Article Text

Abstract
Background Health literacy is defined as the capacity to obtain, interpret and understand basic health information. In each country, the count of published literature is a good indicator for scientific activity. This study aimed to assess the growth rate of scientific production in the field of health literacy in Middle Eastern countries during 2005–2014.
Methods We used the PubMed database and retrieved 839 papers in the field of health literacy from three productive countries in the Middle East: Iran, Saudi Arabia and Turkey. We applied the bibliometric indicator of Price’s Law to assess the increase of scientific literature. The correlation between bibliometric data and some health indicators such as gross domestic product and population was calculated.
Results Worldwide research productivity in health literacy field was 56 653 documents while that from Middle Eastern countries were 839 papers. Iran, Turkey and Saudi Arabia were three productive countries in Middle East. Iran and Saudi Arabia have undergone exponential growth, but Turkey has undergone linear growth over the studied period.
Conclusions In conclusion, although the present data show promising increase and good start in research productivity from countries in Middle East, they have a trivial sharing in publishing scientific papers in the field of health literacy through 2005–2014.
- Health literacy
- Bibliometrics
- Middle East
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Iran, Turkey and Saudi Arabia are leading countries in the Middle Eastern region in the field of health literacy based on research productivity during 2005–2014.
Growth of scientific output on health literacy has been exponential in Iran and Saudi Arabia.
Growth of scientific output on health literacy has been linear in Turkey.
Introduction
Health literacy is a widely used term that encompasses a range of descriptions.1 This term was first used in the USA and Canada, but nowadays it is an international concept in which each country has official definitions of health literacy.2 According to the WHO definition, health literacy represents the cognitive and social skills that determine the motivation and ability of individuals to gain access, understand and use information in ways that promote and maintain good health.2 It implies the achievement of a level of knowledge, personal skills and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions. Thus, health literacy means more than being able to read pamphlets and make appointments.3
According to Schyve’s4 view, low health literacy is one of the ‘triple threats’ to effective health communication.5 Several studies have shown that limited health literacy, which is often defined as the inadequate capacity to read and understand, as well as access basic health information and services needed to make appropriate health decisions is associated with negative health outcomes, less disease knowledge, less effective self-care behaviour and finally increased costs.6–12
The recent bibliometric analysis indicated there has been increased research in the field of health literacy too.13 In fact, the growth in this field has been so rapid that the field of health literacy is becoming at risk for losing track of its own successes and failures.14
Kondilis et al visualised health literacy research in Europe.15 Their study covered the period of 1991–2005 and PubMed database was chosen as a source of data. They examined data from 25 European countries (countries with main affiliation in the European Union and the four candidate countries) plus the USA. They identified 13 710 and 49 523 articles that were published by European candidates and the USA, respectively. Findings of the mentioned research showed that the 25 European countries produced less than one-third researches in health literacy compared with the USA. The Netherlands, Sweden, Germany, Italy and France were the European countries with the highest number of published research in the field of health literacy. For the second time, health literacy of European people was examined. Results showed that >10% of the total surveyed population had an inadequate level of health literacy. This proportion varied between 1.8% and 26.9% by country.16
In the other study in this field, to find scientific outputs related to health literacy topic through 1997–2007, Bankson searched nine databases CINAHL, Health Source: Nursing/Academic Version, PubMed, SocINDEX, PsycINFO, Academic Search Premiere, Educational Resources Information Center and Library and Information Science Technology Abstracts.17 The results of this study showed that PubMed indexed most of articles on health literacy.
To date, most evidence on the prevalence and consequences of health literacy is based on studies from high-income countries. A previous investigation showed that a low-income population had a lower average level of health literacy than a high-income population.18
Based on the study by Wikkeling-Scott and Rikard, health literacy research has only been conducted in 10 Middle Eastern countries.19 However, little research exists to understand the health literacy needs of people in the Middle East. The objective of this paper is to evaluate the growth of scientific output that has been published on health literacy in Middle Eastern countries the past 10 years.
To achieve this aim, this article is organised into five sections. The first one introduces introduction to the topic, explains the subject of this paper and reviews of literature. The second section describes methodology and in the third and fourth parts findings and conclusion are mentioned respectively. Finally, in the fifth section, references of this paper are presented.
Methods
To carry out this study, we retrieved documents from PubMed database and applied Price’s Law indicator about the increasing number of scientific literature. Bibliometric data have also been correlated with some social data, such as population and gross domestic product (GDP) of each country.
Preliminary search in PubMed indicated that Iran, Turkey and Saudi Arabia are the leading countries in health literacy studies by producing 54.68% of publications. The other Middle Eastern countries such as Kuwait, Qatar, Syria, Egypt, Bahrain, Oman, Lebanon, Iraq, United Arab Emirates and Tunisia published about 45.32% of publications. Considering the fact that three countries namely Iran, Turkey and Saudi Arabia are main countries that publish scientific papers in the field of health literacy in Middle East, it was determined to continue our research by assessing the situation of Iran, Turkey and Saudi Arabia through 2005–2014.
Data source
Through preliminary review and test of PubMed, Scopus and Web of Science databases, PubMed showed greater coverage in this field than the other ones. PubMed is a well-known and most popular open-access database of scientific research.20 It provides access to over 22 million citations in Medline, pre-Medline and other related databases, with link to participating online journals.20 For the purpose of this analysis, in July 2014, through GoPubMed (www.gopubmed.org), we performed a search. GoPubMed is a search engine that retrieves citations according to our query in PubMed.21
Search strategy
To have accurate results, based on our aims of this study, we defined location: Iran, Saudi Arabia, Syria, Turkey, United Arab Emirates, Yemen, Qatar, Jordan, Bahrain, Iraq, Kuwait, Lebanon and Oman as Middle Eastern countries and limited the variable of year to decay from 2005 to 2014.
To find appropriate keywords related to health literacy field, we searched Medical Subject Headings and referred to prior literature in this topic. Keywords included in the search strategy were:
‘health literacy’(TIAB) or readability(TIAB) or ‘health awareness’(TIAB) or ‘health knowledge’(TIAB) or ‘consumer health information’(MESH) or ‘health information’(TIAB) or ‘health promotion’(TIAB) or ‘patient education’(TIAB).
According to the WHO report (https://www.who.int), Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates are classified in the high-income group countries with rapid social and economic development, whereas Egypt, Islamic Republic of Iran, Iraq, Jordan, Lebanon and Syrian Arab Republic are considered as middle-income countries with well-developed public health services and limited resources. In addition, Yemen is put in low population health outcomes with lack of resources for health, political instability and other complex development challenges.
Growth of publication
Price’s Law is an indicator for analysing the growth of publication in a specific research field and defined time in a survey.22 To assess whether the literature production fitted Price’s Law, different regression models were performed. Linear, exponential and logistic curves were explored to determine which best fitted the data of the mentioned countries. If the data fitted better to the exponential line than the others, results were considered as fulfilling the Price’s Law. Logistic models were applied to evaluate the saturation hypothesis of growth.
To assess the annual growth rate (AGR) of publications, following formula was used:
(Current year total−previous year total)/previous year total.
To evaluate the factors related to variation in health literacy research productivity, publication activity was adjusted by country population and GDP, which were from 2014 and were supplied by the World Bank (https://www.worldbank.org); likewise, data analysis was performed using Excel software. GDP of each country is normally accepted as the general benchmark for that country’s economic health and validity. Descriptive statistics were calculated for the variables studied too.
Results
Through 2005–2014, the USA was the leading country in the health literacy field in the world with 21 128 documents. Canada and the UK ranked second and third with 3592 and 3185 scientific outputs, respectively. The results of this study indicated that Middle Eastern countries published 839 scientific papers in the field of health literacy through 2005–2014.
In terms of productivity, Iran, Turkey and Saudi Arabia have obtained the top rank among the Middle Eastern countries and have published the most papers in the field of health literacy through 2005–2014. According to PubMed database, 36.19% of these publications have been published in Iran. Turkey and Saudi Arabia by producing 19.18% and 12.18% of publications respectively, ranked second and third.
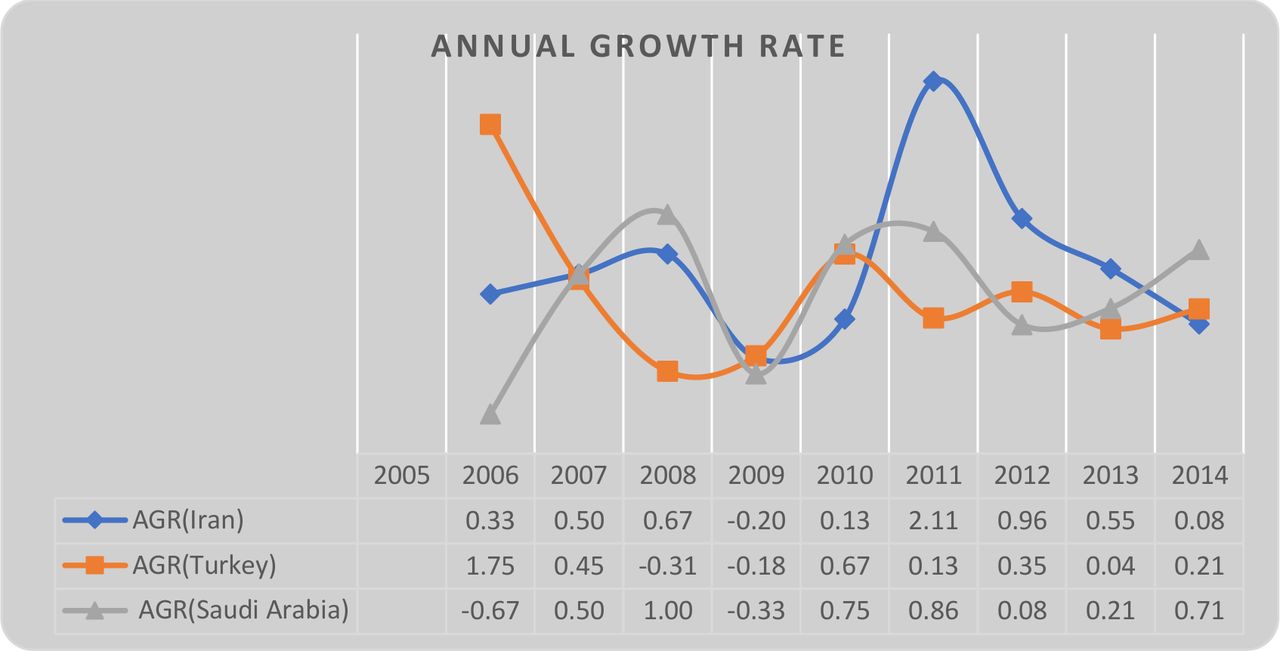
According to the results, the highest growth rate through 2005–2014 belonged to Iran in 2011; Turkey experienced the growth rate of 1.75 in 2006 and Saudi Arabia obtained the growth rate equal to 1 in 2008.
Although Turkey experienced the highest growth rate of 1.75 in publishing scientific articles in the field of health literacy, this indicator has never been repeated in the later years, in which this country has had the negative growth rate in 2008 and 2009 as well as this indicator has never exceeded 1 in Saudi Arabia.
Based on the AGR rate (figure 1), the highest rate was observed in Iran, Turkey and Saudi Arabia through 2011, 2006 and 2009, respectively. Overall, none of the mentioned countries has experienced a steady growth based on the number of publication.
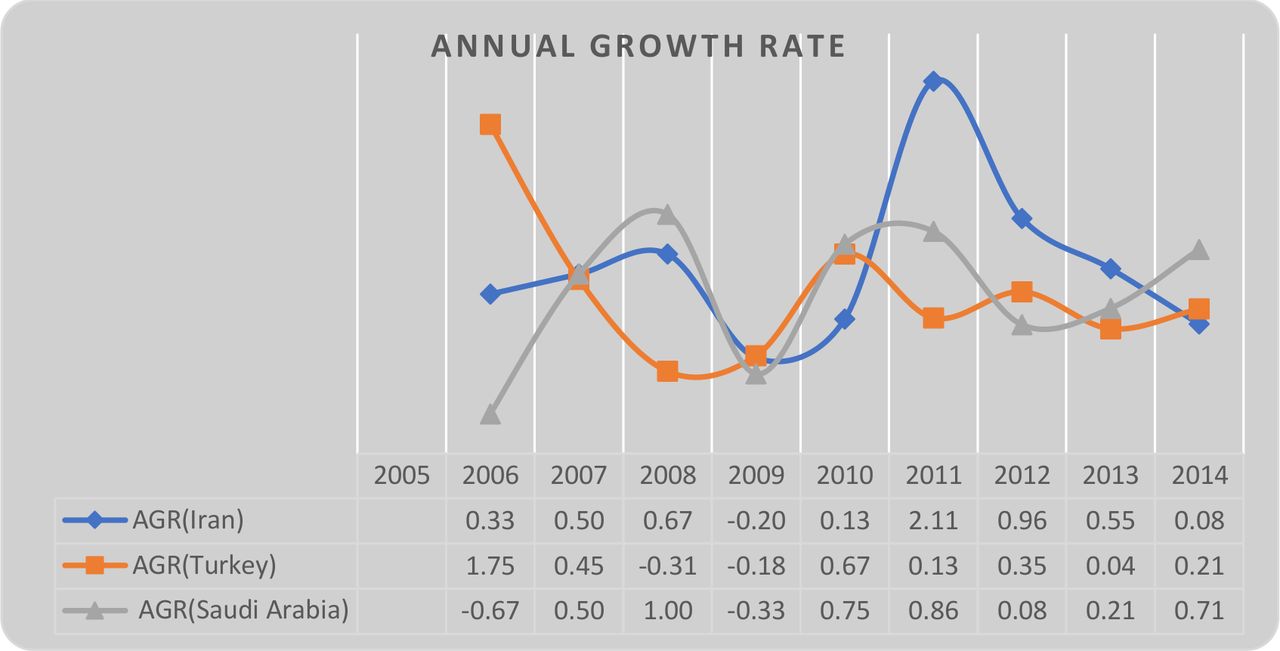
Annual growth rate (AGR) of scientific publications in the field of health literacy in three top countries, during 2005–2014.
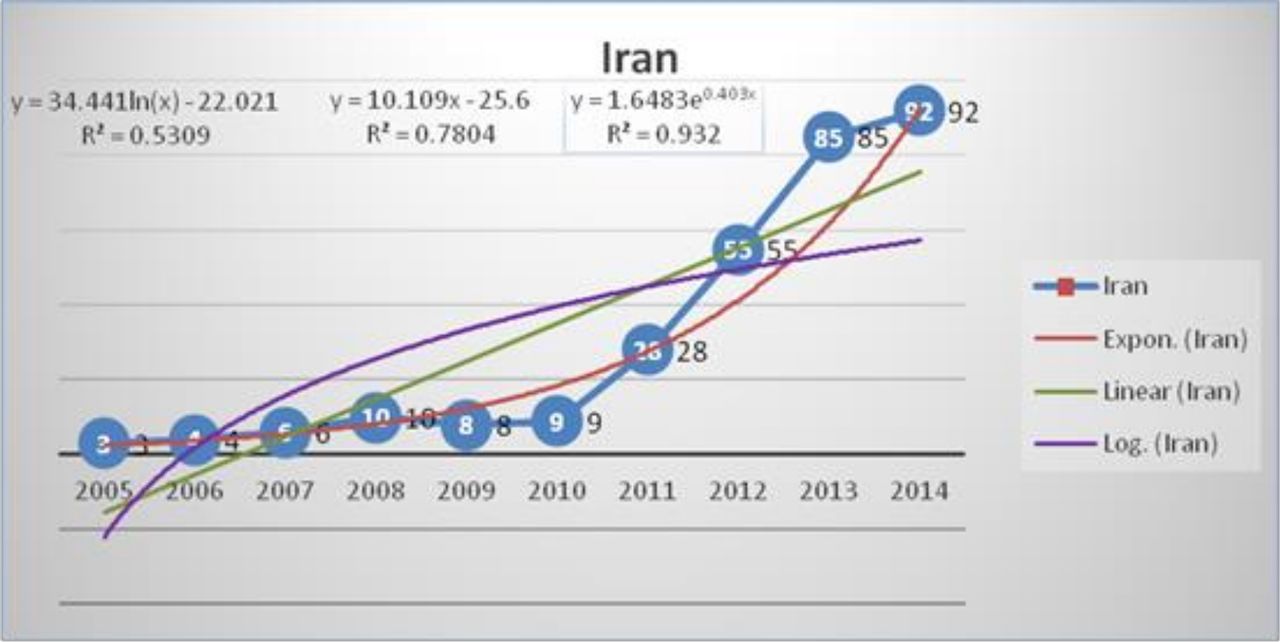
Regarding fitting of three top countries’ researches with Price’s Law, in Iran(figure 2), during the study period, the number of articles grew from 3 in 2005 to 92 in 2014. A significant correlation between the number of articles and the year was observed with a high coefficient of determination. All of the exponential, linear and log curve fitting indicated that there was a high growth rate for annual articles but it was higher in exponential model. The linear, exponential and log fitting curve for health literacy researches in Iran were found to be 0.93, 0.78 and 0.53 respectively.
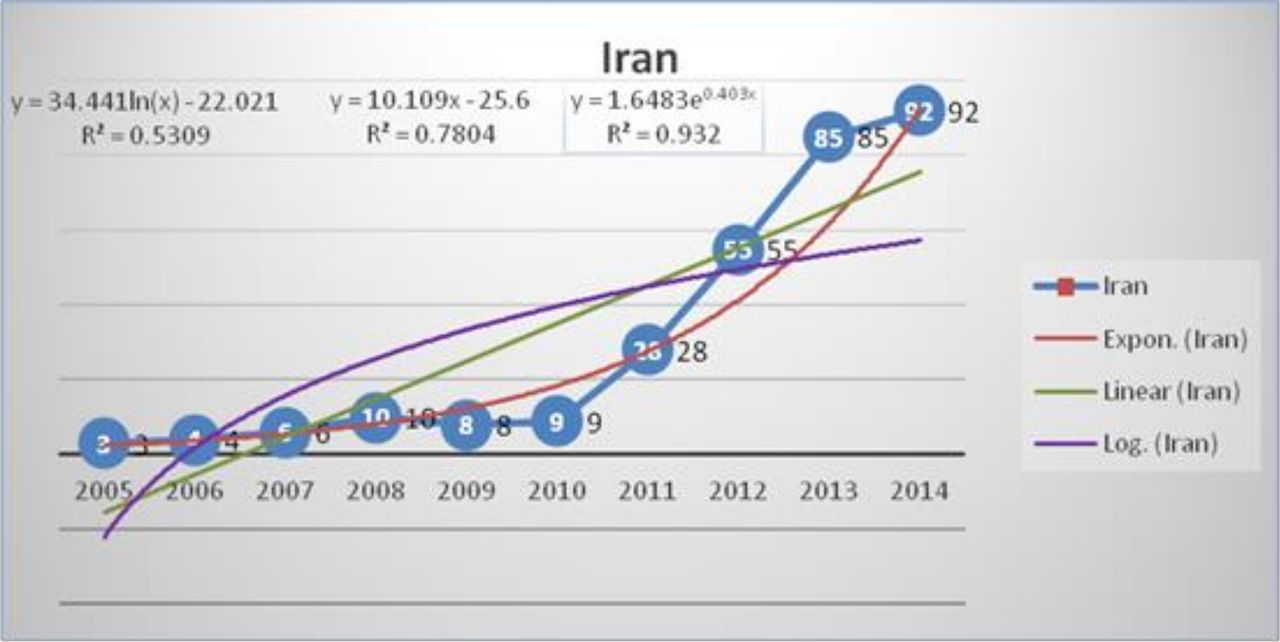
Growth of scientific production on health literacy research in Iran.
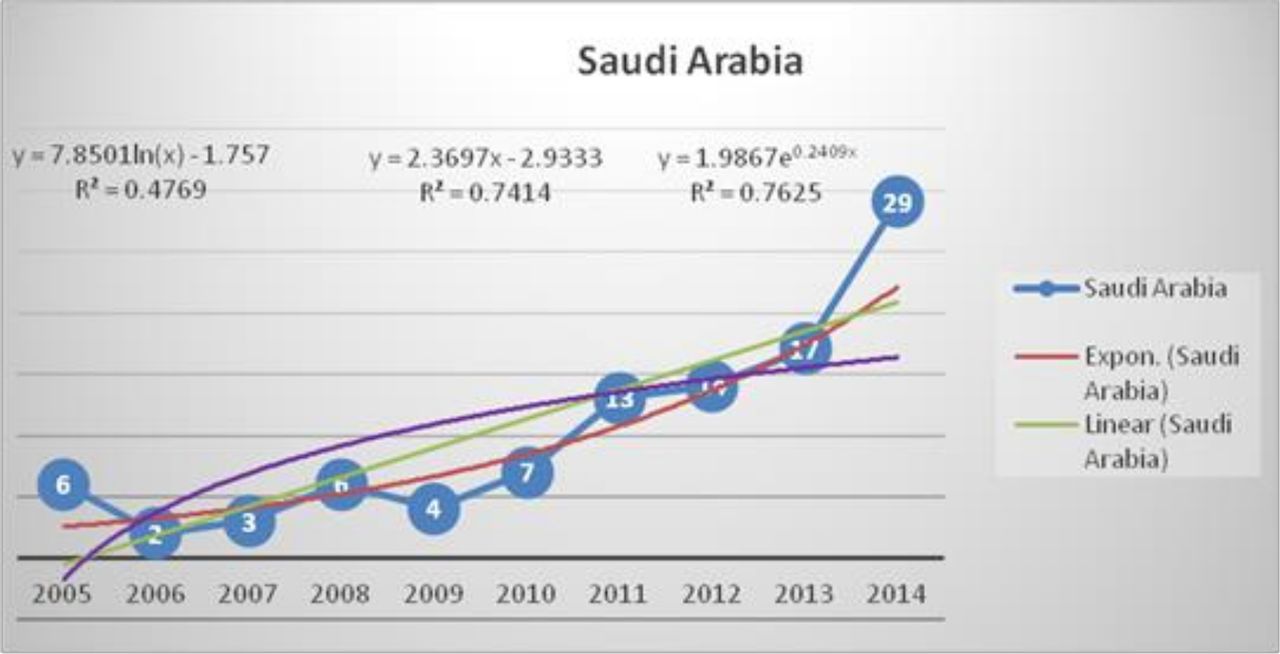
In regard to productivity, over the last 10 years, there have been increase in the number of publications generated in the field of health literacy in Saudi Arabia (figure 3). The mathematical adjustment to an exponential, linear and log curve permit us to obtain a correlation coefficient r=0.76 in exponential model, indicating 24% of variance unexplained by this fitting. In contrast, the linear and log adjustment of the measured values provide correlation coefficients r=0.74 and r=0.47, respectively. With these data, we can conclude that the repertoire analysed is more in keeping with an exponential fitting than a linear one, and that the postulates of Price’s Law are fulfilled.

Growth of scientific production on health literacy research in Saudi Arabia.
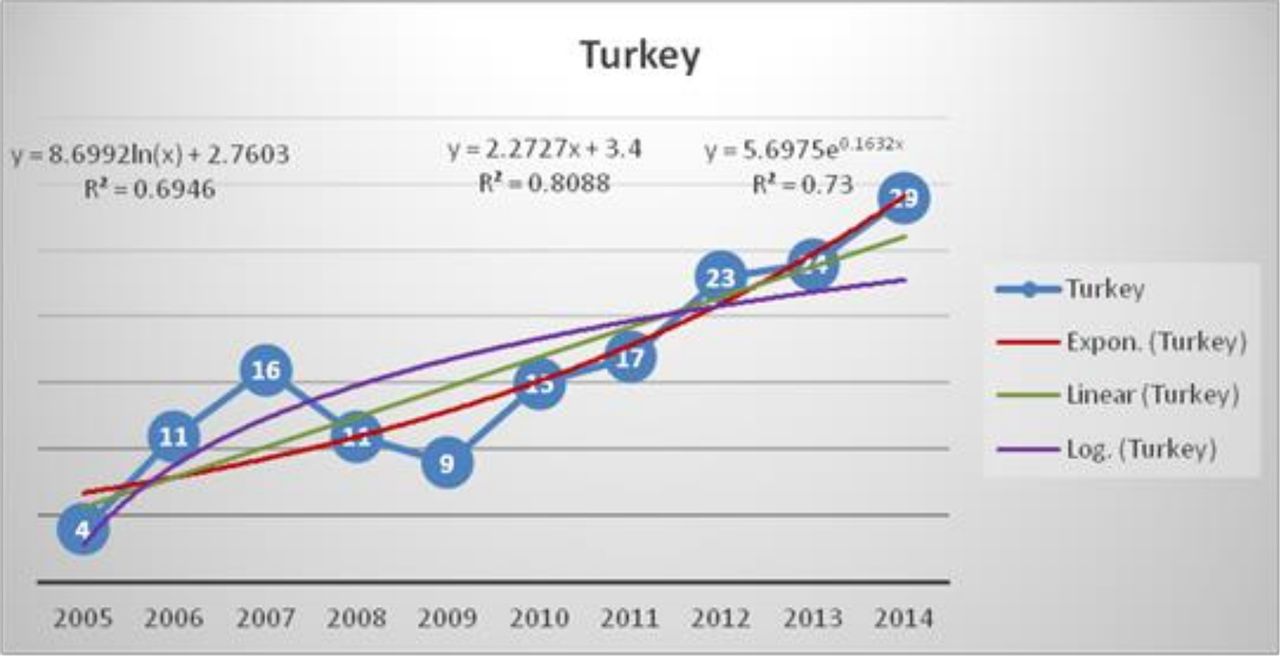
In Turkey, the results also fall into line with Price’s Law of exponential growth (r=0.80 in the linear adjustment, unexplained variance of 20% vs r=0.73 in the linear adjustment, unexplained variance of 27%) (figure 4).
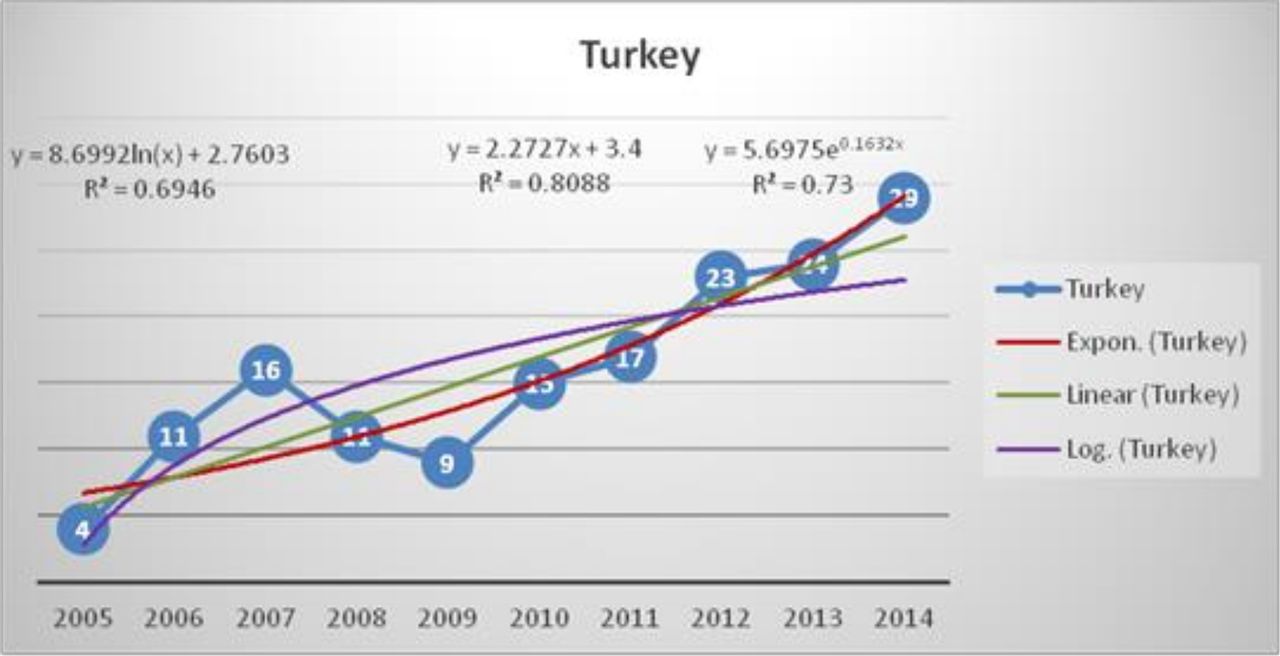
Growth of scientific production on health literacy research in Turkey.
The mathematical adjustment to an exponential curve as shown in figure 4 permitted us to calculate a correlation coefficient r=0.80, indicating 20% of variance unexplained by this fitting. In contrast, the linear adjustment of the measured values provides an r=0.7, with a portion of unexplained variance of 30%. With these data, we can conclude that the database analysed was more in keeping with an exponential fitting than a linear one, and that the postulates of Price’s Law were fulfilled.
The correlation of scientific production in three countries with GDP of each country indicated the positive correlation in Saudi Arabia and Turkey and negative one in Iran (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between production of scientific publications on health literacy in three top countries and population, In addition, correlation between production of scientific output and gross domestic product (GDP) indicator.
Correlation between paper productivity and the population of each country has shown the quite similar distribution, except for Iran that has shown positive correlation.
Discussion
Over the last 20 years, health literacy has become a popular concept in research and health policy.23 In times of rising healthcare costs, policy makers should be especially interested in understanding the mechanisms underlying the inefficient usage of healthcare services. Health literacy as an underlying variable may play an important role in identifying the causes of using healthcare services inefficiently.
From the viewpoint of scientometric science, there are many indicators to assess the scientific output of a country. Productivity and quantity of citations in each article are two of important indicators.
According to the results of this study, the USA holds a pole position in terms of research regarding health literacy as it is a higher producer of public health publications in the world. In this regard, the results lead us to the conclusion that the field of health literacy is not the prime of research in most of the countries in Middle Eastern region. Three countries namely Iran, Saudi Arabia and Turkey based on the number of published research in the field of health literacy in the past 10 years are ranked from the first to third, which is in line with the research by Rashidi et al24 in the other scientific field in Middle East. In other words, these three countries published 67.55% of scientific publishing in the field of health literacy in Middle Eastern region representing the growing interest of researchers in this subject.
Assessing affecting factors in scientific growth of countries indicated that in low-income andmiddle-income countries, scientific advancement has high correlation with economic growth, in which high-income countries accommodate just 16% of population in the world but publish 80% of scientific output.25 On the other hand, low-income countries by having 81% of population in the world, just produced 0.07 of all scientific publications in the world.25
Table 1 indicates that although Iran had acceptable and rapid growth rate in 2011–2014, AGR was declared at the same time. Based on the expert view, economic difficulties, decrease in the current budget of universities, reduction of participation in national or international congresses, decrement in industrial contracts and exchange rate fluctuation in 2011 were the most important factors resulting in decrease of scientific output despite increase in the quantity of articles.26
Quantity of documents published by three top ranked countries in Middle East through 2005–2014
Like Iran, in Saudi Arabia and Turkey the quantity of articles increased steadily during2011–2014,but the growth rate was heterogeneous and did not follow specific pattern.
According to our data, the growth pattern is not similar in these three countries. The scientific output on health literacy has followed an exponential way in Iran and Saudi Arabia and linear way in Turkey. With these data, we can conclude that the postulates of Price’s Law are fulfilled in documents specific to Iran and Saudi Arabia. Exponential increase occurs when there are no limits to growth. However, if there are some intellectual, physical or economic limitations or limitation regarding the size of literature, then other functions such as the logistics may be more appropriate.27
The development of relationships between economic indicators and research activities is a common activity in the field of scientometrics. GDP is the economic growth measured in terms of an increase in the size of a country’s economy.22 It is the main indicator used to measure the strength of a country’s economy and represents the total value of all goods and services produced over a specific time period. With regard to the GDP at first, it should be borne in mind, the higher the spending on health, the greater the research production.22 This regulation is valid for Turkey and Saudi Arabia; some results like this have been previously detected. In Iran, the research publications are in contrast to its GDP in which by decreasing GDP the quantity of publications have increased in the field of health literacy. Another interesting study results indicated that by increasing population, the quantity of publications have increased too.
Conclusions
Iran, Turkey and Saudi Arabia are leading countries in Middle Eastern region based on research productivity in the field of health literacy. In this study, without considering the quality of papers, just the quantities of them have been assessed that is one of the limitations of scientometric studies. Therefore, it has been recommended that similar studies have to be done by considering other international databases like Scopus and ISI Web of Knowledge.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.