Article Text

Abstract
Objective To explore the digital literacy knowledge and needs of pharmacy staff including pharmacists, graduate (pre-registration) pharmacists, pharmacy technicians, dispensing assistants and medicine counter assistants.
Methods A systematic review was conducted following a pre-published protocol. Two reviewers systematically performed the reproducible search, followed by independent screening of titles/abstracts then full papers, before critical appraisal and data extraction. Full articles matching the search terms were eligible for inclusion. Exclusions were recorded with reasons. Kirkpatrick’s 4 level model of training evaluation (reaction, learning, behaviour and results) was applied as an analytical framework.
Results Screening reduced the initial 86 papers to 5 for full review. Settings included hospital and community pharmacy plus education in Australia, Canada and the US. No studies of pharmacy staff other than pharmacists were identified. Main findings indicate that pharmacy staff lack digital literacy knowledge with minimal research evidenced at each level of Kirkpatrick’s model.
Conclusions As a society, we acknowledge that technology is an important part of everyday life impacting on the efficiency and effectiveness of working practices but, in pharmacy, do we take cognisance, ‘that technology can change the nature of work faster than people can change their skills’? It seems that pharmacy has embraced technology without recognised occupational standards, definition of baseline skills or related personal development plans. There is little evidence that digital literacy has been integrated into pharmacy staff training, which remains an under-researched area.
- digital literacy
- Kirkpatrick’s 4 level model
- pharmacy education
- systematic review
- training
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Background
Pharmacy staff across all practice settings are reliant on information technology (IT).1–4 Pharmacists, graduate (pre-registration) pharmacists, pharmacy technicians, dispensing assistants and medicine counter assistants use widely available office, retail and management information systems alongside dedicated pharmacy management and electronic health (ehealth) applications in a range of community, hospital and other pharmacy settings. The abilities of pharmacy staff to use these applications at home and at work, also known as digital literacy or digital competence or e-skills, depend on personal experience and related education and training.5–8 The British Computer Society defines digital literacy as, ‘being able to make use of technologies to participate in and contribute to modern social, cultural, political and economic life’.9 A similar definition of digital literacy is adopted in the US, ‘the ability to use information and communication technologies to find, evaluate, create, and communicate information; it requires both technical and cognitive skills’.10 Both definitions are grounded in historical and conceptual definitions of digital literacies.11
IT facilitates the provision of core pharmacy services in the UK in collaboration with other healthcare professionals with similar examples worldwide.12–15 In the US, digital literacy also forms the basis for pharmacy led health literacy as a tool for improving public health and patient outcomes.16
Collaborative working in health has been viewed as both beneficial to patients and a more efficient use of health professionals’ skills since long before the advent of ehealth.17–19 Health strategists worldwide promote the adoption of IT and ehealth to support patient care through collaborative working, which is tracked globally by World Health Organization.1–3,12,13,20–22 Both the adoption of ehealth and standards of digital literacy at home and in the workplace are key themes of interest at the international level.23–25
United Nations Educational Scientific and Cultural Organisation identifies digital literacy as both a ‘life skill’ and ‘gate skill’ because ‘it targets all areas of contemporary existence’.26 The European Commission Information Society promotes and tracks citizens’ and member states’ digital engagement.27,28 Similarly, the European Parliament promotes digital literacy for lifelong learning along with a recommendation for ‘better identification of occupational needs’.29
In the US, a government initiative to create a ‘digital nation’ recognised the role of digital literacy in promoting inclusion.23 A government commissioned report into digital literacy in Australia concluded that ‘both citizen and worker will need to be digitally literate for the digital economy to work effectively’ while a report from New Zealand argues ‘that technology can change the nature of work faster than people can change their skills’.24,25
In the UK, a range of strategic principles, national competency frameworks for training, core skills and digital literacies for the general public, and recently more specific targets for the health sector, have been developed by the government, advisory and professional bodies.30–36
Pharmacy students in the UK undertake the General Pharmaceutical Council accredited and regulated Master of Pharmacy course.5 This undergraduate university course is followed by a pre-registration year, based in practice culminating in an end of year written examination. Training for pharmacy technicians, dispensing assistants and medicines counter assistants is similarly accredited and regulated but undertaken as a combination of practical experience, college and open learning.6 Specific mention of the digital literacies required to facilitate pharmacy staff’s collaborative healthcare role is not evident in the UK curricula for initial training or their continuing professional development (CPD).37,38 The Accreditation Council for Pharmacy Education (ACPE) in America added health informatics to its standards for pharmacist training in 2007. The focus was initially on basic computer skills and then on ability to find appropriate relevant evidence base for practice.39 Pharmacy program accreditation in Canada, Australia and New Zealand make explicit mention of the need to prepare students to make best ‘use of information technology in pharmacy and more widely in health care’.40,41 While digital literacy may be covered to an extent in some initial training programmes, there is limited evidence that it features in CPD for existing members of pharmacy staff.
In summary, despite the increasing adoption of IT and ehealth to support the role of pharmacy staff, there is a paucity of research exploring their perceptions and digital literacy knowledge and related training. This review identifies evidence of perceived levels of digital literacy amongst pharmacy staff and their related training experiences and future needs.
Objective
To explore the digital literacy knowledge and needs of pharmacy staff.
Review question
This review asks, ‘What are the digital literacy knowledge and needs of pharmacy staff?’ to summarise existing evidence of pharmacy staff perceptions and measures of:
levels of digital literacy knowledge;
inclusion of digital literacy in pharmacy training;
specific digital literacy training experiences;
digital literacy training needs.
METHODS
Design
This systematic review followed the Centre for Review and Dissemination guidance for healthcare reviews (PROSPERO Protocol 2013:CRD42013005503) in seeking to ‘identify, evaluate and summarise the findings of all relevant individual studies’ and to ‘demonstrate where knowledge is lacking… to guide future research’.42,43 The theoretical framework adopted for analysis was Kirkpatrick’s 4 level model (reaction, learning, behaviour, results) for evaluating training programmes.44,45 Kirkpatrick likens level 1 (reaction) to a ‘measure of customer satisfaction’ with level 2 (learning) a ‘measure of knowledge acquired, skills improved or attitudes changed due to training’. Level 3 (behaviour) measures ‘the extent to which participants change their on-the-job behaviour’ while level 4 (results) looks for wider impact in organisational terms. Although Kirkpatrick’s model has been criticised for over-simplification and a lack of contextual consideration, its pre-eminence as a training evaluation tool has been acknowledged over several decades.46,47
Eligibility criteria
This review considered English language studies that related to any aspect of digital literacy or computer skills training for any member of pharmacy staff in all pharmacy settings with no geographical or date restrictions applied.
SEARCH STRATEGY
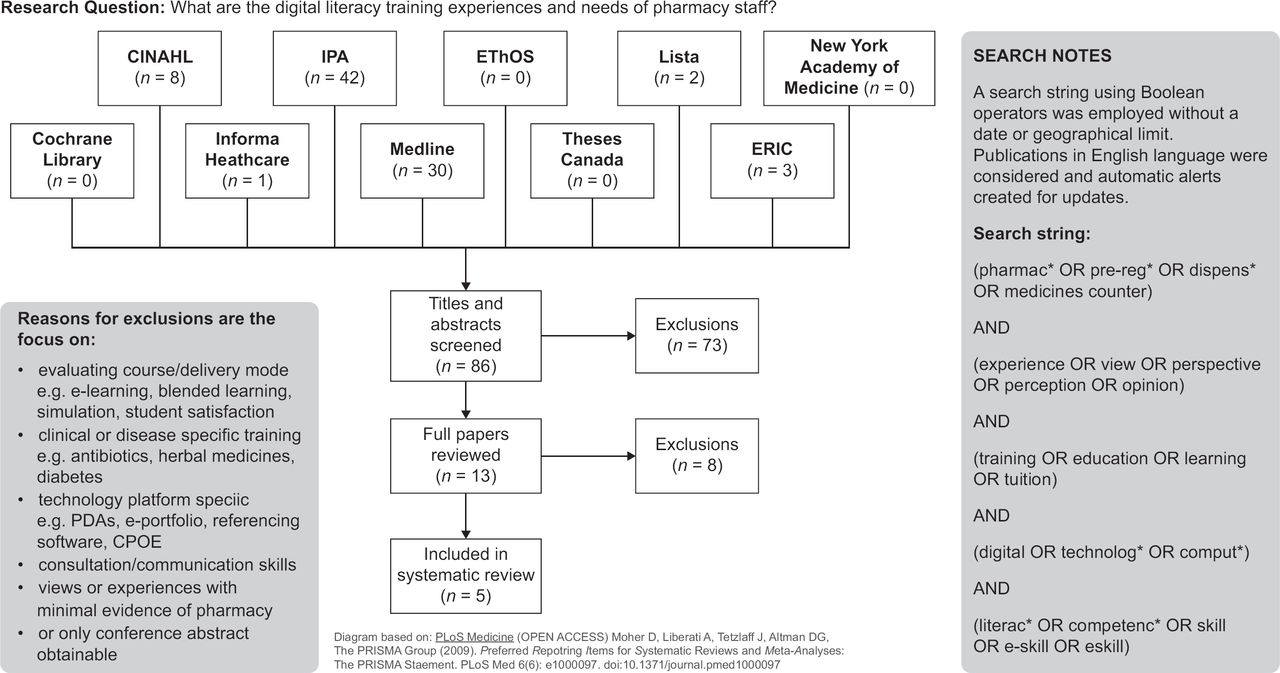
A three-step search strategy was utilised in this review. An initial limited search of MEDLINE and CINAHL was undertaken followed by analysis of the text words contained in the title and abstract, and of the index terms used to describe the article. A second search using all identified keywords and index terms was then undertaken across all included databases (Figure 1). Thirdly, the reference list of all identified reports and articles was searched for additional studies. Titles of papers were independently screened by two reviewers followed by abstracts then full papers. The search string, database returns and exclusions are shown in an adapted PRISMA diagram.48

{kind=link}
Assessment of methodological quality
To reduce risk of bias, papers selected for critical appraisal were assessed independently by two reviewers for methodological quality before inclusion using a standardised critical appraisal tool adapted to suit all study types.49
Data extraction
Data were extracted using a bespoke data extraction tool (Table 3). The data extraction was performed independently by two reviewers before cross-checking to minimise errors and reduce risk of bias.
Data synthesis
Findings were narratively explored through Kirkpatrick’s 4 level model for evaluating training programmes by focusing on evidence of reaction, learning, behaviour and results.
RESULTS
Study selection
Systematic application of the search strategy returned 86 published papers, which after independent screening of titles, abstracts and full papers was reduced to 5 (Figure 1 and Table 1).
There were no studies featuring pharmacy staff other than pharmacists and no unpublished studies identified.
Quality assessment
Each study was independently reviewed for quality by two of the research team. Details of the clarity of the research question, appropriateness of the design, description of context, population, sampling, data collection and analysis along with results, limitations and conclusions are provided in Table 2. It also details reasons for the exclusion of one study on quality grounds, while four were taken forward for data extraction.
Study characteristics
The data extraction table (Table 3) provides summarised study characteristics and contextual information. In brief, one of the studies was a survey conducted to establish baseline computer skills of hospital pharmacists in Canada prior to an educational intervention.50 Another surveyed allied health professionals (AHPs), including pharmacists, in Australia about their use of electronic evidence resources.53 A further Australian study, based on community pharmacists, combined pre-intervention focus groups with a post-educational intervention evaluative survey.51 The final study used mixed methods to review informatics content, including computer and digital literacy skills, in pharmacy education by mapping syllabi returned by schools of pharmacy against the US ACPE Standards.52
Pharmacy staff digital literacy level
Balen and Jewesson50 concluded there was not yet ‘a standard definition of computer literacy and valid dimensions of computer competency for pharmacy practice’. Based on a literature review, Bearman et al51 found ‘there was little or no information regarding community pharmacists’ skills and knowledge levels or how they currently employ internet technologies’. Through focus groups, they identified a ‘wide variety of technical knowledge and skills.’ Where access was available, participants most commonly used the internet at work for email and to search pharmacy-related topics, such as medicines or patient information, with a small proportion contributing to a pharmacy message forum. They were ‘less familiar with local health-specific portals or websites.’ Lack of familiarity or expertise and difficulty finding relevant information online were noted issues.
Balen and Jewesson50 found pharmacists were likely to have both home and work access to computers. Work use included information management, internet searching and email, drug distribution systems, patient care systems but minimal use of spreadsheets, statistical or presentation software. They concluded hospital pharmacists were ‘computer literate’ and ‘not anxious’ about using IT.
Fox et al52 identified ‘confusion within the academy/profession between pharmacy informatics and drug information practice’ and low compliance with ACPE Standards 2007 on pharmacy informatics competencies. Three progressive levels of pharmacy informatics competency were detailed under headings of terminology, systematic approaches, benefits and constraints. Fox et al52 concluded that pharmacists ‘must utilize information technology and automation’ implying but not specifying levels of digital literacy.
In a convenience sample survey of AHP, Gosling and Westbrook53 found pharmacists were the highest users of an online evidence system. Two of 25 closed questions in the survey related to database searching and computer skills. Across all AHPs, nearly three quarters reported their computer skills as good, very good or excellent with pharmacists rated most able to find online information.
Digital literacy in pharmacy training
The study by Fox et al52 focused on searching pharmacy syllabi for elements of informatics training. They cite Flynn55 in asserting ‘few pharmacy programs provide formal pharmacy informatics’. However, they elaborated the role of the Institute of Medicine (IOM) who recognise ‘utilizing the tools and techniques of informatics’ as a core competency for all clinical healthcare professionals. This is further evidenced by the initiatives around educational provision by the American Medical Informatics Association (AMIA) and International Medical Informatics Association (IMIA) whose recommendations were adopted by the American Society of Health-Systems Pharmacists (ASHP).
Balen and Jewesson50 noted that ‘informatics is not a formal component of the core undergraduate or graduate programs’ at their local university and ‘remains an uncommon component of most pharmacy and medical school curricula’ in North America. Findings from Bearman et al’s51 literature review showed that ‘many [community pharmacists] have not been educated in internet use for professional practice’. Although Gosling and Westbrook53 found a ‘marked difference between professions use’ of an online evidence system, there is no clear way to relate this back to pharmacy or other allied health professional training.
Digital literacy training experiences
Balen and Jewesson50 found that 79% of pharmacists (n =106) who responded to their survey ‘had received no formal computer training’. Following their educational intervention, Bearman et al51 received positive feedback from participants about improved searching skills and more effective searching while ‘almost half of the 93 respondents reported a change in practice’. While declaring informatics a new discipline for pharmacy, Fox et al52 emphasised the intricate link between IT and pharmacy informatics explaining ‘IT tools provide the infrastructure for information management to support pharmacy informatics’. In findings across all AHPs, Gosling and Westbrook53 identified social, organisational and professional support, along with general computer skills training, as important facilitators influencing the use of technologies in pharmacy practice.
Digital literacy training needs
Each of the included studies indicated participants want or need more digital literacy related training. Balen and Jewesson50 found that 77% (n =106) in need of ‘general computer skills upgrading’ ranking medical database and Internet search as priority areas. Access to Internet related education was viewed as a priority for community pharmacists by Bearman et al,51 while Gosling and Westbrook53 found ‘general training aimed at improving computer skills more important… than specific system-based training’. Finally, Fox et al52 recommended a set of foundational core competencies, ‘based on themes extracted from course syllabi and from personal experience’, and encouraged pharmacy educators to ‘look to informatics in other disciplines, such as medicine and nursing, for guidance’.
Applying the analytical framework
In terms of Kirkpatrick’s 4 level model, the pre-training survey of computer skills conducted by Kirkpatrick and Kirkpatrick45 and Balen and Jewesson50 evidenced baseline evaluation recognised as a preliminary activity for level 2 (learning). Similarly, Gosling and Westbrook53 conducted a survey which included measures of baseline skills (level 2: learning). Although good computer skills were shown to be associated with the use of technology by pharmacists (level 3: behaviour), it is not clear from the findings presented whether pharmacists were included in the AHPs who received training. Bearman et al51 reported pharmacists ‘were highly positive about the learning experience’ (level 1: reaction), in particular the ‘flexible delivery of the course,’ while online resource identification attracted most comments. Findings also reported ‘specific changes in practice’ (level 3: behaviour) around ‘use of new websites, more effective searching, a change to regular use of specific resources.’ The emphasis in the article by Fox et al52 was on syllabus content: which informatics skills (level 2: learning) are taught in pharmacy education. Their conclusions and recommendations aspired to levels 3 (behaviour) and 4 (results) in urging pharmacy programs ‘to prepare future pharmacists to approach their professional practice as drug safety experts and medication knowledge workers who must utilize information technology and automation in order to create a safer, more effective medication-use system’.
DISCUSSION
The evolving role of pharmacy within the collaborative healthcare team is increasingly reliant on a range of ehealth technologies and digital literacy. This review set out to summarise the best available existing evidence of pharmacy staff perceptions and measures of their levels of digital literacy knowledge, the inclusion of digital literacy in their pharmacy training, specific digital literacy training experiences, and their digital literacy training needs. Very limited research was identified about pharmacists, while no studies were found in relation to other pharmacy staff.
The need for better identification of citizen and workforce skills for the digital age is a matter of increasing focus worldwide, but there is little evidence of its impact on pharmacy education or pharmacy practice. While pharmacy programmes in America demonstrated a lack of compliance with the ACPE standards 2007, there was even less evidence of digital literacies in pharmacy programmes outside the US. So, while digital literacy is acknowledged as an important lifelong and work-based skill, this is not readily evidenced in initial pharmacy staff training nor CPD. Further research might also explain whether higher digital literacy levels amongst hospital pharmacists compared with their community-based colleagues is due to their realm of daily practice, postgraduate training or multidisciplinary team working.
The limited evidence found of digital literacy training experience was, however, positive. Improved search and basic computer skills with social, organisational and professional support were shown to facilitate the use of technologies in pharmacy. Yet, the majority of pharmacy staff had received no digital literacy training. The US leads in viewing digital literacy in pharmacy as a pathway to engaging the community in health literacy with the potential to improve social welfare, inclusion and individual health and well being.
All studies indicated that pharmacists want or need more digital literacy training, but their recommendations lack baseline data and are not current, quantifiable, measurable or specific. A key finding of this review is the lack of digital literacy research amongst not only pharmacists but all pharmacy staff as pharmacy assistants, technicians and medicine counter assistants all use technology in daily pharmacy practice. The core competencies recommended for pharmacy informatics are founded on digital literacy and so may offer a starting point for further research, which should be broadened to include all pharmacy staff. As the role of pharmacists and therefore all pharmacy staff continues to grow in the UK, the digital literacy levels for current and future pharmacists and staff must keep pace with technological change.
In launching the US 2012 Digital Government Strategy, President Obama said, ‘I want us to ask ourselves every day, how are we using technology to make a real difference in people’s lives’.56 As the role of pharmacy in healthcare continues to expand, there are calls for enhanced workforce skills, most recently from the UK Academy of Medical Royal Colleges who emphasise the need for ‘enhanced informatics skills in healthcare professionals so that the significant benefits that technology can enable are realised’.57
Strengths and weaknesses
It is a strength of this review that it demonstrates the lack of research conducted around digital literacy of pharmacy staff, but it is also its main weakness. With so few studies on which to base the review, findings must be treated with caution. Although not a weakness of this review, the survey-or evaluation-based studies used self-reporting, which is recognised for its inherent bias. The use of standardised tools in this review applied independently by more than one reviewer reduced the risk of bias for both inclusion and reporting.
CONCLUSION
In conclusion, although all pharmacy staff are reliant on technology in their daily practice, there is a lack of evidence of their specific and measurable digital literacy knowledge levels, training experience and needs. As a society, we acknowledge that technology is an important part of everyday life impacting on the efficiency and effectiveness of working practices but, in pharmacy, do we take cognisance, ‘that technology can change the nature of work faster than people can change their skills’?23 It seems pharmacy has embraced technology without recognised occupational standards, definition of baseline skills or related personal development plans. This review recommends future research should be focused on establishing what digital literacy knowledge is needed and how training should be designed, delivered and evaluated for all pharmacy staff at all levels and career stages.
Acknowledgments
The lead author gratefully acknowledges the expert input of the late Yash Kumarasamy and Professor Alison Strath to the study design and review protocol.
References
Footnotes
Competing interests The authors have no competing interests to declare.
Funding No dedicated funding was received for this review, but it is part of a larger research programme funded by NHS Education for Scotland. The authors gratefully acknowledge their support.