Article Text

Abstract
Objective To understand how the concept of Health Information Exchange (HIE) has evolved over time.
Methods Supplementary analysis of data from a systematic scoping review of definitions of HIE from 1900 to 2014, involving temporal analysis of underpinning themes.
Results The search identified 268 unique definitions of HIE dating from 1957 onwards: 103 in scientific databases and 165 in Google. These contained consistent themes, representing the core concept of exchanging health information electronically, as well as fluid themes, reflecting the evolving policy, business, and organisational and technological context of HIE (including the emergence of HIE as an organisational ‘entity’). These are summarised graphically to show how the concept has evolved around the world with the passage of time. The term HIE emerged in 1957 with the establishment of occupational HIE, evolving through the 1990s with concepts such as electronic data interchange and mobile computing technology; then from 2006 to 2010, it largely aligned with the US government’s health information technology strategy and the creation of HIEs as organisational entities, alongside the broader interoperability imperative, and continues to evolve today as part of a broader international agenda for sustainable, information-driven health systems.
Conclusions The concept of HIE is an evolving and adaptive one, reflecting the ongoing quest for integrated and interoperable information to improve the efficiency and effectiveness of health systems in a changing technological and policy environment.
- health information exchange
- definition
- scoping review
- eHealth
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Policymakers, health care professionals, industry groups and researchers recognise health information exchange (HIE) as a vital component of the solution to the current problems posed by disparate and fragmented health systems and non-interoperable technologies.1,2
HIE is not a new concept, but an evolving one, which to some extent ‘reinvents itself’ every 2.5 years due to the advancement in technology and changing of the regulatory environment.3,4
The report ‘Evolution of State Health Information Exchange’ prepared for The Agency for Healthcare Research and Quality yielded many significant findings about various HIE projects in terms of their designs and goals, stages of development and specific future barriers to deployment.3 The authors noted that no two HIE projects were similar, as the projects differ vastly with regard to stakeholders engaged, available finance, choice of technology, deployment strategy and community background.3 This variability makes it difficult to track the development of HIE due to variability of the HIE definitions and HIE models deployed.4 As described elsewhere in this issue (see Part 1 of the review), we undertook a detailed scoping review of existing definitions of HIE in order to develop an evidence-based concept map that may be helpful for HIE stakeholders and for improving clarity and comparability in the published literature. This paper describes the components of the analysis oriented around time to assess and map the evolution of HIE concepts.
METHODS
In this part of the review, the included definitions were thematically analysed to understand changing concepts and perspectives of HIE over time and in different global regions. First, definitions were sorted according to the year of publication. Second, definitions were thematically analysed according to their changing contexts with the passage of time.
RESULTS
Corpus of Definitions
As noted in our Part 1 of the scoping review paper, the 268 unique definitions eligible for inclusion dated back to 1957.5 Many definitions used terms synonymous with, or closely equivalent to, HIE, such as ‘Electronic Data Interchange’.6–8 ‘Clinical Information Exchange’,9–14 ‘Healthcare Information Exchange’,15–20 ‘Clinical Health Information Exchange,21,22 ‘Clinical Document Exchange’,23 ‘Medical Data Exchange’24 and ‘Information Exchange’.25 Most of the definitions (n = 240) were from the United States. Other contributing countries were the United Kingdom (UK) (n = 5),10,26–29 Australia (n = 3),8,30,31 the Netherlands (n = 3),7,32,33 Canada (n = 2),34,35 Germany (n = 1),19 Denmark (n = 1),36 New Zealand (n = 1),37 Sweden/Finland (n = 1),38 Israel (n = 1),39 Switzerland (n = 1),40 Portugal (n = 1)41 and the European Union (n = 1).42 The origins of seven definitions were unclear.
Changing definitions over time and different national perspectives
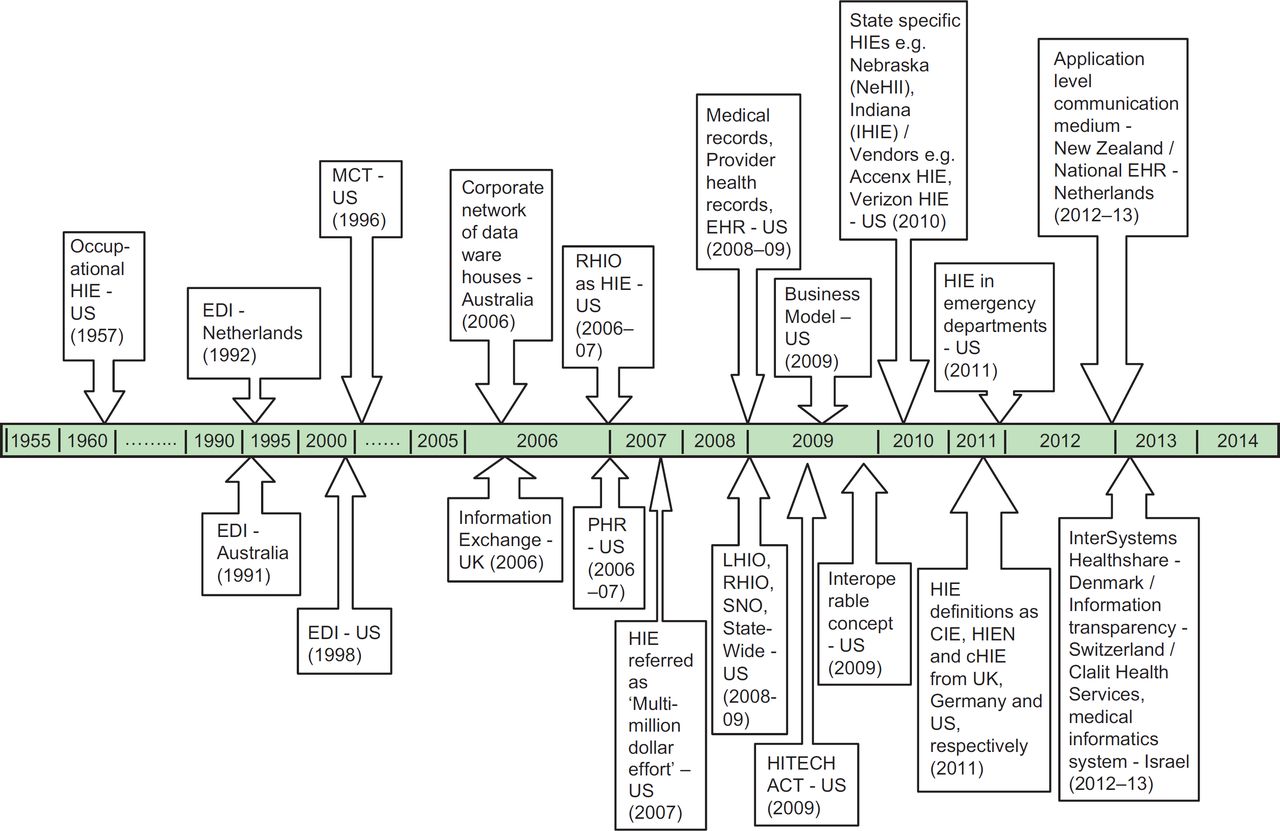
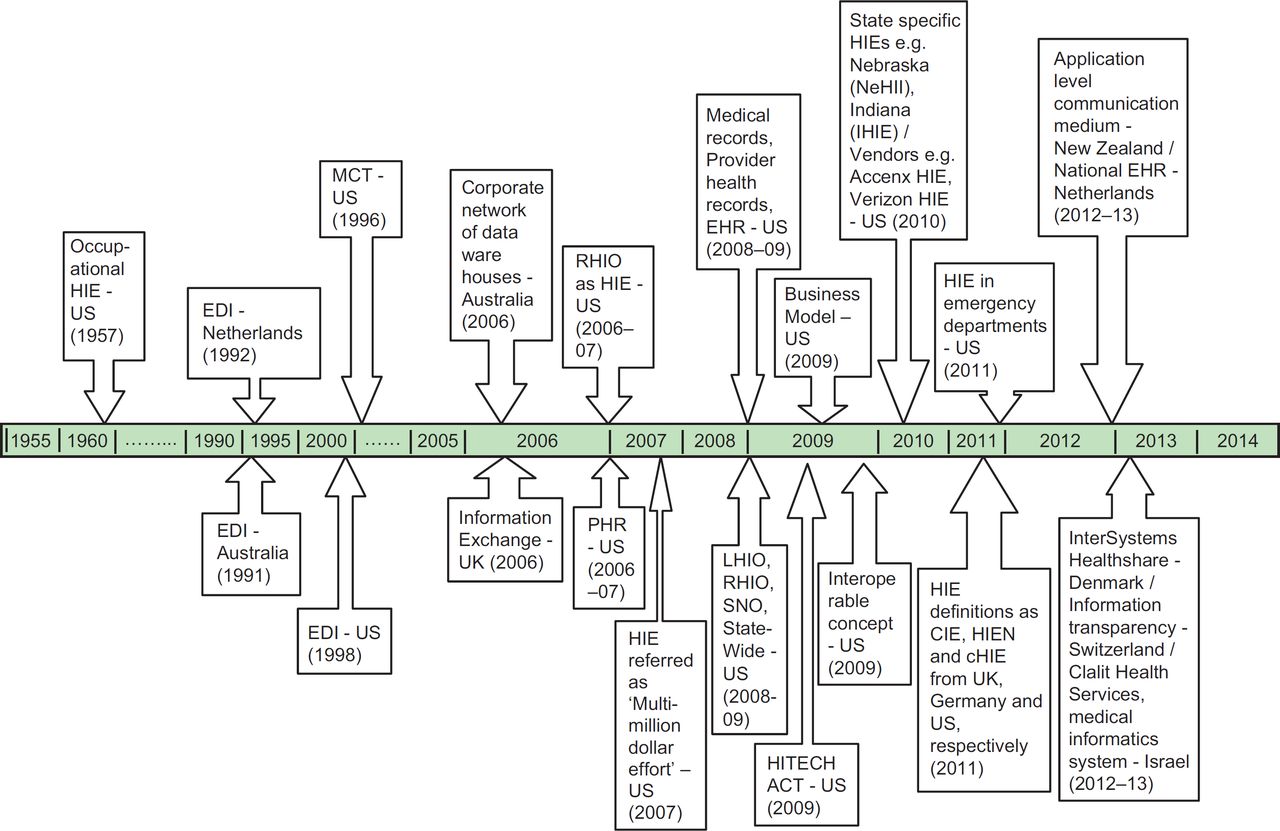
Figure 1 illustrates a timeline of the included definitions. The concept of HIE evolved with the rise in occupational health problems in the United States when Byers in 1957 recognised the need for a central coordinating organisation. Early ‘occupational HIE’ aimed to collect, collate and disseminate all types of information related to occupational health problems.43 In the early 1990s, references to Electronic Data Interchange (EDI) systems for transferring data between General Practitioners (GPs), hospitals and various other stakeholders to enhance quality of care appeared in the literature from Australia (1991),8 the Netherlands (1992)7 and the United States (1998).6 In 1996, the term mobile computing technology (MCT) began to be used in the United States to describe clinical information exchange between older cardiac surgery patients at home and health care providers to give additional information of patients’ recovery to providers after surgery.44
{kind=link}
Varying conceptual starting points: In 2006, a report from Australia defined HIE as the corporate network of data warehouses of the health department that contains data on surgical procedures, international classification of diseases, diagnostic codes, record episodes, information and diagnoses and some demographic items.30 Again in 2006, the first definition from the UK defined HIE as a process in terms of ‘information exchange’ between patients and health professional to achieve shared decision making.26
HIE as an organisational entity. Between 2006 and 2007, the terms HIEs and regional health information organisations (RHIOs) were being used interchangeably in the United States to facilitate the flow of clinical information45,46 in parallel with the concept of linking patients’ health records across organisations,47 including medical records,20 provider health records48 and HER.49 Between 2008 and 2009, the concept of an HIE as an organisational entity was becoming common in the United States, using location-specific names such as local health information organisations (LHIOs), RHIO and sub-network organisations (SNO) and ‘state-wide’, all serving the purpose of overseeing and governing the exchange of health information among different health care stakeholders.50
Funding environment: The funding environment for enabling and sustaining HIE is emphasised in a number of definitions. In 2007, a US definition described HIE as a ‘multimillion dollar effort’ and insisted on establishing a reason to sustain the effort (HIE).51 In the same year, the business case for investment in HIE was argued in terms of its potential to create productive efficiencies for the provider community.45 Another US definition from 2009 defined it as ‘a business offering services to generate revenue that must exceed its expenses and should provide services according to the expectations of stakeholders’.52
Interoperability agenda. References to the term ‘interoperability’ became more common in 200953 in a US definition of HIE along with the term ‘standardised electronic exchange’, recognising the need to manage incompatibilities between systems and software.54
Influence of the US policy/incentives environment: 48 definitions appeared during 2009–2010, all from the United States, with the exception of two from Canada, illustrating the increasing importance of HIE in North America for the two consecutive years after the enactment of the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009 and the associated attention from researchers, academicians and vendors in United States. Along with the general definitions of HIE, a number of HIE definitions are specifically associated with certain states’ and vendors’ names, for example, Nebraska Health Information Initiative (NeHII),55 Indiana HIE (IHIE),56 South Carolina HIE (SCHIEx),57 and New York Clinical Information Exchange (NYCLIX),12 whereas vendors involved were Accenx Exchange,58 Centricty HIE59 and Verizon HIE.60
Global dispersion of the concept: By 2011, the concept of HIE dispersed to the other parts of the world and the literature included definitions from Germany, UK and Finland/ Sweden. We see slight modifications of the term HIE such as Healthcare Information Exchange Network in a definition from Germany,19 Clinical Information Exchange in definitions from the UK10 and United States12 and Clinical HIE in a definition from the United States.22 A definition from the UK stressed the accomplishment of HIE through policy, infrastructure and system of care. Moreover, it further says to acquire and build computing applications and make use of financial and clinical incentives to sustain clinical information exchange. Several definitions dating from 2011 focused on the use of HIE in emergency departments, for supporting access to patient records for the purposes of out-of-hours medical care.
As the topic of HIE gained momentum, more countries, states and vendors came out with definitions in 2012–2013. New Zealand referred to it as an ‘application-level communication medium’ to exchange health information.37 Denmark, a global leader in software for connected care, has aligned the concept of HIE very much with the vendor system procured for national use, InterSystems HealthShare™.36 A definition from the Netherlands referred to HIE as national Electronic Health Records (EHR)32 while a definition from UK referred to it as ‘nationally accessible electronic records’.61 A definition from Switzerland aligns the concept of HIE with the benefits and challenges it generates, such as greater care coordination through transparency, balanced by risks of greater disclosure and the need to change the habits and practices of patients and health professionals.62 Finally, a definition from Israel identifies ‘Clalit Health Services’ as an HIE entity, which uses a single medical informatics system to exchange health information between a national network of hospitals and community care.39
DISCUSSION
The analysis has revealed the emerging nature of the field and the changing relevance of HIE to different stakeholders and contexts.
The majority of the definitions originated in the United States, no doubt reflecting the considerable investments in HIE that have characterised the government’s HITECH Act,63,64 which aims to accelerate the adoption of interoperable health information systems and integrate the health care delivery systems for the benefit of patients. This has fuelled a growth in interest in HIE amongst health care professionals, providers, payers, technology companies, policy makers and researchers.
With respect to international variations, the related terms, HIE, Clinical Information Exchange, Healthcare Information Exchange, EDI and Clinical Health Information Exchange were used mostly in the United States, whereas in the UK only HIE and Clinical Information Exchange terms were typically used when referring to the exchange of health information. HIE and EDI were preferred in publications emanating from the Netherlands, and our review found one definition on Healthcare Information Exchange Network from Germany.19
Although the term EDI was used more in the contexts of exchanging business information using a standard format, our review found two definitions of EDI, dating back to 19927 and 1998,6 that fit our inclusion criteria as describing HIE.
Organisations exchanging health information were also known by different names, such as LHIO, RHIO and SNO.50 In some cases, the terms HIE and RHIO were used interchangeably13,34,45,65,66 although RHIO typically referred to an infrastructure that enabled HIE within the health care administrative regions.39,67
The origins of various definitions lie in a range of contexts, reflecting the importance of HIE for various purposes across the health industry, for example, occupational health HIE, community HIE and HIE for public health. Most of the definitions prioritise regional or national perspectives, although a few make reference to the value of HIE on a global level.55,68,69 At the macro level, natural disasters and viral outbreaks present requirements for global monitoring or coordinated international responses, for which effective HIE is essential. For example, this was demonstrated in the aftermath of Hurricane Katrina, where health care organisations throughout the region and nationwide exchanged health information in order to take care of inhabitants displaced by the storm.70 The value of HIE in managing the recent Ebola crisis has also been described.71
Strengths and limitations
Strengths of the review include searching from 1900 to 2014, analysing a large corpus of HIE definitions and using academic databases and grey literature to find HIE definitions. Moreover, including reference of each source document and the given appendix (see Appendix A) ensured rigour of the findings.
However, we recognise the considerable progress that many countries across Europe, New Zealand, Australia, Israel and elsewhere have made in implementing national and regional health information infrastructures to support HIE, which are not fully reflected in the corpus of HIE definitions. Extending the search to related terms such as ‘national health information infrastructure’ would no doubt uncover additional definitions, and authors in the future may wish to extend the review to capture broader aspects of health informatics.
Implications for research, practice and policy
Governments become more attuned to what other countries are doing, and with major eHealth technology businesses globalising, we might expect the language of HIE to coalesce around a set of concepts. The priority according to different issues within HIE discussions may also change as more countries become involved in HIE; for example, personal health insurance and reimbursement are major issues in the United States, but in the UK and some other countries, health care is free to citizens at the point of care and funded through national taxation.
Although HIE is still in infancy, it has been on a promising track due to evolving technology and growing models of value-based payment which propose the design and functions of HIE initiatives.72 Apart from improved care and coordination, further research is required to explore the new evolving functionalities of HIE such as the availability of clinical data for public health surveillance and constructing longitudinal consumer-accessible personal health records.72
CONCLUSIONS
HIE remains an evolving concept, which due to its complexity presents challenges for developing concrete and shared definitions. It will continue to evolve mainly due to change in technology, stakeholders engaged and different paradigms of health care in different countries. In addition, the growing health care challenges around the world, such as Zika, will trigger further research to develop effective HIEs with new designs and services.
Appendix A: Extracted Definitions
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.
- 17.
- 18.
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.
- 28.
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.
- 139.
- 140.
- 141.
- 142.
- 143.
- 144.
- 145.
- 146.
- 147.
- 148.
- 149.
- 150.
- 151.
- 152.
- 153.
- 154.
- 155.
- 156.
- 157.
- 158.
- 159.
- 160.
- 161.
- 162.
- 163.
- 164.
- 165.
- 166.
- 167.
- 168.
- 169.
- 170.
- 171.
- 172.
- 173.
- 174.
- 175.
- 176.
- 177.
- 178.
- 179.
- 180.
- 181.
- 182.
- 183.
- 184.
- 185.
- 186.
- 187.
- 188.
- 189.
- 190.
- 191.
- 192.
- 193.
- 194.
- 195.
- 196.
- 197.
- 198.
- 199.
- 200.
- 201.
- 202.
- 203.
- 204.
- 205.
- 206.
- 207.
- 208.
- 209.
- 210.
- 211.
- 212.
- 213.
- 214.
- 215.
- 216.
- 217.
- 218.
- 219.
- 220.
- 221.
- 222.
- 223.
- 224.
- 225.
- 226.
- 227.
- 228.
- 229.
- 230.
- 231.
- 232.
- 233.
- 234.
- 235.
- 236.
- 237.
- 238.
- 239.
- 240.
- 241.
- 242.
- 243.
- 244.
- 245.
- 246.
- 247.
- 248.
- 249.
- 250.
- 251.
- 252.
- 253.
- 254.
- 255.
- 256.
- 257.
- 258.
- 259.
- 260.
- 261.
- 262.
- 263.
- 264.
- 265.
- 266.
- 267.
- 268.
- 269.
- 270.
- 271.
- 272.
- 273.
- 274.
- 275.
- 276.
- 277.
- 278.
- 279.
- 280.
- 281.
- 282.
- 283.
- 284.
- 285.
- 286.
- 287.
Footnotes
Funding We would like to thank the Higher Education Commission, Pakistan, and The University of Edinburgh for providing funds for this review.