Article Text

Abstract
Background An increasing burden of cardiovascular disease (CVD) in low-resource settings demands innovative public health approaches.
Objectives To design and test a novel mobile health (mHealth) tool for use by community health workers (CHWs) to identify individuals at high CVD risk who would benefit from education and/or pharmacologic interventions.
Methods We designed and implemented a novel two-way mobile phone application, ‘AFYACHAT’, to rapidly screen for the CVD risk in rural Kenya. AFYACHAT collects and stores a short message system (SMS) text message data entered by a CHW on a subject’s age, sex, smoking, diabetes and systolic blood pressure, and returns as SMS text message the category of 10-year CVD risk: ‘GREEN’ (<10% 10 year risk of cardiovascular event), ‘YELLOW’ (from 10% to <20%), ‘ORANGE’ (from 20% to <30%), or ‘RED’ (≥30%). CHWs were equipped and trained to use an automated blood pressure device and the mHealth tool.
Results Five CHWs screened 2865 subjects in remote rural communities in Kenya over a 22-month period (2015–2017). The median age of subjects was 50 (interquartile range 43–60) and 1581 (55%) were female. The point prevalence of hypertension (systolic blood pressure > 140 mmHg), diabetes and tobacco use were 23%, 3.2% and 22%, respectively. Overall, the 10-year risk of CVD among patients was <10% in 2778 (97%) patients, from 10% to <20% in 65 (2.3%), from 20% to <30% in 12 (0.4%) and ≥30% in 10 (0.2%).
Conclusions We have developed a mHealth tool that can be used by CHWs to screen for CVD risk factors, demonstrating the proof of concept in rural Kenya.
- mHealth
- low- and middle-income countries
- hypertension
- cardiovascular disease
- Kenya
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Non-communicable diseases (NCDs) account for two out of every three deaths worldwide.1 Of 36 million deaths linked with NCDs globally, 80% occur in low-and middle-income countries (LMICs). The proportion of NCD deaths is expected to increase to 69% of all deaths by 2030.1 The relative increase in NCDs burden has been classified as a global crisis and interventions are needed to address the growing burden in African countries.1,2 NCD deaths are mainly caused by cardiovascular disease (CVD), cancer, chronic respiratory disease and diabetes.3
Although the growing burden of NCDs in LMICs is well recognised, primary data from these countries are scarce and the disease burden may be underreported.1 It is estimated that up to 85% of individuals with diabetes and 66.3% of individuals with hypertension remain undiagnosed.4 Recent studies in Sub-Saharan Africa (SSA) have reported a sharp increase in the occurrence of CVD risk factors in rural areas.4 The rise in CVD is linked to the increase in hypertension, diabetes, obesity and hypercholesterolemia in Africa in recent years. Obesity and hypertension are now common throughout Africa, particularly in urban areas.5 The number of people with diabetes in SSA is expected to more than double between 2000 and 2030.5
Reflecting a continental crisis in human resources for health, SSA, with 11% of the population and 24% of the global burden of disease, has only 3% of the world’s health workers.6 Community health workers (CHWs), defined as members of a community with minimal formal nursing or medical training who provide basic health and medical care to their community, are increasingly recognised as an essential part of the health workforce needed to fill this gap in human resources and achieve public health goals in LMICs.7,8 CHWs can have many responsibilities within a community, including social support, linking to resources and health teaching.9 The prevention, control and management of chronic NCDs may be accomplished by task shifting from professional doctors and nurses to CHWs.6 However, given their minimal training, CHWs need ongoing support to build and reinforce their capacity for healthcare.10
Mobile health (mHealth) is a field of electronic health that provides health services and information via mobile technologies such as mobile phones.11 An estimated 83% of the Kenyan population has a cell phone12 and mHealth tools have the potential to be of immense value to rural communities for the purposes of data collection, disease surveillance and health monitoring.13 mHealth can support the performance of healthcare workers by the distribution of clinical updates, learning materials and reminders, particularly in rural locations in LMICs.14 Although research gaps remain,10 there is growing evidence for the effectiveness of mHealth interventions in LMICs, particularly in improving treatment adherence, appointment compliance, data gathering and developing support networks for health workers.15 A small number of mHealth studies have been done which specifically targeted CHWs, most used a combination of mobile phone applications for data submission, job aids to improve diagnostics and sending and receiving short message system (SMS) messages and reminders. mHealth for NCDs appears feasible for follow-up of patients in SSA, but research in this area has been limited.10
Here, we show that a novel two-way mHealth tool can be used by CHWs to screen for CVD risk factors in rural Kenya. This is a potentially scalable strategy that could be widely applied across many settings in Africa for primary prevention as well as active case detection and referral of high-risk patients who would benefit from pharmacologic intervention.
METHODS
Setting
The study was conducted in rural Kenya, in SSA. Kenya ranks 146th out of 188 ranked countries in terms of human development index, and 36% of the population lives in multidimensional poverty.16 Life expectancy at birth is 62 years and leading causes of death in older adults are neoplasms, stroke, pulmonary tuberculosis and cardiac diseases.17 Two rural districts were included in the catchment area of the two collaborating health clinics. The Lewa Downs Health Clinic in Isiolo District (estimated population 142,000) serves the employees of the Lewa Downs Wildlife Conservancy, as well as surrounding communities. The Field-Marsham Medical Center in Marakwet District (estimated population 141,000) serves the employees of the Kenya Fluorspar Corporation (mining company) as well as surrounding communities. Both areas are rural, with subsistence agriculture and mining as the main local industries. The health clinics provide primary healthcare and management of common illnesses under significant resource constraints to geographically vast catchment areas.
Community health workers
CHWs were chosen by collaborating health clinic staff on the basis of past enthusiasm, reliability and engagement with past collaborative medical outreaches. Canadian certified nurses and physicians trained CHWs over one half-day on the fundamentals of healthy living and the basics of CVD, hypertension and diabetes. During these sessions, the CHWs were taught to use an automated blood pressure monitor. In addition, CHWs were taught how to use the AFYACHAT SMS tool, using their own personal mobile telephones, as described below.
AFYACHAT mHealth tool
The custom-made, novel AFYACHAT tool is an electronic data collection and algorithmic risk stratification tool leveraging SMS as its mode of data exchange. The name was chosen because afya means health in Kiswahili (Kenya’s national language). The system was built using RapidSMS, which is a free and open-source framework built with Python and Django.18 RapidSMS provides a flexible platform and modular components for large-scale data collection and automating data analysis and has been used for other mHealth tools.19,20
Users entered the following patient data as a single SMS text message from their cellular telephone (smart phone technology not required): first name, last name, age, sex, tobacco user (yes/no), known diabetic (yes/no) and systolic blood pressure (measured). The SMS text message was sent to the local (Kenya Safaricom) telephone number (cost of transmission USD $0.01), where it was captured in a central database. AFYACHAT then returned to the user an SMS text message with the CVD risk profile, coded as ‘GREEN’ (<10% 10-year risk of cardiovascular event), ‘YELLOW’ (from 10% to <20%), ‘ORANGE’ (from 20% to <30%) or ‘RED’ (≥30%). CHWs used AFYACHAT from their personal telephones, receiving immediate feedback of the CVD risk profile, which they communicated to the patient they were screening.
The basis for the CVD risk estimation contained in the AFYACHAT system is from the World Health Organization’s Prevention of CVD: Pocket Guidelines for Assessment and Management of Cardiovascular Risk (2007). We used the WHO/ISH risk prediction chart for AFR E in settings where blood cholesterol cannot be measured. The risk charts estimate the 10-year risk of a fatal or non-fatal cardiovascular event based on the following inputs: sex, age, systolic blood pressure, smoking status and presence or absence of diabetes mellitus.21
Population screened
CHWs selected a convenience sample of participants over 40 years of age from their communities for screening. The rate and venue for participant screening, and method of approaching community members was left to the discretion of the CHWs, who were well-known in their communities and had tacit knowledge of best practices in their respective areas.
The CHW’s process for screening involved asking the individual for their age, sex, smoking status and diabetes history and then using an automated blood pressure monitor to measure their systolic blood pressure. Using the two-way interactive AFYACHAT and their cellular telephone, this information was submitted in a single SMS and an immediate reply with participant’s CVD risk was received. If the risk level was 10% or greater (not ‘GREEN’), the CHW advised that the individual go to the clinic or meet with the clinic staff on their next outreach visit to the community. Referred patients were seen by clinicians at the collaborating centres, where the need for antihypertensive and/or oral hypoglycaemic agents was assessed, following region-specific WHO guidelines.21 CHWs were remunerated for their time and received re-imbursement for the cost of the SMS messages as a monthly ‘airtime’ stipend.
We evaluated the user experience and field readiness of the AFYACHAT system using non-structured interviews with CHWs and field observations. Qualitative feedback was solicited from end users of the AFYACHAT program (CHWs), and we summarised salient comments grouped by theme. CHWs were observed during interactions with participants while using AFYACHAT, and we used field notes to describe the strengths and weaknesses of the system during ‘real-life’ use in the rural African setting.
Statistical analysis
AFYACHAT automatically records all SMS entries in a central data repository. Data were cleaned by removing duplicate patient entries. Descriptive and comparative statistics were computed using non-parametric methods (Chi-squared test for dichotomous variables and Kruskall–Wallis U-test for continuous variables). GraphPad Prism6 (GraphPad Software Inc., La Jolla, CA) and IBM SPSS Statistics 19 (SPSS Inc., Chicago, IL) were used for analyses.
RESULTS
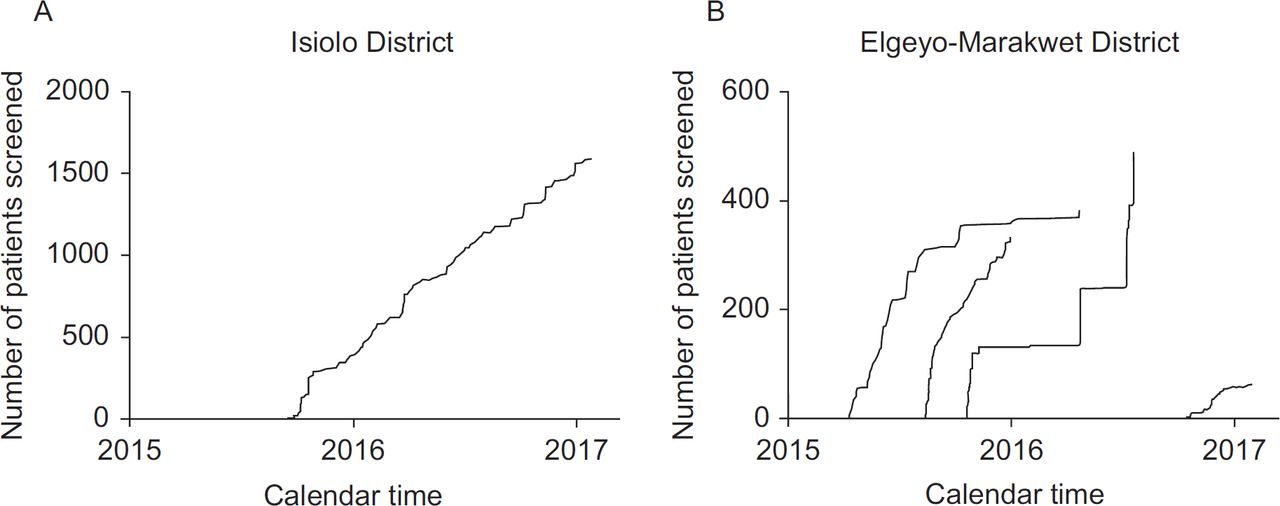
From 10 April 2015 to 2 February 2017, five CHWs screened 2865 community members for the CVD risk in Elgeyo-Marakwet and Isiolo counties, Kenya using the AFYACHAT System. Characteristics of the CHWs were as follows: three female and two male; all had secondary-level education and none had formal nursing or medical training. The cumulative number of patients screened over time by the five CHWs is shown in Figure 1. The rate of screening varied among CHWs, up to 99 patients/month for CHW 1, who screened the largest number of patients.
{kind=link}
Characteristics of patients screened are shown in Table 1. Overall, the 10-year risk of CVD among patients was <10% in 2778 (97%) patients, from 10% to <20% in 65 (2.3%) patients, from 20% to <30% in 12 (0.4%) patients and ≥30% in 10 (0.2%) patients.
Independent risk factors for CVD were inter-correlated, as expected. Age and systolic blood pressure (SBP) were positively correlated (p = 0.065, p = 0.001), and patients older than 65 years had higher rates of systolic hypertension (28% vs. 23%, p = 0.026). Known diabetics were older {median age [interquartile range (IQR)] 55 (50–64) vs. 50 (43–60) years, p < 0.001} and had higher SBP [median (IQR) 144 (129–157) vs. 125 (112–138) mmHg, p < 0.001]. Male and female patients had similar rates of hypertension and diabetes (p > 0.05 for both comparisons).
Tobacco use (including chewing tobacco and cigarette smoking) was prevalent in 30% of males and 15% of females (p < 0.001), increased with age (p < 0.001), and differed between sites/ethno-linguistic groups (41% of the predominantly Kalenjin ethnic group in Elgeyo-Marakwet vs. 6.5% of the predominantly Meru in Isiolo, p < 0.001). In a multivariable logistic regression model, age > 65, male sex and Elgeyo-Marakwet site remained statistically significant independent predictors of tobacco use [adjusted odds ratio (95% CI) 2.0 (1.6–2.6), 9.3 (7.4–12) and 2.2 (1.8–2.7), respectively]. Tobacco use was associated with a lower prevalence of systolic hypertension (17% vs. 25%, p < 0.001), and self-reported diabetes (1.3% vs. 3.8%, p < 0.001). All independent risk factors were significantly associated with increasing AFYACHAT CVD risk profile, as expected, except for tobacco use (Table 1).
Qualitative feedback from the CHWs indicated that the AFYACHAT mHealth tool was simple to learn, easy to use in the field, provided timely responses (CVD risk stratification), and was well accepted by the target population. On the other hand, CHWs reported some limitations of the system in practice. Due to power interruptions at the clinic where the central database was stored, the system was sometimes unavailable when the CHW tried to send an SMS. CHWs reported that they had trouble texting fast enough when there was a large group of patients waiting to be screened. This led to the CHW writing down the results and sending an SMS later, innovating to compensate for technological limitations of the system.
DISCUSSION
We have shown proof of concept that a novel mHealth tool, AFYACHAT, can be used by CHWs to efficiently screen large numbers of patients in rural African communities for their CVD risk. Identifying the silent burden of NCDs in resource-limited rural settings is an important step in the cascade of care to address a growing public health problem. Our AFYACHAT system is potentially a scalable tool which, coupled with the extensive reach of CHWs across rural Africa, could have a substantive public health impact. However, additional implementation experience and data will be needed before widespread uptake of the strategy can be recommended. Innovative aspects of our strategy include: the use of CHWs for CVD risk screening in rural Africa, two-way mHealth technology applied to CVD assessment, a data management system that can be used for programme monitoring and evaluation and use of an open source toolkit, RapidSMS.18
In addition to demonstrating the promising utility of a novel screening strategy and tool, our study provides valuable data on point prevalence of several CVD risk factors in an understudied rural African population. Our results suggest that almost a quarter of the rural Kenyan population over 40 have elevated systolic blood pressure. This prevalence is similar to results from the WHO’s STEPwise approach to Surveillance (STEPS) survey, which found that 23% of all Kenyan participants had raised blood pressure, defined as SBP > 140 and/or diastolic blood pressure > 90 mmHg or currently on medication for raised blood pressure.2 Hendriks et al.,22 who conducted a cross-sectional study across SSA also found the prevalence of hypertension in Kenya to be 24%, but of those 24%, only 2.6% were receiving treatment for their condition. A consistent observation from both the studies is the need for screening and the lack of follow-up, especially by those in rural areas.2,22 National findings on tobacco use suggest that 13% of the Kenyan population between the age of 18 and 69 use tobacco products (both smoked and smokeless), with rates by gender of 23% for men and 4% for women.2 This rate is lower than the measured rate in our study population, 30% for men and 15% for women, with important regional and/or cultural variation in tobacco use. These differences are likely attributable to the older population screened in our study (all participants were over 40); the prevalence of tobacco use in Kenya increases from 13% to 22% in the 60–69 age group in the national survey.2 It is estimated that diabetes occurs in 4%–11% of the urban population and 3% of the rural population in Kenya.23 This is consistent with the 3.2% of patients who reported being known diabetics in our study. However, it is believed that the prevalence of diabetes in Kenya is under-estimated due to lack of data, especially from rural areas.24
Similar studies conducted in LMICs have found value in using a CHW-based model for CVD screening. A study conducted by Levitt et al.25 used trained CHWs to implement a non-laboratory-based CVD risk model to identify high-risk patients in Bangladesh, Guatamala, Mexico and South Africa. They found that 77.4% of patients were at low risk, 17.4% were at low to moderate risk, 3.7% were at moderate risk, 1.1% were at moderate to high risk and 0.2% were at high risk. Another study conducted in South Africa compared CHWs who were trained to use a mobile-based CVD risk assessment tool to those who used a paper-based non-laboratory risk assessment tool. Those CHWs using the mHealth tool had decreased CHW training time, decreased CVD risk screening time, and elimination of errors in calculating a CVD risk score.13 Advantages of AFYACHAT over previously described mHealth tools include the two-way interaction, allowing for data collection and rapid feedback of clinically meaningful integrated risk assessment.
Several aspects require further development and study in order to take AFYACHAT to scale. User feedback and field observations revealed some opportunities to improve AFYACHAT. Upgrades are planned for the central database hardware and power connection to eliminate service interruptions. Upgrading the CHWs cell phones could also be investigated as newer hardware with full keyboards would improve the speed of texting compared to T9 texting. Alternatives to the patient self-report for assessing the presence or absence of diabetes, including point-of-care random glucose testing, are being considered for future AFYCHAT iterations. The costs of a program, including CHW stipend, airtime, equipment and consumables (e.g. batteries for blood pressure machine) will require further study in different countries to appreciate the costs of scaling AFYACHAT. Implications and challenges of community-based screening require careful consideration. Screening for modifiable CVD risk factors may have an intrinsic value for increasing awareness and individual self-efficacy for the management of their risk. On the other hand, screening for hypertension and diabetes should go hand-in-hand with efforts to establish pathways into care and long-term drug therapy, which may be difficult in rural contexts and may have cost implications. CHWs may provide an important bridge between their community and the health facility, and may facilitate linkages to care. Remuneration models for CHWs require further study, balancing program costs with recruitment and retention of human resources for health.
Our study has several limitations. AFYACHAT represents an adaptation of a WHO risk stratification tool designed for use by trained health professionals. Validation of this tool in the community setting by CHWs using an electronic platform requires further validation against a gold standard (e.g. physician diagnosis). One element of the risk estimate was the patient self-report of a prior diagnosis of diabetes, which relies on the participant’s previous screening and knowledge of a diagnosis of diabetes. The Kenyan STEPS survey reported that only 12% of Kenyans have ever had their blood glucose tested by a healthcare professional.2 A cross-sectional study conducted by public health officials in Kenya showed that only 27% of participants had a good understanding of diabetes.25 Given the current knowledge about the lack of diabetic testing in Kenya, it is probable that our 3.2% prevalence rate for diabetes is an under representation of the actual number of those living with diabetes in the region. This may affect the overall CVD risk estimates as a diagnosis of diabetes increases the 10-year risk of a cardiovascular event. Future studies should consider random blood glucose testing on all patients to screen for diabetes. Larger numbers of communities, CHWs, and participants over a longer time frame would be needed to demonstrate the generalisability, scalability and durability of this screening tool. Measuring the clinical impact of AFYACHAT, with longitudinal follow-up of screened participants, would be an important future direction for research on this tool. Finally, the AFYACHAT tool is only one component of a comprehensive strategy to mitigate CVD risk factors; additional challenges will include sustainable funding, ensuring adherence to treatment regimens and documentation of health outcomes.
CONCLUSIONS
In this study, five CHWs screened nearly 3000 patients for the CVD risk in rural Kenya using a novel mHealth instrument. This active case-finding strategy for asymptomatic CVD risk factors combines the benefits of CHWs as cost-effective human resources for health and a scalable mHealth technology to augment their capacity and automate data collection. Further development of AFYACHAT, implementation experience and data on user acceptability and impact of the system will be needed to assess the potential scalability of the system. Nonetheless, a community-based strategy such as AFYACHAT to assess the CVD risk may represent a valuable addition to current efforts to combat the rising tide of NCDs globally.
Acknowledgements
This study was supported by Medcan Clinic, Toronto, ON, Canada. The funder had no role in study design, data collection and interpretation, or the decision to submit the work for publication.