Article Text

Abstract
Introduction Globally, electronic medical records are central to the infrastructure of modern healthcare systems. Yet, the vast majority of electronic medical records have been designed for resource-rich environments and are not feasible in settings of poverty. Here, we describe the design and implementation of an electronic medical record at a public sector district hospital in rural Nepal and its subsequent expansion to an additional public sector facility.
Development The electronic medical record was designed to solve for the following elements of public sector healthcare delivery: 1) integration of the systems across inpatient, surgical, outpatient, emergency, laboratory, radiology and pharmacy sites of care; 2) effective data extraction for impact evaluation and government regulation; 3) optimization for longitudinal care provision and patient tracking and 4) effectiveness for quality improvement initiatives.
Application For these purposes, we adapted Bahmni, a product built with open-source components for patient tracking, clinical protocols, pharmacy, laboratory, imaging, financial management and supply logistics. In close partnership with government officials, we deployed the system in February of 2015, added on additional functionality and iteratively improved the system over the following year. This experience enabled us then to deploy the system at an additional district-level hospital in a different part of the country in under four weeks. We discuss the implementation challenges and the strategies we pursued to build an electronic medical record for the public sector in rural Nepal.
Discussion Over the course of 18 months, we were able to develop, deploy and iterate upon the electronic medical record, and then deploy the refined product at an additional facility within only four weeks. Our experience suggests the feasibility of an integrated electronic medical record for public sector care delivery even in settings of rural poverty.
- electronic medical records
- health systems strengthening
- implementation research
- global health
- Nepal
- open source technologies
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
- electronic medical records
- health systems strengthening
- implementation research
- global health
- Nepal
- open source technologies
INTRODUCTION
The digitization of healthcare delivery systems is a pressing global need even in settings of poverty.1,2 The opportunity costs of continuing with paper systems are significant. The absence of electronic medical records (EMRs) can hamstring already challenging efforts to transform human resource management, financial accountability, healthcare systems performance evaluation, public health surveillance and longitudinal care delivery systems.3,4 Paper-based systems are human resource and time intensive and are often plagued by inaccurate reporting processes leading to out-of-date and irrelevant data.3–5 An effective EMR is an essential component of a robust and efficient modern healthcare system.3,6,7
Despite the strong evidence that adoption of health information technology leads to improved care,8,9 only recently have wealthy countries started to see widespread adoption.10 Low- and middle-income countries face additional challenges such as a lack of engineering and other technical expertise, limited funding, poor information technology infrastructure and unreliable power.2,11 Indeed, many hospital information systems that have been successfully implemented in resource-poor countries tend to be focused on specific clinical diseases rather than care integration,12 and there are only limited descriptions of such integrated systems.13
Even the most sophisticated and well-funded systems have achieved greater success in data recording, research, and program evaluation than in creating a tool that physicians can refer to during a clinical encounter.2,14 Although there have been efforts to address these challenges,14–17 successful implementation of integrated EMR systems, particularly those that are actively used by healthcare providers during clinical encounters, has been an elusive goal.
DEVELOPMENT
Possible, a non-profit healthcare organization, started in June 2014 to customize and deploy an EMR system appropriate for the Nepali public sector healthcare system. Possible works on a public–private partnership model with the Ministry of Health in rural Achham district in the far-western development region. There, Possible independently manages the government-owned, district-level Bayalpata Hospital and implements community healthcare delivery programs. Bayalpata Hospital has 25 beds and sees approximately 60,000 outpatients and 2,000 inpatients per year. Patients are seen by physicians and health assistants, a mid-level non-physician provider role common throughout Nepal.
We originally identified the following key needs as central to developing an EMR: to be simple for physicians and mid-level providers, to improve government reporting, to decrease wasteful expenditures on unnecessary medications, to use the EMR for healthcare services research, and to advance quality improvement initiatives. After some review and deliberations in the first months of 2014, Possible selected Thought Works’ (Chicago, USA) Bahmni system as its design characteristics were suited to the on-the-ground realities of Achham (Box 1).
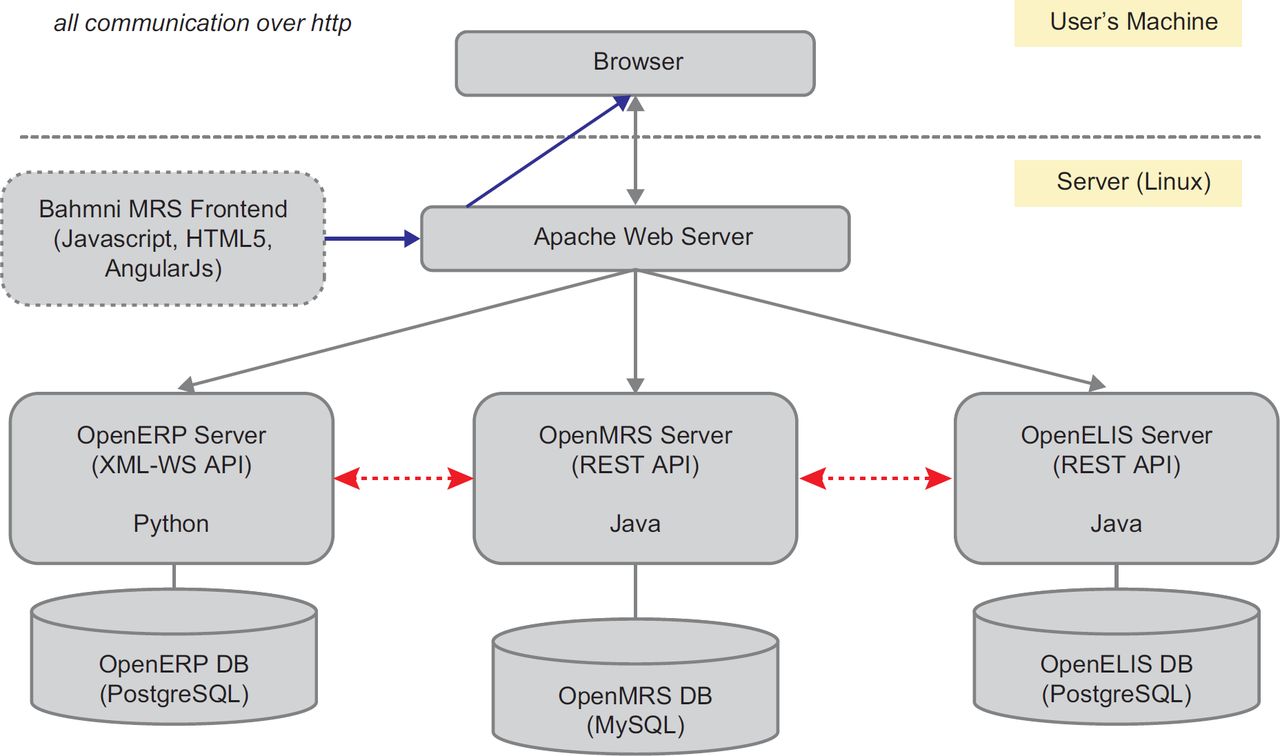
Bahmni (http://www.Bahmni.org) is an open source framework built as a javascript application on top of the OpenMRS (http://www.openmrs.org) data model and application program interface. Bahmni uses OpenERP (https://www.odoo.com/) for billing and inventory management and OpenELIS (http://www.openelis.org/) for laboratory management. Thought Works has been developing Bahmni over the last four years for deployments in India, Uganda, Haiti and other countries. We provide a diagram of the system architecture in Figure 1.

*PACS = Picture Archiving and Communication System; USG/ECG = Ultrasound Sonagraphy Test/Electrocardiography; DICOM = Digital Imaging and Communications in Medicine; ICD-10 = International Classification of Diseases, version 10
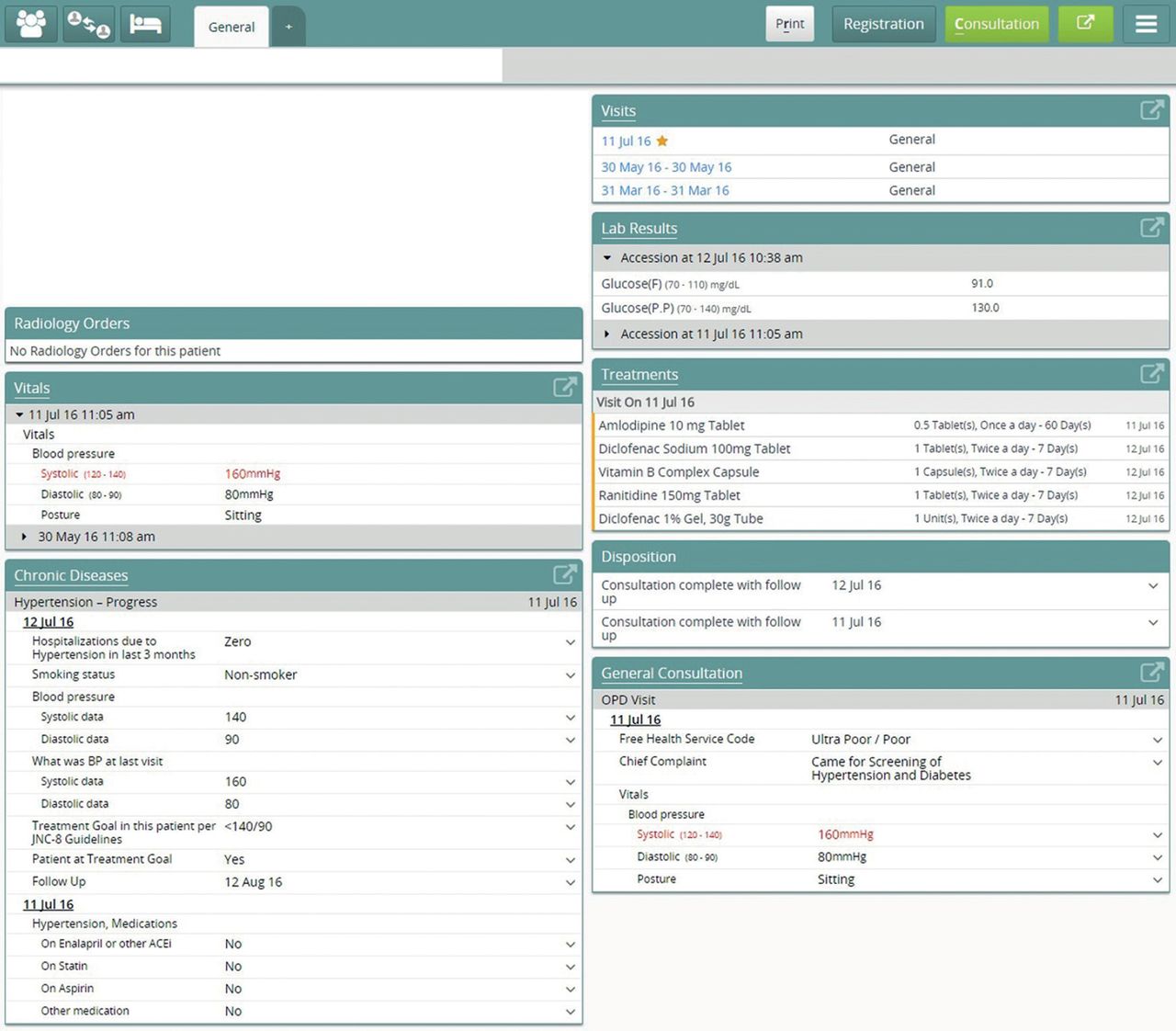
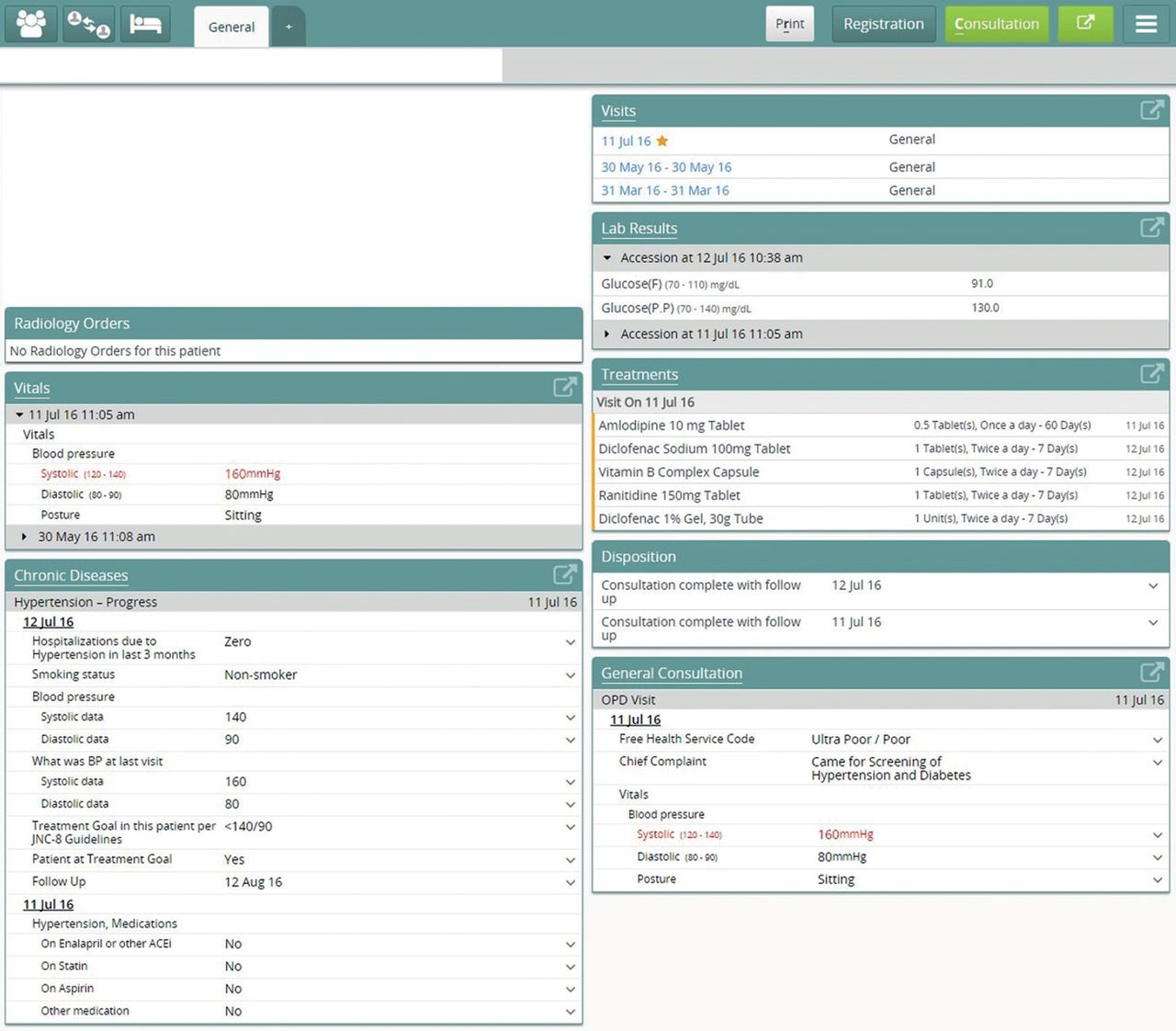
A primary innovation of the Bahmni system is that it provides a stripped-down user-friendly interface for the robust and widely used OpenMRS architecture. In a resource-limited setting such as rural Nepal, most providers have had limited prior exposure to computers or EMR systems. A well-tuned user-experience without non-essential features is thus of critical importance for providers to be able to use the EMR at the point of care without feeling overwhelmed. Workflow efficiency in the outpatient department is paramount, since Bayalpata Hospital can care for over 600 outpatients per day during peak seasons (Figure 2). Possible uses the EMR in the inpatient department for bed management, drug administration, laboratory orders and results review, progress notes documentation, and discharge planning and documentation. In the operating theaters, Possible uses the EMR to document operative notes.

APPLICATION
Bayalpata hospital EMR implementation
EMR implementation necessarily took place in a phased manner (Box 2). In preparation for the initial rollout of Bahmni at Bayalpata Hospital, a team from Thought Works came to the hospital and together with a staff trainer, trained the doctors, mid-level providers, nurses, and registration staff over a period of two weeks in July of 2014. Over the subsequent six months, we undertook several off-site and on-site design iterations and planning sessions. On 10 February 2015, Bahmni went live at the hospital with the patient registration module. The EMR was deployed to the laboratory and outpatient departments over the following week. This phased rollout allowed the deployment team to adequately support each department during the initial stage. Initially, providers were only required to enter diagnoses for patients, but over the course of time, these providers became able to review medical history and lab results, enter vitals, fill out notes, order lab tests, and prescribe medications from within the EMR.
EMR implementation timeline with 3 release phases.

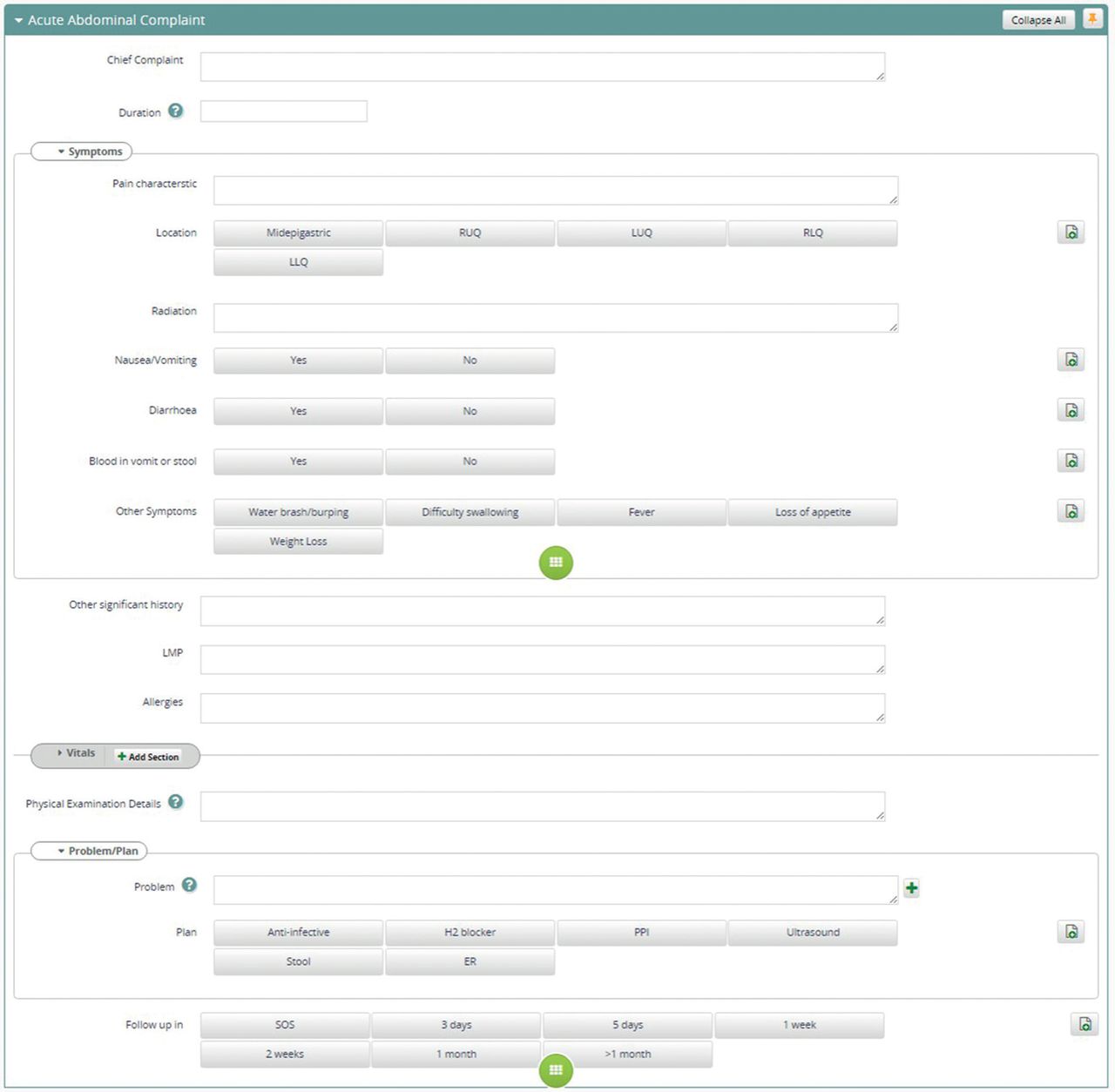
Providers access the EMR on touchscreen Chromebooks made available at all points of care. Chromebooks were chosen because they are low maintenance, inexpensive (below USD $300), and ideal for browser-based applications like Bahmni. Clinical notes have been designed to take advantage of the touchscreen functionality through use of buttons where possible for quick data entry. Unlike with electronic tablets, a physical keyboard is available when typing is required (Figures 2a, 2b and 3).

EMR response and challenges
We conducted individual focus group discussions with three different participant groups – doctors, mid-level providers and nurses – three months after the deployment of the first phase. Five doctors, thirteen mid-level providers, and twelve nurses participated in the focus groups. We held a discussion with each group that began with directed questions and ended with open discussion. Participants also completed an anonymous survey with questions scored on a scale from one to ten, as well an area for free-text comments (Table 1).
Overall, the respondents described the EMR as a useful tool that improved the hospital and had the potential of making their work easier in the future. The focus group discussions and free-text responses, however, elicited several challenges. The doctors expressed concerns that introducing a computer into the room distracted from building the patient-provider relationship. The mid-level providers and doctors raised the issue that the EMR led to extra documentation time; when the power went out, they were forced to document encounters on paper and again later in the EMR. The nursing focus group revealed that there was some confusion about documentation responsibilities and the responsibilities of nurses in documenting. Many participants expressed challenges that parallel those of others working with EMRs in wealthier countries.18,19
An anticipated challenge, one that was persistently difficult to mitigate, was regulating the server room’s temperature. The servers require maintenance of temperatures below 23°C, yet during the summer months, ambient temperatures frequently reach 35°C. This required installation of air conditioner–heater systems that have significant power needs. Like many district hospital systems, at the time of predeployment, the hospital was already operating beyond its electric power capacity. This issue caused occasional EMR down times, which challenged clinicians’ faith and patience with the system. Bayalpata Hospital addressed these issues with ongoing investments in grid improvements, solar power, generators, battery backups, and more effective load balancing. It was difficult, however, to keep up with the demands on reliable electricity throughout the roll-out period.
Human resource management and training have also been core challenges. Most of the end-users had only minimal exposure to computers and no prior experience with EMRs. Initially, users voiced some discontent about an increased time investment per patient. Becoming adept at the EMR system and to the computers themselves took focus and time away from the patient. Possible designated a staff physician as the lead clinical point person to help coordinate trainings, make announcements on system changes, and gather feedback and suggestions from the care delivery team on how to improve the functionality and interface. The use of a champion from within the clinical staff helped with encouraging, processing, and utilizing feedback from frontline providers. Over several months, the clinicians developed significant improvement in their ability to efficiently navigate Bahmni.
Following this model, Possible selected focal personnel from different departments within the hospital (e.g. nursing, surgery, mental health and pharmacy) to form an EMR-focused clinical informatics team at Bayalpata Hospital. This team meets quarterly to discuss ways to further optimize the EMR. Additionally, Bahmni and the OpenMRS development communities have created a system and culture responsive to user feedback, and as a result, Thought Works continues to enhance the user interface to make Bahmni as intuitive and efficient as possible. In order to take full advantage of the EMR system, work still remains to educate providers, habituated in paper-based systems, to write good notes and use the data for better clinical decision-making.
EMR refinement
Constant iteration is necessary in these early implementation phases to optimize the system for usability and utility, ensuring that the EMR is providing increasing value to patient care, and meaningful data for program management, evaluation, and quality improvement.
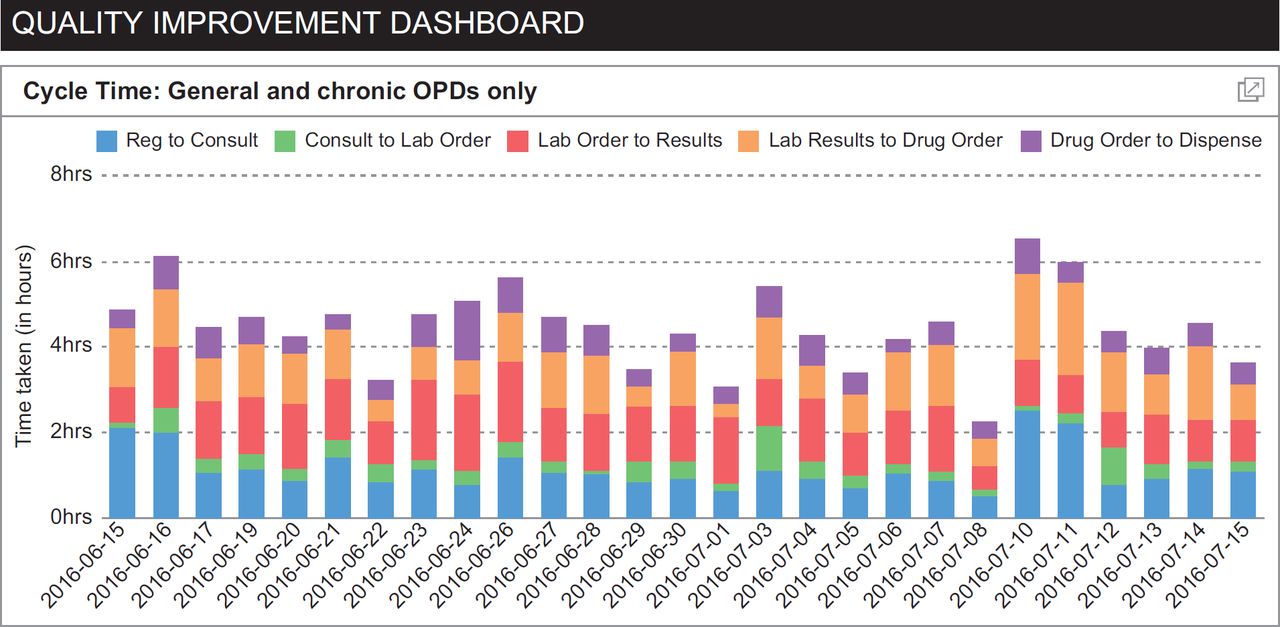
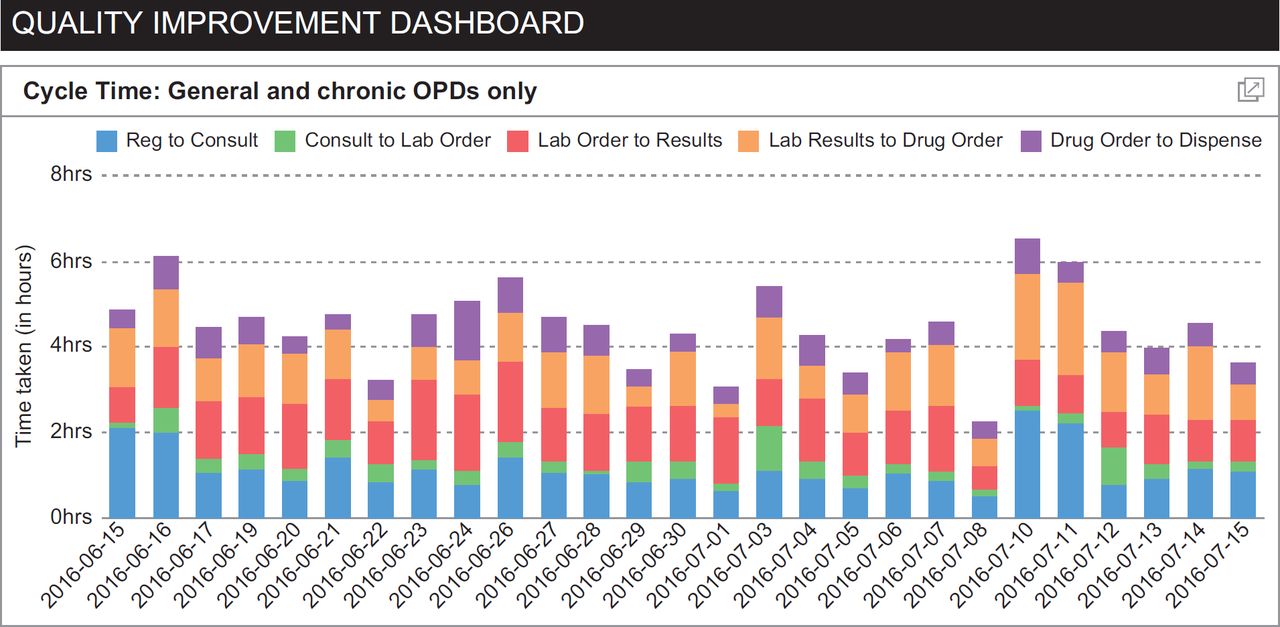
Our focus thus far has been on setting up a simple yet robust EMR system and building end-user capacity to take advantage of the system. Our efforts at monitoring and evaluation have centred on increasing EMR use and improving data quality. To this effect, we measure indicators such as ‘percent of patients who were discharged without a discharge note in the EMR’ and ‘percent of outpatients without a treatment plan documented’ (Figure 4). We also review manually entered non-coded diagnoses and perform daily data quality sweeps. These efforts continue in earnest as we are increasingly using the system to monitor indicators directly related to patient care and patient experience, e.g. we are currently refining our approach to measuring outpatient cycle time and care-to-wait-time ratios using time-stamped data pulled from the EMR in a quality improvement dashboard (Figure 5). Using data generated from the EMR, we have rolled out indicators that monitor chronic disease-specific quality metrics, for example blood pressure, glycosylated hemoglobin (HbA1c) and CD4 targets.

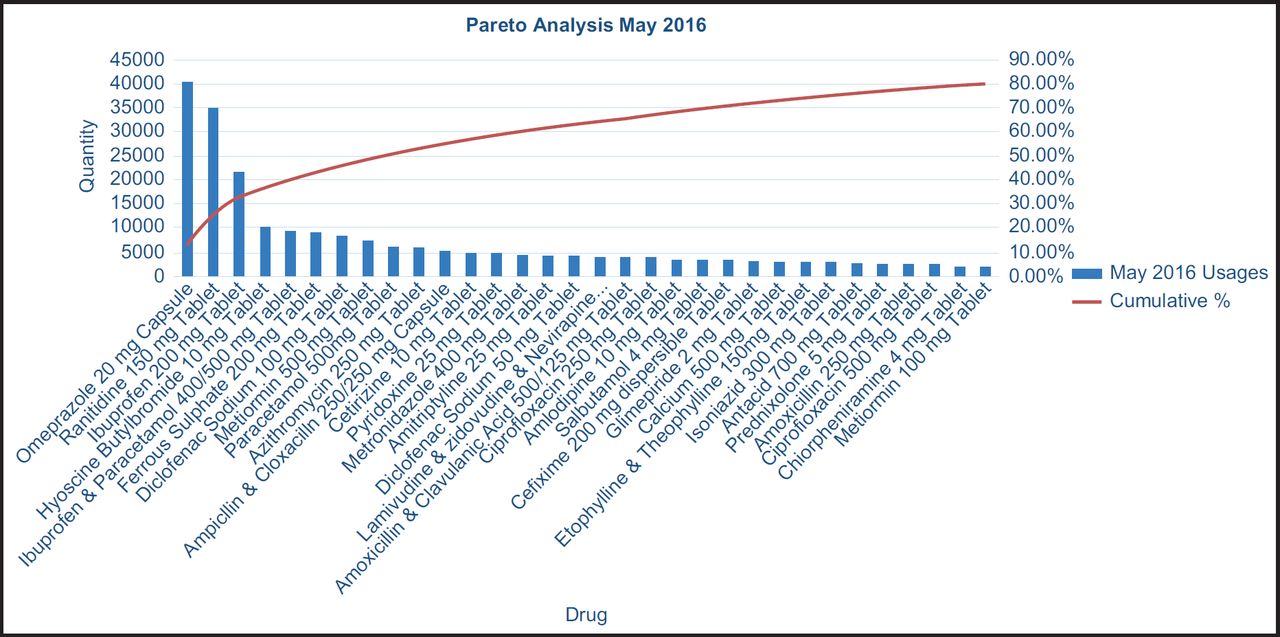
Improvement in stock management at both the supply chain and facility levels are significant advantages of the EMR. The digital platform allows us to monitor the requisition and movement of medicines and other consumables, and flexible reporting systems enable quality improvement efforts (Figure 6). For example, we measure stock out and maintenance rates as well as the percentage of essential medicines received from the government. At Bayalpata Hospital, drug orders by providers are sent directly to the pharmacy for dispensing, saving patients time, and orders are then automatically deducted from the hospital inventory.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Replication and scale
A major rationale for the OpenMRS-based Bahmni systems was that it is affordable (Table 2) and designed for the types of providers found among public healthcare institutions in South Asia. From the beginning, Possible engaged government partners at the local and national levels. Indeed, using an OpenMRS-based system like Bahmni was itself predicated on the Ministry of Health’s commitment to OpenMRS as the back-end program for its healthcare system. This engagement requires constant dialogue, as there are frequent shifts at the leadership levels within the Ministry. Policy priorities themselves have been dynamic, particularly after the devastating earthquakes on 25 April 2015 and 12 May 2015.
The national dialogue surrounding EMR standards and possibilities has been influenced by successful implementation of a full-service EMR in a rural district hospital, leading our government partners to wonder whether a similar system might be employed more broadly across government facilities. Subsequently, when Possible initiated a new public–private partnership at a district hospital in Dolakha, a district heavily affected by the earthquakes, Possible quickly and successfully deployed the EMR within four weeks.
The IT infrastructure required to host an open source EMR system like Bahmni requires initial investment in materials and expertise. In our experience, however, ongoing costs are much lower due to the availability of remote support, the lack of licensing fees since we have used open-source software, a substantial OpenMRS design and implementation community on the Web, and regional experts for maintenance of the system. These resources are available within Nepal, even in rural areas. Indeed, partly as a result of deployments in Achham and Dolakha, the government has made commitments to expand an OpenMRS-based EMR throughout the country, using private sector technology companies to deploy and maintain the systems.
DISCUSSION
We have successfully implemented an affordable integrated EMR system at two public sector rural district hospitals in Nepal. Our initial deployments have proved acceptable to clinicians, technologically feasible, and compatible with the national healthcare information system. We are now refining and expanding the EMR and making preparations for scale. Eventually, the EMR will provide both patient-level and population-level outcomes for quality improvement, health systems research, and public health surveillance systems.
Acknowledgments
We wish to express our appreciation to the Government of Nepal, Ministry of Health, for their continued efforts to improve access to healthcare in rural Nepal and for their advocacy around the use of EMRs in the public sector healthcare system. We also wish to express our deepest appreciation to our partners at the Achham District Health Office and Public Health Office and all of the allied healthcare workers serving Achham and and Dolakha Districts. These include the Female Community Health Volunteers, (Sub) Health Post and Primary Care Center staff members, and District Health Office staff members. We also wish to thank Lena Wong for her assistance in preparing the figures.
References
Footnotes
↵* Anant Raut and Chase Yarbrough are co-first authors.
Conflict of interest statement AR, BG and DC are currently employed by a nonprofit healthcare company (Possible) that delivers free healthcare in rural Nepal using funds from the Government of Nepal and other public, philanthropic, and private foundation sources. CY, DS, RS and DM all work in partnership with Possible and VV, JH and AHB worked in partnership with Possible at the time of electronic health record implementation. CY, DS and DM have been employed at two academic medical centres (Brigham and Women’s Hospital and Boston Children’s Hospital) that receive public sector research funding as well as revenue through private sector fee-for-service medical transactions and private foundation grants. DC is a faculty member and employed part time at a public university (University of Washington). VV is employed at an academic medical centre (Mount Sinai Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. VV is also a faculty member at a private university (Icahn School of Medicine at Mount Sinai). JH is employed at an academic medical centre (UCLA Medical Center) that receives public sector research funding as well as revenue through private sector fee-for-service medical transactions and private foundation grants. JH is also faculty at a public university (UCLA). AHB is a medical resident at a public hospital (Contra Costa Regional Medical Center), which receives revenue through fee-for-service medical transactions and other grants. BS was employed by Possible at the time of electronic medical record implementation and is currently employed by an academic medical centre (Patan Hospital) which receives revenue through fee-for-service medical transactions and other public, philanthropic, and private foundation sources. RS is employed at two academic medical centers (Brigham and Women’s Hospital and Massachusetts General Hospital) that receive public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. MA was employed by the Government of Nepal. DM is a non-voting member on Possible’s board of directors, but receives no compensation. RS and DM are also faculty members at a private university (Harvard Medical School). All authors have read and understood the Journal of Innovation in Health Informatics’ Ethics and Publication Malpractice Statement, and declare that we have no competing financial interests. The authors do, however, believe strongly that healthcare is a public good, not a private commodity.
Funding statement Research reported in this publication was supported by the Office of the Director, National Institutes of Health of the National Institutes of Health, under Award DP5OD019894. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Eunice Kennedy Shriver National Institute Of Child Health & Human Development and the National Institute of Dental & Craniofacial Research provided support for this award. Research reported in this publication was also supported by the Charles H. Hood Foundation. The funders had no role in the program design, program implementation, data collection and analysis, decision to publish or preparation of the manuscript.
Author contributions Designed the EMR system: AR, CY, VS, DC and DM
Implemented the EMR system: all authors
Conducted focus group discussions: AR, DC and CY
Analyzed data and evaluated the EMR system implementation: AR, CY, DC and DM
Contributed to writing the manuscript: AR, CY, DC and DM
Reviewed manuscript and critically revised content: all authors
ICMJE criteria for authorship read and met: all authors
Agree with manuscript results and conclusions: all authors