Article Text

Abstract
Background The use of portals might be expected to rise; however, adoption has been slow. Development of portals has occurred with limited patient involvement. This paper fills a need for literature concerning perspectives regarding the value of portals, how best to organize and provide portals and critically how to seek patient involvement in implementation.
Objective The objective was to explore the feelings, ideas, and expectations of patients and primary care providers concerning the implementation and use of patient portals.
Methods The study employed a descriptive qualitative design interviewing seven patients and four providers from an interdisciplinary primary health care clinic in Ontario, Canada. Patients were older with at least one chronic condition. Interviews were analysed independently by three coders who then met to synthesize the findings.
Results There was limited experience of portals and substantial convergence between patients and providers regarding concerns and potential benefits with an overall positive view. Four themes emerged: 1) the context in which patient portal use takes place; 2) the necessary conditions for use of a patient portal; 3) the implementation of a patient portal and 4) the use of a patient portal for care.
Conclusion Findings highlight that it is not sufficient to engage patients in the use of a portal; it is critical that patients be engaged in the early stages of implementation. With many health and fitness electronic tools available (e.g. Fitbit), this study reminds us that tools are not enough. Patient engagement requires patient-centred partnerships between patients and health care providers.
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Patient portals are one component in the broader category of personal health records. Patients may use personal health records, including patient portals to enter, retrieve and/or share their own health information; communicate with their health care providers; and better manage their health.1 An example would be a patient with diabetes who enters their glycated hemoglobin A1c values, tracks these values over time for trends, receives feedback from their health care provider and makes behavioural changes accordingly.
The unique feature of patient portals is that they are tethered to an existing information source such as an electronic medical record (EMR). Evidence on the relationship between patient portal use and health outcomes as reported in four review papers is equivocal.2–5 One paper reviewed only RCTs and found no evidence of improvement in health outcomes.2 Two systematic reviews3,5 found mixed results with some reviewed studies reporting improved patient outcomes such as lowered glycated hemoglobin A1c values3 and other studies reporting no clinical benefit.5 The review of the RCT studies2 and two systematic reviews3,5 found mixed results for process measures such as both decreases and increases in office visits. A fourth paper utilized a realist review and found some evidence of improved clinical and process outcomes.4
The use of patient portals might be expected to rise as a result of the increasing availability of EMRs and consumer interest in conducting their lives online (e.g. health information, banking and socializing). However, patients have been slow to adopt portals and many do not see their value, especially when portals have limited functionality and require them to enter data.6 Patients who see the value tend to be those with chronic conditions, the elderly and those who care for these patients and parents of young children.7 Research supports the focus of portals on capturing clinical information and feeding it back to the patient,8–10 but the system impact is limited by the low adoption rate.
Patient portal development has occurred with limited patient involvement. Therefore, this paper seeks to inform more patient participation in the design, implementation and utilization of patient portals.6 Such a patient-centred approach may lead to increased buy-in. This paper fills a need for literature concerning patients’ perspectives regarding the value of patient portals, how best to organize and provide portals and how to seek patient involvement in the process.11
In Canada, the health care system is funded federally and provincially through tax revenues and the health care systems are generally managed provincially. Publicly funded services are available to citizens such as visits to physicians and hospital and emergency department services. Some people have additional private or workplace-provided insurance that covers other services such as dental services and physiotherapy. Currently, the Ontario government does not cover the costs of access to patient portals.12,13 The objective of this pilot study was to explore the feelings, ideas and expectations of patients and primary care providers concerning both the implementation and the use of patient portals.
Methods
Design, setting and participant recruitment
The study employed a descriptive qualitative design.14 A purposive sample of 11 participants from an interdisciplinary primary health care clinic in the province of Ontario, Canada, was identified. The seven patients, six of whom were 50 years or older, had at least one chronic condition including diabetes, hypertension, asthma, obesity, COPD, thyroid condition, hyperlipidemia and cancer. The four providers included two family physicians, one nurse practitioner and one family practice nurse.
Data collection
Data were collected through individual semi-structured interviews lasting on average 30 minutes. Interviews were audio-recorded and transcribed verbatim to promote trustworthiness. Before beginning, the interviewer (BLR) checked for knowledge of patient portals, and if necessary provided a brief explanation: ‘A patient portal would be connected to your provider’s electronic medical record and allow you to see parts of your record. You may be able to input information or communicate with your provider using the portal’. The limited familiarity with patient portals was acknowledged and participants were invited to imagine how they might interact with patient portals. Table 1 contains the interview questions for patients and providers.
Data analysis
Three researchers (BLR, JBB and AT) identified independently initial line-by-line codes corresponding to salient topics found in each interview transcript. They then met to compare coding for each transcript. A coding template evolved over the course of these meetings. They met twice subsequently to further synthesize codes into themes and identify exemplar quotes. Saturation of themes was reached. Particular attention was paid to any differences that might arise among themes for patients and providers. However, no themes arose only in the patient or provider groups; therefore, illustrative quotes are reported here from both patients and providers.15
Results
There was limited first-hand knowledge of patient portals among patient participants. Some made connections between patient portals and having used a portal at work or doing online banking. Providers had more knowledge of portals but no direct experience. Some participants talked about their current use of e-mail communication (between patients and providers) and made connections to how that might work in a portal.
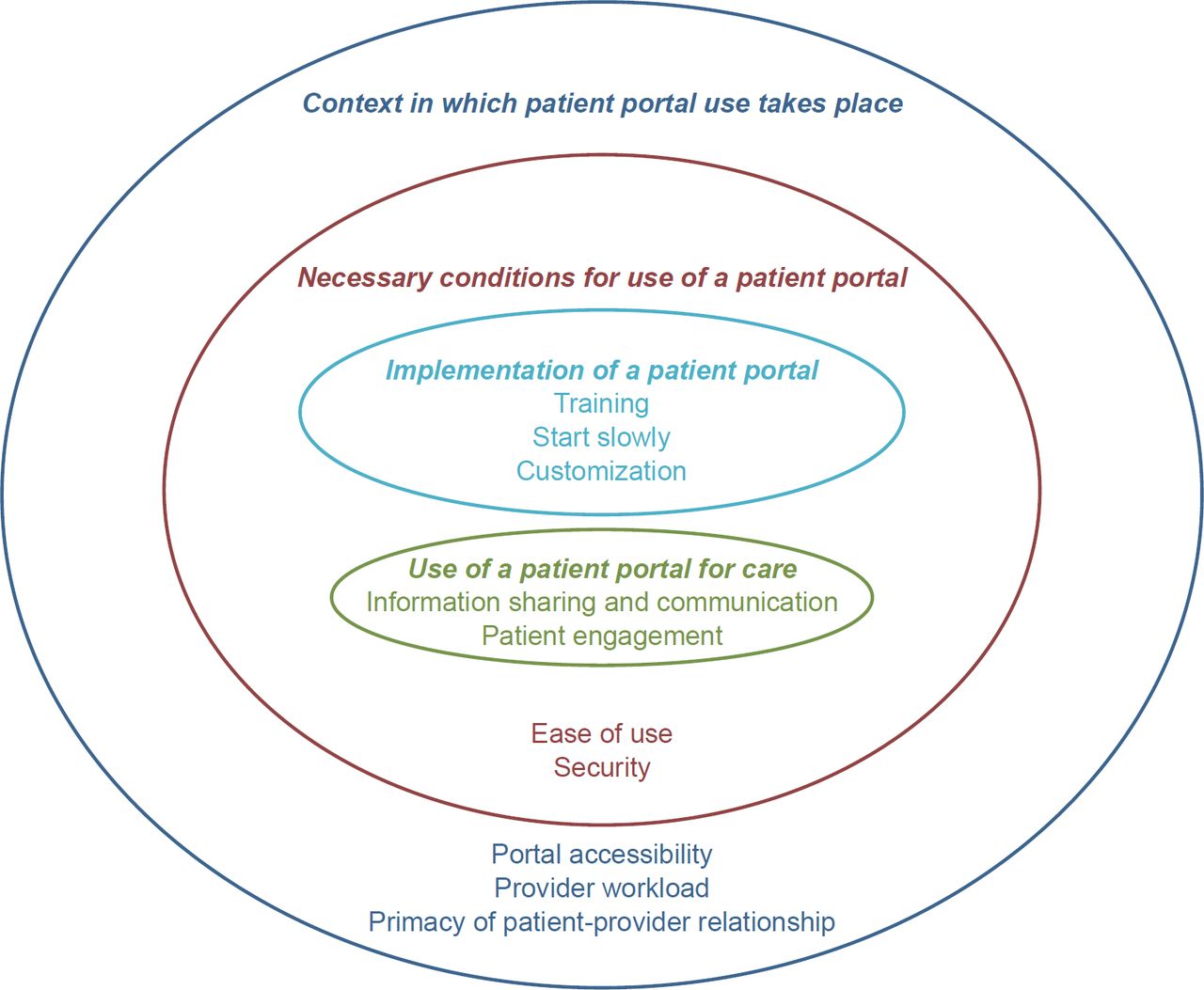
There was substantial convergence between patients and providers regarding concerns and potential benefits of patient portals with an overall positive view. Four broad themes emerged from the data: 1) the context in which patient portal use takes place; 2) the necessary conditions for use of a patient portal; 3) the implementation of a patient portal and 4) the use of a patient portal for care (Figure 1).
{kind=link}
Theme 1: context
Context included three subthemes: portal accessibility, provider workload and the primacy of the patient–provider relationship. Context was seen as being influenced by portal use (e.g. effect on patient–provider relationship) and influencing portal use (e.g. costs might prohibit use). Context was framed either positively or negatively. When negatively expressed, it was usually an issue to be grappled with, rather than an insurmountable barrier.
The first subtheme of accessibility to patient portals arose with respect to two related issues – computer literacy and the cost of portals. Participants worried that those who are not computer literate may be patients most likely to benefit from this technology but least likely to be able to access and understand it: ‘I don’t think I would have too much of a problem [using a portal]…but I think a lot of people would have problems’. – Patient 1.
Currently, patient portals are generally paid for by the patient. This could pose additional barriers and potential inequities for patients who cannot afford to pay: ‘[Sicker patients] may be the ones that can least afford a fee, but may have a very huge benefit from [portals].’ – Provider 1. However, providers and some patients felt that it was appropriate for the patient to bear the cost: ‘[Portals] better not have a [financial] impact on the health care system’. – Patient 7.
In the second subtheme, patients and providers identified potentially positive and negative effects on provider workload. A provider suggested a positive effect included improving work flow: ‘…You play phone tag... and it gets very frustrating on both ends…it could be much more efficient to communicate electronically’. – Provider 3.
Patients expressed concerns about the amount of time it would take providers to review communications: ‘It would just add one more thing the nurses have to deal with’. – Patient 2. However, most participants felt that with appropriate training and guidelines this could be avoided. One provider likened it to the current telephone system: ‘…patients don’t expect that I’m going to answer the phone. The same needs to be built into portals… maybe it’s the receptionist, the nurse who triage…sometimes questions to me’. – Provider 1.
The third subtheme under context was the primacy of the patient–provider relationship. Patients and providers expressed that like other tools, portals will be effective in so far as they are used within a positive patient–provider relationship. One patient captured this succinctly: ‘We don’t want to replace our wonderful health care professionals with just machines’. – Patient 7. Participants imagined that patient portals would be part of their health care, not a substitute for in-person care: ‘…the face to face…should still be available’. – Patient 1; and ‘You have to make sure the relationship is going to be established first. I wouldn’t “portal” with [just] anybody’. – Provider 2. Participants also emphasized that portals require trust and honesty. A patient stated: “it may be possible [to record my weight at home], it’s an honour system.” – Patient 7. A provider stated: ‘…the trusting relationship can grow electronically… but I think it takes a lot of sensitivity on the provider’s part’. – Provider 3.
Theme 2: necessary conditions
Necessary conditions included two subthemes: ease of use and security. All participants highlighted ease of use: ‘It would have to be dead easy; yeah it would have to be very simple’. – Patient 5.
They also expressed the need for security. Security was not described as a barrier but as the usual condition surrounding all on-line interaction: ‘When you do anything through a portal, even secured, people have to realize what they’re saying yes to’. – Patient 2. A provider stated: ‘Well certainly privacy is one [concern], it’s huge’. – Provider 3. Another patient expressed a common view that the transfer of information across providers should be limited: ‘If you go to a specialist, he shouldn’t have all the knowledge, he should only be limited to what he’s dealing with’. – Patient 1.
While overall computer security was mentioned, participants focused to a greater extent on confidentiality with respect to who has access to the portal: ‘I guess it’s a privacy issue, but it just makes sense that I would be the one who has access to it and nobody else’. – Patient 4. A provider stated: [Patients will ask] ‘Can I get into the portal of my kids, my husband and the only person…that can engage in their chart should be the person’. – Provider 4. Further, providers questioned their fiduciary responsibility: ‘Does [the provider] actually track…where the legal responsibility lies for making sure the [family member] has power of attorney?’ – Provider 1.
Theme 3: implementation
Participants were asked explicitly how providers might engage patients in the actual implementation of a patient portal, helping providers decide what and how to use a portal. Patients had difficulty identifying how they might assist in portal implementation and seemed surprised to be asked their opinions. In spite of this, both patients and providers were able to offer ideas of how portals should be implemented with three subthemes emerging: training, start slowly and customization.
While ease of use was described under Theme 2 as a necessary condition, participants still expressed the need for training as essential to successful portal use: ‘Don’t just hand [patients] the portal and expect them to go on their own, train them’. – Patient 1. It was also recognized that on-going support may need to be available: ‘[Patients may ask] what if I have problems that I can’t access that [portal feature]… who’s going to be my IT support’. – Provider 2.
Regarding the second subtheme of starting slowly, one approach was for practices to start by targeting specific patient populations:
Start small, make it available to people with diabetes first. Set up a pilot project [maybe] 50 patients. Monitor it, see how easy it is, unless you…start using it you don’t know how easy it is going to be. – Patient 7.
Another strategy was to start slowly with only a few functionalities: ‘Start with opening a couple of the areas…maybe just blood work first’. – Provider 2.
The third subtheme was that portal use needs to be customized for each patient. One patient expressed that each patient–provider dyad should have a conversation about how they would together use the portal:
[The portal] is going to be custom tailored to each person… it doesn’t need to be a long process. [Doctor would say] ‘Here’s the things that we can do. These are things I think would work for you, are there any other things that you’d like to have access to?’ [My provider] and I could [in] five minutes between us, figure out what would work. – Patient 4.
Within customization, providers expressed that clinicians need to show leadership in portal development: ‘What sort of things you’re going to implement…let the patient know this [feature] is or isn’t [available]… because the patients are going to have a wide variety of expectations’. – Provider 1. During implementation, portals should be discussed like any other management decision: ‘It would go back to any treatment or investigation decision … explain to the patient, know what is the potential benefits and detractors, and then see if they actually want to do it’. – Provider 1.
Theme 4: use of a patient portal
Use of a patient portal included the two subthemes: information sharing and communication and patient engagement. Regarding information sharing and communication, any mechanism that allows patients to obtain more information about their health was viewed positively by patients: ‘I think that’s the age we’re in now, people want to know…control their life a little bit more if they know things…just that sharing of information is real important’. – Patient 4. Some providers echoed the value of information in and of itself: ‘…the age that we’re into is everybody wants information and they want information quickly… So a lot of people realize the value in having information about themselves to make decisions for their health care…’ – Provider 1.
Specifically, patients and providers tended to refer primarily to accessing lab results. Patients and providers alike worried about the best way to communicate bad news concerning test results as well as the inability of patients to understand and interpret what they are seeing. A patient stated: ‘…if [the portal] was developed…keep everything…in everyday language because I find…that if people don’t have all the information or education…they can take things out of proportion’. – Patient 6. And a provider expressed: ‘…knowing the patient who’s using the portal and whether or not they would have an understanding of the record. There are some patients I wouldn’t want using portals because it may be more alarming for them’. – Provider 3.
While providers saw benefits to patients entering information into a patient portal, there was concern about maintaining a medical record.
…it would be good for patients to send us information [such as address changes]… [but] you don’t want them fiddling with the history, they can dispute it…but I want my record… to look the same as what I put in there… – Provider 4.
The second subtheme was that portals could facilitate the engagement of patients in their own health and health care. A provider stated: ‘[It’s] a shift to people being part of their care and helping to make the decisions, so they need the information to actually be more of an active participant in their health care plans’. – Provider 1.
Patients were asked directly about inputting their own information into the portal and indicated an interest in inputting clinical values into the portal for information that they track at home: ‘…keeping up to date with my progress…if I was able to input blood sugars…would benefit my health practitioners… I think that would be beneficial to keep everyone in the loop about what’s going on with me’. – Patient 6. Some participants saw using clinical information from a patient portal as a way of monitoring the patient’s condition over time: ‘The most useful thing for me would be to look at the lab reports, quarterly…I would like to see those. I would like to see probably prior ones, maybe going back for a number of years’. – Patient 3. Patients were also interested in knowing where they stood against other patients and clinical norms: ‘I don’t want to just see my own records but I want to be able to compare myself to other people with the same condition… see what the general population with diabetes was achieving’. – Patient 3.
Discussion
This qualitative study found convergence between patients and providers regarding concerns and potential benefits of patient portals with a generally positive view of portals. Participants raised issues not only in their personal interest but in the interest of the other group of participants, for example, patients expressed concern that portals should not increase workload for providers.
The patients in this study were older with at least one chronic condition. This sample was chosen because research indicates that this population is interested in using patient portals.7 While this may limit the transferability of the findings to younger, healthier populations, it is important to understand these patients’ perspectives because they may be the early adopters of this technology. The positive views expressed by older patients is consistent with recent literature16 mitigating previous concerns that older people will not be able to make use of portals.17 A study by Kerns et al.18 found that patients’ trust in a personal health record was related to its recommendation by their clinician. The importance of trust is echoed in our finding that participants see the portal as only valuable within the context of a solid patient–provider relationship.
With respect to using portals, patients identified that more information about their own health was beneficial in and of itself. Patients talked about the ways they might use information, comparing their own information over time or themselves against norms. Implicit was the notion that this might lead patients to make changes to improve their health. Patients and providers expressed that using a portal should involve two-way communication with some caution expressed on how information is input and retrieved by patients. In contrast to the findings from Kerns et al.18, where participants wanted to share information seamlessly across all health care providers, patients in our study were reluctant to allow access to their portal by anyone other than their primary care provider.
Despite the small sample size for this study, saturation of themes was achieved across the patient and provider participants. However, this study may be limited in the transferability of its findings to a setting outside of the province of Ontario and, as mentioned above, in populations that are younger and healthier. Settings where portals are provided without charge to patients may find different perspectives, for example.
The findings from this study highlight that it is not sufficient to engage patients only in the use of a portal; rather, it is critical that patients be engaged as partners in the early stages of portal implementation. When asked directly, patients offered constructive suggestions on implementation, but they first seemed surprised that their opinions were being sought. Therefore, patients will need to be encouraged to see a role for themselves in the process of portal implementation. This role might include being part of an advisory group that informs the implementation and evaluation of the portal from the outset. Patients can also take part, alongside providers, in the actual piloting of the portal, providing feedback that informs improvements to portal processes.
It is important to understand the engagement of patients in patient portals in the context of the current market for health and fitness solutions and applications. Solutions such as HealthVault in the United States and Telus Health Space in Canada offer patients ways of organizing their health and health care data. A number of applications such as Fitbit and Apple Watch offer healthy goal setting and monitoring. There is limited research evaluating these solutions.19,20 While it may be that these tools are useful, the findings from this study remind us that tools alone are not enough. Engagement in their own health, especially for those with chronic conditions, requires a patient-centred partnership between patients and health care providers.
Funding Acknowledgement
The authors would like to acknowledge the support of the Ontario Ministry of Health and Long-Term Care Primary Health Care Program Seed Funding. The views expressed in this paper are those of the authors and do not necessarily reflect those of the Ministry.
Dr. Ryan is funded by the Canadian Institutes for Health Research Community-based Primary Health Care Innovation Team, Patient-centred Innovations for Persons with Multimorbidity. Dr. Stewart is funded by the Dr. Brian W. Gilbert Canada Research Chair in Primary Health Care Research.