedentary periods of 20 min or more, and approximately one-third is accumulated in periods of 30 min or more. And while much attention has been devoted to reducing the overall sitting time of office workers, reducing the average time of a sitting bout—a period of uninterrupted continuous sitting time—has only recently been recognised as an important goal.7 8 Especially for the target group of older adults (who are an increasingly large group of the total workforce) that need to be supported to remain physically healthy, sitting time and the length of sitting periods need to be reduced.9
Digital, multicomponent interventions (eg, smartphone apps that use data collected by activity sensors and that motivate end-users using, for example, prompts or goal setting) have been found to be promising means to improve sedentary behaviour in the office.10–12 These mHealth interventions (healthcare interventions using mobile wireless technologies13) have the great advantage that they can consider personal work-rhythms when providing health advice. In this study, we report the evaluation of a context-aware activity coach, called the PEARL app, that consists of a smartphone app and physical activity sensor. It builds a personal activity profile and suggests a short break from prolonged sitting or to become physically active, at a personally suitable time.
Methods
The PEARL application
The PEARL app aims to (1) decrease total sitting time during working hours and (2) break up long sitting periods of more than 45 min. It provides intervention messages and feedback via a smartphone application, tailored to the personal physical activity rhythm of the user and a user’s personal agenda (based on calendar items in Outlook). See figure 1 for the different technology modules. Physical activity is measured by the ProMove three-dimensional (3D) activity sensor, worn over the right hip. The sensor converts 3D accelerations to counts per minute (unit: 10−3 m/s2), and the coach uses the number and timing of physically active minutes (based on the cut-point for comfortable walking speed14) for the intervention.

Technology modules; left: smartphone application, right: activity sensor.
The app continuously updates the personal activity profile using information about daily physical activity rhythms and activity behaviour before and after each calendar item. Next, this physical activity profile and the current behaviour are input for the real-time construction of the decision rules that support the intervention goals. The main trigger for pushing an intervention message to become physically active is the combination of an individual’s current duration of the sitting period, and the estimated chance of interrupting this sitting period within the near future. This chance is derived from the baseline week and contains the average day rhythm and the behaviour at the start and end of events in the calendar. The estimated behaviour at the start and end of events is updated daily to model each workday individually. As a result, the app will only suggest a short break from prolonged sitting or to become physically activity when this is a suitable time for the user. A sedentary bout ends by at least 1 min of physical activity.
Study design
We conducted an intervention study where participants were asked to use the PEARL app and wear the sensor for 2 weeks, during workdays starting daily before commuting. The first week served as a baseline to gather data for creating the personal activity profile. During the second week, the PEARL app provided feedback and intervention messages of which the timing was based on the individual physical activity profile of the baseline week, combined with current behaviour. The goal of this evaluation was to assess the potential effect of the intervention and to determine the user experience.
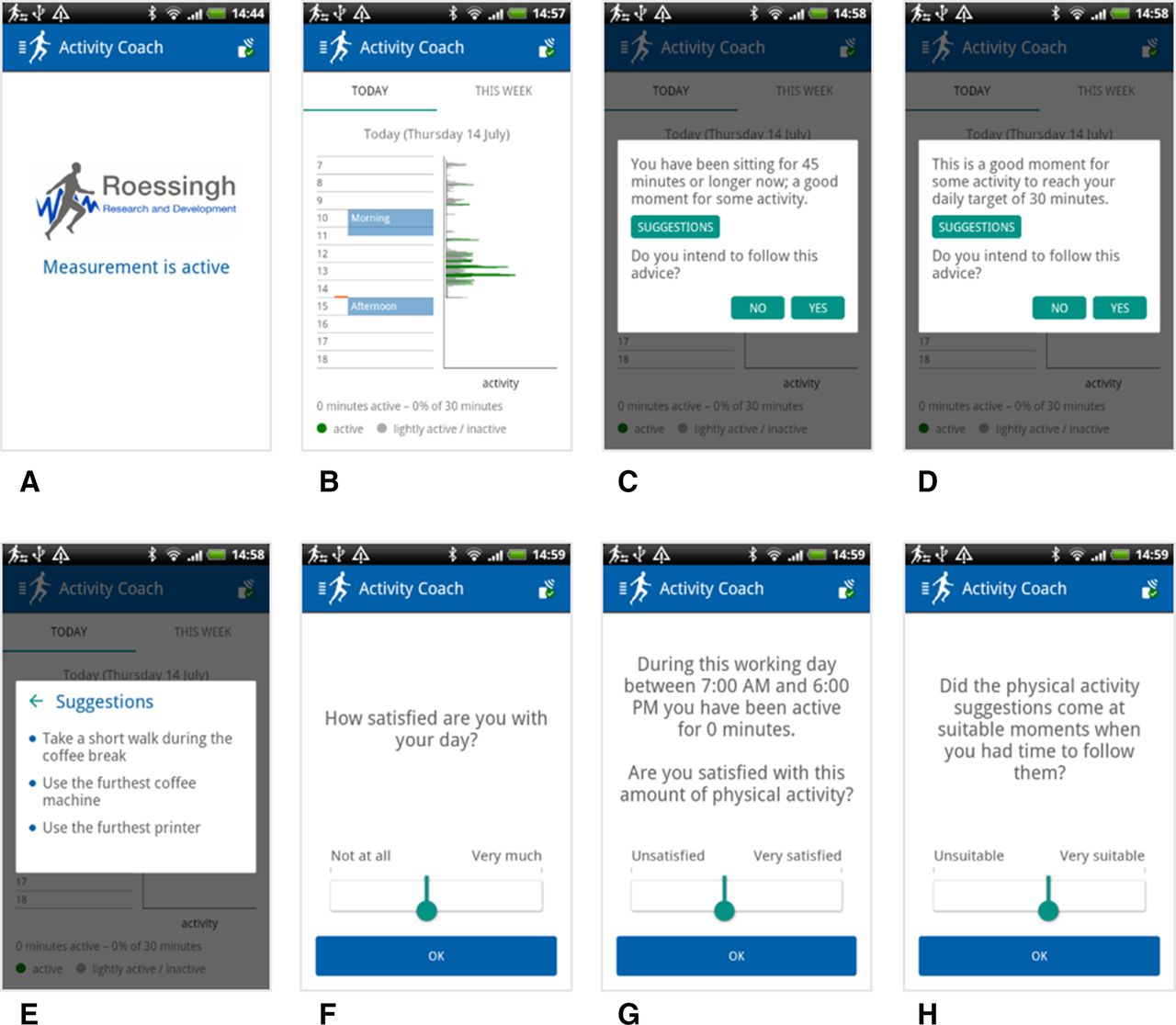
While using the intervention, we assessed participants’ compliance with intervention messages. Each prompt was followed by a question regarding the intention of the participant to comply, as shown in figure 2C and D. Then, at 18:00 hours of each intervention day, the participant received a short questionnaire in the app regarding their (1) satisfaction with their day, (2) satisfaction with the amount of physical activity during that day; and (3) if the intervention messages came at suitable moments during the day. See figure 2 for a flowchart of these questions. After the intervention week, usability was assessed by means of the System Usability Scale (SUS)15 and the user experience via the Mobile Application Rating Scale (uMARS).16 A structured interview was conducted to triangulate results (see online supplementary appendix A for the interview scheme).
Supplemental material

Screenshots during baseline week (A) and intervention week (B–H): (A) home screen; (B) home screen showing physical activity and outlook calendar items; (C) and (D) two types of intervention messages; (E) suggestions for physical activity; (F–H) questions regarding satisfaction with the day (F), satisfaction with physical activity (G) and satisfaction with the timing of prompts (H).
Participants
Participants were recruited via the Human Resource department of the University of Twente, Enschede, The Netherlands. Inclusion criteria were (1) age ≥50 years old and (2) being an office worker and using a personal computer (PC) or laptop for at least 50% of their working time. Exclusion criteria were physical impairments that hindered effective use of the intervention (eg, colour blindness).
Analyses
Physical activity measures were calculated on a daily level. A valid day consists of at least 4 hours of wear time. The overall physical activity level was assessed via the mean intensity of counts per minute per day and the percentage of sedentary minutes per day. Minutes were classified as being sedentary when ≤1660×10−3 m/s2.17 The physical activity pattern was measured by the number of sedentary bouts. We distinguish short (<20 min), medium (20–44 min) and long bouts (≥45 min) and analysed both the number and the total time in these bout lengths. Total time was normalised to minutes per hour of wear time. Changes in physical activity were statistically tested for intervention versus baseline period using the paired t-test or Wilcoxon signed-rank test. All questions related to satisfaction were accompanied by a visual analogue scale, ranging from 0 to 10. A score for usability was calculated using the standardised SUS scoring method. User experience scores were calculated via a composite score, and averages for the different uMARS categories, following Stoyanov et al.16 Interview transcripts were analysed via a question analysis approach,18 where we made a frequency table for the different answers, given to each question, was made.
Results
Participants
Fifteen subjects participated. Their mean age was 58.93±5.4 and seven were male. Their professions were categorised as researcher (n=5), administration (n=4), technician (n=3), (project) management (n=2) and care professional (n=1). Participants indicated to work, on average, 69% of their worktime with a PC, varying from 30% for some researchers up to 100% for some technicians.
In summary, the participants wore the activity sensor for 126 days, of which 110 were valid. One subject did not have any valid intervention days and was excluded from analyses. Participants had, on average, 3 baseline days (range 1–5) and 4.6 intervention days (range 2–16). The average duration of a valid day was 9.5±2.1 hours, with only 5 days between 4 and 6 hours.
Physical activity pattern
Table 1 displays the different outcome measures, related to physical activity. The participants’ daily physical activity level did not differ significantly between the baseline (M=958, SD=208) and the intervention period (M=1019, SD=174), t(13)=1.43, p=0.176, nor did the average, overall sedentary time per day (baseline (M=47.8, SD=3.6) versus intervention period (M=46.8, SD=3.0), t(13)=−1.24, p=0.239).
Overview of physical activity pattern measures
The median time in long bouts was significantly lower during the intervention (Mdn=14.4), Z=−2.54, p=0.011, compared with the baseline period (Mdn=19.3). The median time in short bouts was significantly higher during the intervention (Mdn=16.9), Z=−2.29, p=0.022 compared with the baseline period (Mdn=14.8). Finally, the median time in medium bouts did not significantly differ between the baseline (Mdn=15.1) and intervention (Mdn=15.9), Z=−0.53, p=0.594, while the combined medium and long bouts were significantly lower during the intervention (Mdn=35.2), Z=−2.92, p=0.004, compared with the baseline period (Mdn=31.2).
The total number of bouts per hour of wear time increased significantly from baseline (M=3.75, SD=0.62) to intervention (M=4.11, SD=0.66), t(13)=2.71, p=0.018. The total number of long bouts per hour of wear time decreased significantly from baseline (M=0.28, SD=0.06) to intervention (M=0.22, SD=0.09), t(13)=−2.77, p=0.016. The median number of short bouts significantly increased from baseline (Mdn=2.93) to intervention (Mdn=3.34), Z=−2.48, p=0.013. The ranks of the median number of medium bouts did not significantly change from baseline (Mdn=0.49) to intervention (Mdn=0.54), Z=−0.35, p=0.73, nor did the sum of the number of medium and long bouts change significantly from baseline (Mdn=0.79) to intervention (Mdn=0.74), Z=−1.60, p=0.109. These results suggest that longer bouts of sedentary behaviour were replaced by shorter bouts. We have plotted these distributions in minutes to an hour of wear time (see figure 3).
{kind=link}
{kind=link}
{kind=link}
Distribution of the average time per hour of wear time as sedentary or physically active.
Compliance
In total, we gathered 57 intervention days with 276 prompts. On average, participants received six messages per day. They indicated to follow the advice for an average of 3.2 of these messages (52.6%). The participants (n=12) rated the timing of the intervention messages at the end of each workday with an average score of 3.2±1.6 on a scale from 0 to 10.
User experience
The usability was rated ‘acceptable’, with a score of 77.9 on the SUS, while the user experience was rated ‘acceptable’ to ‘good’ with an overall score of 3.59 on the uMARS. The average scores for the uMARS subconstructs Engagement, Functionality, Aesthetics and Information were 3.08, 3.68, 3.71 and 3.88, respectively. Additionally, the average UMARS subjective quality score was ‘good’ (2.98). Participants mainly indicated that they would not pay for the intervention, but expected their employer to pay. Finally, the UMARS perceived impact scale was rated, on average, as 3.18, indicating that participants slightly agreed that the coach increased their knowledge, attitudes and intentions.
Via interviews, we elicited the reasons for a positive or negative user experience, and uncovered the usability issues that the participants encountered. Most participants indicated that they felt that the PEARL app could be of added value (n=11). They mentioned that it created awareness on the need to become more physically active during the workday and provided insight into their physical activity pattern. Additionally, it motivated them to become active if the coach indicated that they were not active enough. One participant stated: “The module gave me the insight that I am active, so in that way it was nice, but I do not think I would use it on the long term.” Another person said: “[The added value is] mainly [on] interrupting long periods of sitting.” Those participants that indicated that the intervention was not of added value to them believed that they were sufficiently physically active during the day.
Most participants stated that the intervention created awareness on their physical activity and sitting behaviour (n=9) and provided insight in their physical activity pattern (n=9). Physical activity suggestions (n=3) were appreciated, as well as the graphical user interface (n=2). Negative aspects mentioned by the participants mainly concerned the timing of suggestions (n=10), the size of the sensor (n=6) and losing wireless connections (n=2). Participants suggested to improve the timing of suggestions in such a way that it is not disturbing them (eg, not when being in a creative process, while lecturing or a while after being physically active).
Discussion
Main findings
In this study, we evaluated the potential effect and user experience of a context-aware activity coach, called the PEARL app, an mHealth service that aims to improve the sedentary behaviour of older office workers. Using the technology did not lead to an improvement in overall sitting time. However, using the coach did allow older office workers to increase their sitting time in short bouts (<20 min) and decrease their sitting time in long bouts (≥45 min), while sitting time in medium bouts (20–44 min) was unchanged. With respect to the number of bouts, we found that our intervention reduced the number of long bouts, to the cost of the number of short (which increased). This is an important finding, given that these prolonged periods of sedentary behaviour pose an independent health risk8 additionally to the health risk of overall sitting behaviour. Being able to change the sitting pattern towards being more fragmented can be the initiation of further fragmentation and possibly also reduction of sitting time, thereby reducing the risk of development of chronic diseases.4 19
Usability and user experience of the coach were appreciated positively, with room for improvement. Timing of motivational prompts turned out to be one of the most important aspects shaping satisfaction and the user experience. The office workers in our study indicated that this timing needs to be improved in such that it better follows their work rhythm. Given the fact that the PEARL app is highly personalised, as it offers personal motivational prompts based on previous physical activity and agenda items, this is an intriguing finding. It appears that the presence of an agenda item alone does not serve as a proper indication for being able to move around. For example, creative processes should not be interrupted. In the future, a user’s willingness for being physically active should also be modelled outside appointments.
Comparison to prior work
This study is the first to assess the potential effect of a digital intervention to break up prolonged periods of sedentary time among older office workers. What makes this intervention unique is that it uses personalised activity recommendations based on previous behaviour and agendas. As such, it is an extension of the toolkit for occupational health professionals, which already included adjustable or active desks,20 21 pedometer challenges22 and building design.23
Studies that focus on breaking up sedentary periods commonly use pattern outcome measures based on sitting bouts of 20 min or longer. However, our study shows that the behaviour change predominantly occurred in the sitting bouts of 45 min and longer. Therefore, using a cut-point of 20 min can result in both significant and non-significant changes, depending on whether the focus of analyses lies on the total time in these bouts or the total number of these bouts. We found that the total sedentary time in bouts ≥20 min significantly decreases when using the intervention, while the number of bouts ≥20 min does not. We suggest that the best measure for describing a sitting pattern is the total time in various bout durations. Although the total number of bouts could provide insight in the overall fragmentation of the sitting time, it is not sufficiently sensitive to changes in behaviour.
The PEARL app incorporated several persuasive features, as suggested by Oinas-Kukkonen and Harjumaa.24 For example, it reduced the overall behavioural goal in small activities, provided personalised prompts and allowed for self-monitoring. This study shows that incorporating these features is effective, but at the same time, stresses the need for further specification of these design principles. Stating that a technology should provide personalised advice is too simplistic. Rather, for a specific goal (eg, reducing sedentary time among older office workers), it should be determined which factors contribute to successful personalisation. Then, these factors can be modelled and acted on.
Recommendations for mHealth developers
Based on our interviews, we have the following recommendations for mHealth developers. First, it is preferable if the activity sensor and app are on the same device. The interface of the app should also present insights into the total sitting time and relevant pattern measures to the older office worker in an easily comprehensible manner. With respect to prompts that mHealth interventions can give to engage older office workers in a non-sedentary behaviour, we advise developers to ‘allow’ for physical inactivity after a period of physical activity (eg, 30 min) and to leave an interval of about 60–90 min between prompts so as not to overload the office worker.
Limitations
We included a relatively small number of participants (n=15) in our study. Although this somewhat limits the external validity of our study, focusing on a small number of office workers was the only feasible way to conduct a study that provides the fine-grained results we were aiming for, given the huge amounts of activity data that were generated. Therefore, including a small number of participants, of which large amounts of data are analysed, is a common and sensible approach.25 Some of the participants were familiar with physical activity research and were, of course, aware of the fact that they were being monitored as part of our study (as we did not conduct a classic randomised controlled trial which would have accounted for this effect). This might have affected our results.
The intervention and measurement period was relatively short and the timing was restricted to September. This means that the study did not allow for the assessment of sustained behaviour change. Nonetheless, the study showed that the PEARL app is capable of achieving this change quite rapidly. Next, the consequences of using the intervention may be affected by the time of year in which it is used, as the amount of physical activity is affected by the season and weather conditions.26
Conclusion
In a time where sedentary behaviour is recognised as an important health problem, mobile health technology may prove to be an excellent means to get office workers out of their chairs. Our study has shown that a context-aware activity coach can successfully withhold older office workers from long periods of sitting.
Acknowledgments
The authors would like to thank all subjects who participated in the study. And special thanks goes to Mirka Evers for her contributions to the intervention study and Dennis Hofs and Boris van Schooten for their contributions to the development of the context-aware activity coach.
References
Footnotes
Contributors All authors substantially contributed to the conception and design of the study. SB analysed and interpreted the physical activity data. SB and LvV were major contributors in writing the manuscript. SB and LvV analysed and interpreted the user experience data. All authors contributed to the drafting and revising of the article and approved the final manuscript.
Funding This work has been done within the PEARL project, funded by the European Ambient Assisted Living Joint Programme and the National Funding Agencies from Austria, Denmark, Germany, Netherlands, Romania and Switzerland (PEARL; AAL-2013-6-091).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was reviewed by the Medical Ethical Committee of Twente, The Netherlands. Since the study was held among healthy volunteers with minimal risks involved, it was waived for approval. All participants provided informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.