Article Text

Abstract
Background Traditional implementations of electronic medication management (EMM) systems have involved two common formats – a ‘big bang’ approach on the day of go-live, or a phased ward-by-ward approach over months.
Objective To describe the patient-centric roll-out, a novel implementation model in converting from paper to EMM.
Method This model iteratively converted a large tertiary teaching hospital to electronic from paper medication charts, commencing the roll-out in the emergency department (ED). The tenet of ‘one patient, one chart’ was maintained with new patients commenced on EMM, while existing inpatients were maintained on paper charts until their discharge. In the second week, all other intake points commenced patients on EMM, and in the third week, all remaining patients were manually converted to EMM. The implementation was assessed with training completion rates, staff satisfaction surveys, focus group interviews and incident logs.
Results At go-live, 79% of doctors, 68% of nurses and 90% of pharmacists were trained in the EMM system. The ED converted to electronic prescribing within 24 hours; by day 20, all patients were on EMM. Two hundred and thirty issues were logged, none critical, of which 22 were escalated. Of the 51,063 medications administered, there were 13 EMM-related clinical incidents including three double dosing errors, none of which led to an adverse event or death. Overall, 77% of staff surveyed were satisfied with the EMM implementation.
Conclusions The patient-centric roll-out model represents an innovative and safe approach with a single medication chart reducing transcription and improved medication safety for the patient and the organisation.
- electronic health records
- hospital medication systems
- implementation
- medication errors
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
The transition from a paper-based medication prescribing and administration model to an electronic system represents a major change initiative for an organisation. This transition requires a whole-of-hospital change management approach, factoring current organisational culture and pre-existing models for change initiatives, while maintaining patient safety as a paramount consideration. Electronic medication management (EMM) systems represent a highly desirable functionality that is accepted by the health sector as advantageous for improving many aspects of medication safety, including medication reconciliation and cost-effectiveness.1–5
While many hospital sites, particularly in North America, favour a single ‘big bang’ delivery of the electronic medical record (EMR) and EMM at the same time, most Australian hospitals to date have implemented EMM prior to an enterprise-wide EMR.6,7 In the Australian context, this has led to long lead times for adoption and post-go-live maturity.8 In Western Sydney, the experience of implementing EMR prior to EMM had ingrained a culture of digitisation and electronic documentation. The advantage of allowing EMR to be embedded in a hospital prior to EMM improves digital literacy and reduces the risks associated with EMR adoption alongside EMM, when the latter is eventually implemented.
Roll-out strategies across the globe for EMR and EMM traditionally involve two main methodologies9,10:
‘Big bang’ – an all at once implementation across the organisation, usually activated on a single day or week. This option is likely to be disruptive to the entire hospital and would require comprehensive testing and a large training burden in a short timeframe.
Phased (or staged) – usually a ‘ward-by-ward’ implementation over weeks or months until the whole hospital is converted to the electronic system. By the very nature of this method, it necessitates a hybrid medication system – patients that move between wards will require transcription of their medications from paper to EMM and vice versa. This is a high-risk scenario for medication safety and duplicates work effort during the transition period.
Simple EMR implementations are more conducive to the ‘big bang’ approach, where clinical documentation is not complicated by medication charts. EMM implementations in Australia have so far favoured a phased ward-by-ward approach. Advantages and disadvantages of both the traditional roll-out models are shown in Table 1.
While the phased strategy at previous sites has been somewhat iterative and allowed lessons to be learnt, it has led to change fatigue within the project team as well as for end users. This phased strategy often does not begin in the emergency department (ED), which is left as one of the last wards to convert to EMM. This leads to patient admissions with paper medication charts requiring conversion to electronic prescribing in EMM wards – that is, duplicate prescribing on a daily basis throughout the transition period.
The success of EMM implementation is highly dependent on adequate support for staff during training and through the go-live period. Any intended benefits are at risk of not being realised if change management, user adoption and go-live support are poor. The use of proactive, well-informed superusers to assist in EMR change management and support in the implementation phase is a well-documented concept with significant advantages.11–13 Previous EMM sites in Australia had implemented with a baseline of 1:10 ratio in their superuser strategy. In order to empower superusers with adequate knowledge, they are required to undergo extra training, understand all aspects of application functionality and the rationale for design decisions. In the go-live phase, superusers perform better as supernumerary staff members acting as support to their colleagues while maintaining minimal or nil patient load. This project took all the experience and lessons learnt from the previous implementation sites in formulating a facility-specific superuser strategy to support the design, testing and roll-out of EMM using a patient-centric approach.
The project’s clinical reference committee and focus groups had identified that patient safety was the ultimate consideration in EMM implementation; hence, the roll-out strategy must align with this philosophy and maintain patient and medication safety as the overriding principle for its design. The tenet of ‘one patient, one chart’ was held paramount – that a patient must only have either a paper medication chart or an electronic medication chart. This led to the development of an innovative model – the ‘patient-centric’ roll-out method. The objective of this paper is to describe the rationale, method and implementation of this model for EMM roll-out.
METHODS
Location and setting
This healthcare facility is a tertiary teaching hospital in the western suburbs of Sydney, Australia’s largest metropolitan centre. The hospital is part of a health service district that serves a population of over 2 million people. The hospital has approximately 400 acute inpatient beds and has over 50,000 ED presentations annually. The hospital has several unique characteristics that differentiated it from previous EMM sites, which had a significant effect on the choice of the roll-out strategy. This hospital was a lead site for EMR implementation in New South Wales and has been a champion for digital transformation within Australia. The hospital has a highly motivated and enthusiastic clinician workforce that is keen to adopt digital change initiatives. It was the first site in Australia to have full EMR utilisation for 2 years prior to EMM implementation. A new clinical services building (commissioned in April 2016) with a 2:1 device-to-patient ratio allowed for a better state of digital readiness, not seen in previous EMM implementations in Australia. The previous EMR and other digital transformations at the hospital had largely been championed by the ED, which had led the hospital’s EMR strategy over the past 15 years. The highly supportive ED clinician workforce was both an advantage and focal point for the EMM strategy.
Patient-centric model
This model was chosen as the safest way to ensure that each patient only had either a paper or electronic medication chart during the roll-out period. The average inpatient length of stay at the hospital being 5–7 days allowed for a rapid roll-out of EMM over a 3-week period, which occurred during March 2017. Other advantages were:
Continuous (non-fractured) workflow – as patients are admitted to the electronic system, actions will be monitored for completeness ensuring no hybrid activities occurred.
A truly phased conversion with iterative learning of the new system within each ward.
Mitigation of medication safety risk from hybrid prescribing systems for each patient.
Ability during implementation to monitor the full patient journey from ED, conversion to admission, inpatient course and discharge processes.
Change champions and superusers were able to lead transitioning wards as other staff are learning or acquiring new skills (i.e. the ward is converted dynamically).
Since the EMM prescribing began in the ED, there is no need for daily duplication of medication charts.
Roll-out strategy
The patient-centric model was converted into an approved roll-out plan and endorsed by the clinician reference group as well as hospital executive staff. ‘Go-live’ refers to the point in time when the EMM system is active in the hospital and the first patient has medications prescribed electronically. The roll-out methodology (depicted in Figure 1) followed these patient-centric principles:
Patients remain on one prescribing system (either EMM or paper) throughout their hospital journey.
New ED patients entering the hospital from date of go-live were commenced on EMM.
Patients commenced on paper prior to go-live remained on paper until discharge from hospital (or manual conversion on week 3 – see below).
On week 2, all other patient entry points to the hospital were commenced on EMM including operating suite, direct admissions, intensive care unit transfers and live births.
On week 3, any patients remaining on paper medication charts (i.e. those admitted for longer than 2 weeks) were manually converted to EMM.

Superuser strategy
In implementing via a patient-centric approach, the superuser strategy was designed to ensure that competent clinical end user support would be available across the facility. To achieve this, a superuser ratio of 1:6 was delineated with these clinicians tasked with providing expert knowledge in the design, testing and support of EMM. Superuser workflow familiarisation sessions were provided to increase awareness of all design decisions and clinical workflow changes via education, training and demonstration of application functionality.
Post-go-live survey
EMM adoption and acceptance were evaluated with surveys and direct face-to-face interviews with clinical staff. A convenience sample of 206 staff was surveyed 1 month after the go-live period. The research team evaluating the adoption and acceptance of the EMM system were separate and mutually exclusive members to the project and implementation team.
RESULTS
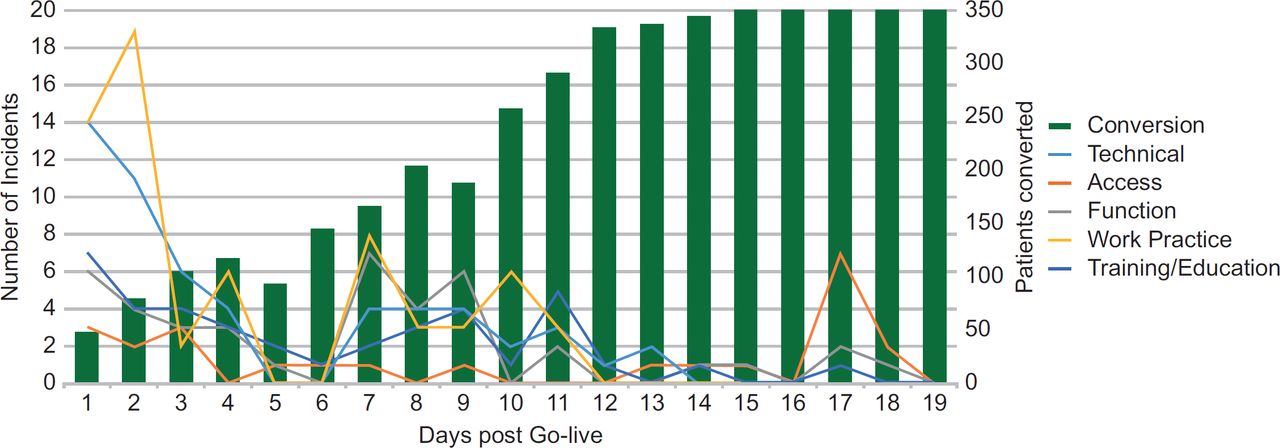
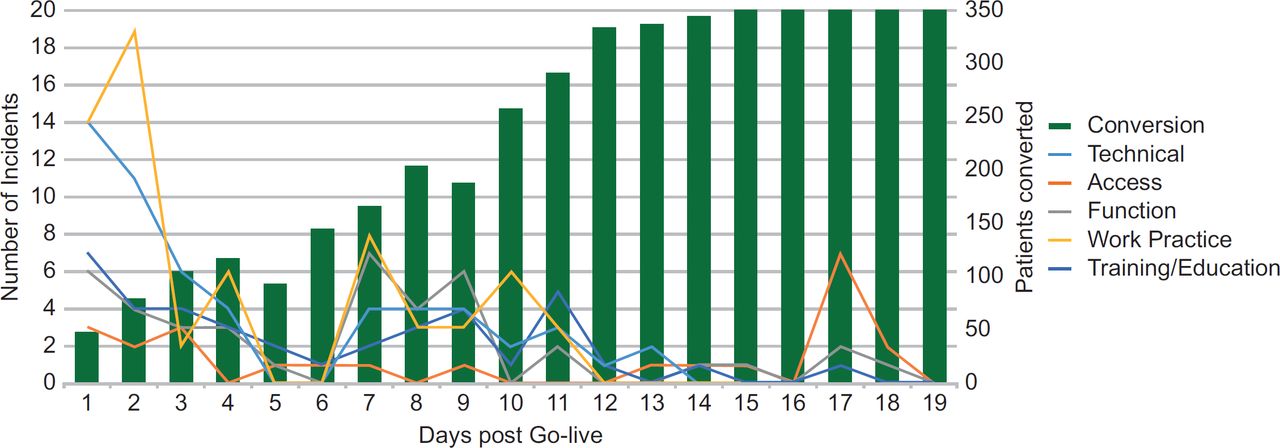
The patient-centric roll-out was readily adopted by the clinicians and hospital administration. Training was commenced 6 weeks prior to go-live, though the majority of staff were trained in the latter 3 weeks. Go-live training, superuser and incident statistics are shown in Table 2. Overall, at go-live, 79% of doctors, 68% of nurses/midwives and 90% of pharmacists were trained in the EMM system. The rate of conversion and issues logged are shown in Figure 2. The ED converted to full electronic prescribing and medication administration within 24 hours post go-live; short stay wards converted to EMM within 48 hours. One week after go-live, approximately 35% of the hospital had been converted to EMM. The second week saw all patient intake and admission points to the hospital commence patients on EMM. At the end of the second week, roughly 80% of the hospital had converted to EMM and approximately 70 patients remained on paper medication charts. The third week ushered the period of forced manual conversion of any remaining patients to EMM. This was done by convenience, when their 7-day medication chart ended and, by day 20 post go-live, all patients were on EMM. There were 230 issues logged over the first 3 weeks including 13 EMM-related clinical incidents and three double dosing errors. There were no EMM-related adverse patient outcomes or deaths.
{kind=link}
{kind=link}
Post-go-live survey of 206 medical, nursing and pharmacy staff 1 month later involved a convenience sample of 11% of the total staff trained and received a 100% response rate. This showed that an overall 77% were satisfied with the EMM system and its implementation; 14% were neutral and 9% were dissatisfied overall. Although some users (14%) found the new EMM system difficult to use during the initial implementation of EMM, many users (58%) believed their job performance was enhanced as a result of using the system. Most users (79%) found that the training provided by the project team was sufficient and useful in preparing them for EMM work practices. The majority of users (87%) found that the go-live support provided made their adaptation to EMM easier.
Staff feedback showed greater levels of clinician satisfaction with increased usage. There was a demonstrable shift from service desk calls to greater reliance on ward superusers. The first-line support was provided by superusers and the implementation team, while back-up support was provided for persistent issues via the command centre and EMR team. The success of this approach was evidenced by the decrease in issues logged over the go-live transition. During the 3-week roll-out, logged issues averaged 10 per day with the majority relating to work practice and functionality. With the transition toward superuser support, logged issues averaged one per week. The superusers maintained a log of resolved first-line issues and were able to address ongoing work practice and functionality queries.
Discussion
The roll-out experience confirms the thirst for electronic systems in the healthcare sector, albeit if the right conditions are in place. The presence of a mature EMR, device readiness and digital literacy amongst hospital staff are a recipe for a more rapid and successful roll-out of new technology and software functionality. EMM implementation is fraught with medication safety as well as a digital risk – this experience suggests that EMM systems should be implemented well after hospitals and their staff are comfortable with the EMR. A hospital with well-established use of the EMR has already overcome significant digital and change management hurdles. This allows for EMM implementation as a value-added module where staff are versed in electronic workflows and thirsty for more digital advancement. EMM itself adds pharmacological and patient risks to the equation, which is mitigated when an organisation has overcome the digital risks associated with the initial EMR conversion.
To date, big bang implementations had not been employed in the Australian context. This is largely due to the extensive training and support requirements, as gleaned from the US experience of big bang roll-outs. A sizeable workforce of change agents and go-live support for the first month of operation would be necessary. Any faults or disruptions that occur during go-live are likely to impact the entire hospital. Big bang is considered a high-risk option and requires a large number of support staff to execute the implementation successfully.9
However, with phased implementations, faults or disruptions during go-live will likely only impact upon the ward being implemented at any particular period. This model usually necessitates that ED is rolled out towards the end of the implementation, and would lead to a daily stream of patients with paper medication charts that need to be converted to EMM. The drawn-out implementation phases can lead to burnout amongst project staff and disengagement amongst clinicians.14 This strategy has the appearance of a sequential and gradual conversion for the support team; however, for each ward, it is a ‘big bang’ event on the day the ward converts to electronic, and for the whole hospital, these phases represent multiple tiny go-lives, in effect ‘a series of small bangs’.
The patient-centric approach to EMM implementation forces clinicians and support staff to own the risks of training requirements and rapid roll-out. In phased implementations, the necessity of a hybrid medication chart reduces the burden on training and support staff, while transferring this risk to the patient, who is unaware of the potential for errors in transcription and reconciliation.
Other than the pre-implementation factors that set up the hospital for a successful rapid roll-out, the realisation of a positive go-live experience was largely attributable to the superuser strategy and organisation-wide support. Early engagement with key stakeholders identified potential risks and workflow issues in advance of the go-live, and also provided an opportunity for establishing these stakeholders as change agents across the facility. A ward-specific comprehensive readiness checklist was performed to ensure that all necessary activities were addressed in preparation for the go-live. In conjunction with this approach, multiple ward-specific dress rehearsals (practice dummy runs) were undertaken to identify any potential difficulties, including walk-through practice of the downtime processes.
The support strategy provided a basis for the smooth implementation of EMM and played a significant role in driving user satisfaction during the implementation phase. For example, as indicated in the focus group interviews, the availability of support staff in each ward at all hours (24 × 7) was considered important to, and highly appreciated by, the users during roll-out. Acceptance of EMM is also aided by perceived improvements in medication management. During focus group interviews, clinicians expressed their post-go-live acceptance of benefits such as increased time saving and convenience, improved legibility and reduced medication errors. On reviewing the three double dosing errors, all were analysed to be resulting from the lack of familiarity with the system among the doctors and nurses involved in the cases. Training and education were the only interventions required and these errors were rarely seen after the initial 3-week implementation period.
While the study intervention does not have a control group, the evaluation showed a good uptake of EMM and similar adoption results to other implementations around Australia, all of which applied the phased model to date. The survey evaluation results reflect a small but representative population of the hospital which was cross-discipline and cross-seniority of staff. There is always the possibility of skewed sampling with a convenience focus group, though equally this approach may draw in the detractors as well as eager adoptees.
Despite low overall dissatisfaction (9%) with the EMM implementation, the salient issues and the level of dissatisfaction were different between the three disciplines of users (doctors, nurses and pharmacists). Only 6 out of 91 doctors (7%) and 8 out of 103 nurses (8%) surveyed were dissatisfied with the implementation of EMM, whereas 5 out of 12 pharmacists (42%) surveyed were dissatisfied. The face-to-face interviews revealed that, as in the implementation of any new electronic system, the implementation of EMM slowed down some users early on, particularly the pharmacists. Amongst medical staff, junior doctors felt that senior doctors should take on more responsibility in using the EMM system rather than leaving issues and perceived bugs for the junior doctors to sort out. Some pharmacists felt that the EMM system forced them to spend more time at a computer terminal verifying medication orders, rather than spending time with patients and clinical activities.
End-user satisfaction is a key determinant of system design and implementation strategy.15 The encouraging satisfaction survey results will be a positive factor and an important consideration in fine-tuning our strategies for future EMM implementations within our organisation.
CONCLUSIONS
The patient-centric model offers a novel approach to EMM implementation with the advantages of a single medication chart, avoiding hybrid records and reducing medication safety risk to the patient and the organisation. The combination of a digitally literate workforce and superuser support model allows for a rapid roll-out of EMM across the hospital.