Article Text

Abstract
Background Personal health records (PHRs) are tools that allow individuals to access, share and manage their health information online. Despite apparent interest, adoption rates remain low. There is a gap in our understanding as to what different populations of users, in particular young adults, might want from such a tool.
Objective To describe and interpret the views and expectations of young healthy adults about using an online PHR.
Methods A qualitative descriptive study was carried out. Four focus groups were conducted with a total of 29 participants (18–34 years old) from a community setting in Montreal, Canada. Interviews were transcribed and analyzed with inductive thematic analysis.
Results With respect to how young adults viewed PHRs, three broad themes were identified: perceived advantages to using a PHR, future PHR users and concerns about PHRs. Three other overarching themes emerged from data analysis in terms of what participants expected from using a PHR: the use of the PHR for preventative health, PHR support to take more control over their health and strategies to make the PHR worthwhile. A conceptual framework of factors influencing expectations of PHR use in this population is proposed.
Conclusions While young adults view the PHR as beneficial, this is not enough for them to be motivated to actually use a PHR. To foster use, the PHRs need to be perceived as a health prevention tool that helps users to increase control over their health status. More research is needed to understand the expectations and anticipated use of different populations in designing a person-centered tool;the proposed framework provides theoretical basis in this regard.
- health information technology (HIT)
- personal health records (PHRs)
- primary care
- primary prevention
- qualitative research
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
- health information technology (HIT)
- personal health records (PHRs)
- primary care
- primary prevention
- qualitative research
Introduction
Health information technology (HIT) is widely considered as an important part of the solution to address health care challenges and modernize the health care systems.1–4 Personal health records (PHRs), in particular, have garnered considerable interest and investment in recent years, in both the public and private spheres.3,5,6 PHRs are tools that allow individuals to access, share and manage their health information online. Seen as patient-centered and patientinitiated, they are thought to have the potential to promote patient self-management and greater involvement in their own care.4,7–11
Despite public interest in using a PHR and a proliferation of available options, adoption rates remain low.12–15 There is a gap in our understanding as to why people are choosing to use or not use PHRs. In line with Rogers’ Diffusion of Innovation Theory, in order for PHRs to be self-sustaining as an innovation, there must be enough adoption for it to reach critical mass.16 The technology acceptance model (TAM), which looks at how users come to accept and use a technology, suggests that perceived usefulness, or “the degree to which a person believes that using a particular system would enhance his or her job performance”, and perceived ease-of-use, or “the degree to which a person believes that using a particular system would be free from effort,” are key factors influencing adoption.17 PHRs, in particular, differ from other forms of HITs in that they are user-driven and require an even larger involvement and motivation on the part of the user, as opposed to the health care provider and/or system. So in that view, both perceived usefulness and ease-of-use from the perspective of the user would have to be high to ensure adoption. The discrepancy between apparent interest and actual adoption may lie in not adequately understanding and incorporating the views of end users in what is meant to be a patient-centered tool.11,18,19 Successful adoption of PHRs requires the perception of inherent value as well as a fit between the technology and the wants, needs and characteristics of the end user.18,20,21
PHR studies have generally looked at the older and chronic disease population, largely where PHRs were offered through patients’ health care providers.18,22–28 Furthermore, existing research has mainly focused on the use of PHRs for managing existing health conditions, but little consideration has been given to the potential role of PHRs in prevention strategies.29 Targeting PHRs beyond the chronic disease population could yield the necessary critical mass for more widespread adoption. Young adults, in fact, are an understudied group that represents a potential target for prevention and/or early intervention strategies with PHRs. Though this age group does not currently bear the main burden of chronic disease, evidence suggests this may change.30–32 Most young adults are still healthy and many do not have any major health issues.33 As a result, this population does not necessarily access health care services on a regular basis and may face challenges in terms of continuity of care.34 For those with childhood diseases, transitioning to adult care can likewise contribute to gaps in care. PHRs could thus represent a useful tool to facilitate access and information to a hard-to-reach population at a point where encouraging greater sense of involvement and effective ownership over their own health could translate to better health outcomes in the future.2 Little is known about what issues may affect PHR adoption in this population. In order to fulfil these knowledge gaps, we aimed in this investigation to answer the following research question: What are young health adults’ views and expectations about using an online PHR?
Methods
This study used a qualitative descriptive design35 and consisted of focus groups conducted between September 2010 and April 2011 in a community setting in Montreal, Canada. We targeted ‘typical’ healthy English-speaking young adults, 18-34 years old; therefore, participants with major health conditions were excluded. No prior knowledge of PHRs was required. In congruence with the research design adopted, purposeful sampling with the aim to maximize variation in regard to variables such as age, sex and field of study was employed. This strategy allowed us to obtain a rich mix of female and male participants of varying ages and backgrounds; however, there was an element of convenience sampling, as participation was voluntary. Participants were recruited from university campus posters, ads in online classified systems, and personal networks. Ethical approval was obtained from the McGill Institutional Review Board before the commencement of the study.
The primary method for data collection was focus groups, which seek a broad range of ideas on an open-ended topic and are well suited to exploring users’ views of a service or product.36,37 Prior to discussion, informed consent forms and pre-interview questionnaires were distributed to participants (please see Table 1). Four focus groups were conducted, with a total of 29 participants, with group discussions lasting on average 90 minutes with four to ten participants per group. Subjects were assigned to focus groups with the aim to vary the mix of the group, but were also based on scheduling availability of participants. Questionnaires were anonymous and composed of 26 questions pertaining to sociodemographic information, computer/Internet use, health and prior PHR knowledge and attitudes (Appendix 1). Data from questionnaires were used to characterize and describe participants as a whole, in order to help situate the research and its findings. Focus groups were recorded and subsequently transcribed. A brief presentation was given to introduce the topic of PHRs to the group, followed by discussions facilitated by the primary author using a semi-structured interview guide (see Appendix 1). Table 1 outlines the characteristics of participants based on the pre-interview questionnaires.
Transcripts of interview data were analyzed using inductive thematic analysis, which is a method for identifying, analyzing and reporting patterns (themes) within data.38 An inductive approach allowed for themes to be identified directly from the data, which was appropriate given the exploratory nature of this study.38 Analysis focused on the semantic level, and followed the phases as proposed by Braun and Clarke:39 (1) transcription, reading and rereading of the transcripts for initial familiarization with the data and for preliminary ideas to be noted; (2) initial codes generated systematically, representing features of interest within the data; (3) codes subsequently collated into potential themes; (4) then checked against coded extracts and the entire data set, generating a thematic map of the analysis; (5) an ongoing analysis to name themes, refine specifics of each theme and determine what aspects of the data each theme was capturing; and finally, (6) themes examined in the light of existing knowledge. Data were coded and analyzed by a single coder (the primary author); however, codes and themes were reviewed and discussed with the other authors on an ongoing basis through the analysis and revised where needed. NVivo8 software was used to assist in coding and organizing the data, and SAS 9.2 statistical software was used to obtain basic descriptive statistics from questionnaire data.
Results
Six overarching themes emerged from thematic analysis: the first three themes pertained to how participants viewed PHRs, and the other three themes pertained to how participants expected to use PHRs themselves.
Young people’s Views about a PHR
Theme 1: Perceived advantages of a PHR
In terms of how participants viewed PHRs on a more conceptual level, they pinpointed several potential advantages: having a comprehensive consolidated record, having an accurate health record, being able to access their health record anywhere, having personal health information be integrated with their medical record, using the PHR to improve the efficiency of the health care system and using PHR information for research and to identify population-level trends.
‘Given our context, of the Quebec system and the shortage of doctors, so many people don’t have a family doctor, so they’re never seeing the same person. They’re always seeing somebody different. So being able to go to any doctor, any clinic, and they can pull up that information and see, I mean, that’s priceless’. (Participant #23, Group #4, female)
‘ºJust having the opportunity of carrying all of your information, and for different doctors to be able to access that information, no matter where in the world you are, that’s kind of the most important part, for me personally’. (Participant #24, Group #4, male)
‘I think that the health of everyone being hosted in the cloud really helps in identifying trends, within groups’. (Participant #24, Group #4, male)
Theme 2: Potential PHR users
Participants also discussed who might be most likely to use and benefit from a PHR. Computer literacy was seen as an important factor; as such, some believed that their generation would be more apt to adopt this type of technology than older adults, since they are more accustomed to using computers and the Internet in their day-to-day life. Though it was thought that people with more health issues might benefit more from PHR use, it was also acknowledged that healthier individuals might be more likely to use it. Education and health literacy was also seen as a potential factor in PHR access and use. Lastly, caregivers were a group seen as using or being able to benefit from using a PHR.
‘People our age, we all use the Internet, and when we get older, I think we’ll still be using the Internet. I think it would be a lot easier and more feasible for us to do that than to just expect older people now to start doing that. I don’t think older people now would really do that at all. But I think us, in the future, would’. (Participant #6, Group #1, female)
Theme 3: Concerns about PHRs
When it came to what concerned them about PHRs, issues of security and confidentiality were dominant. Participants conveyed a reticence of putting sensitive information in the PHR, for fear of a breach in privacy. Many were concerned that the information could be accessed and used by employers or insurance companies. Security and confidentiality concerns were magnified in cases where individuals might have a stigmatizing medical condition, and they worried it would change the way they would be treated. However, they conceded that these issues were not a current concern for them since they were still healthy: ‘If I had a serious chronic health issue, I would be nervous about putting that information out into the cloud’. (Participant #18, Group #3, male) Participants also considered how information could be collected and sold for advertising and marketing purposes, and acknowledged that it was the underlying business model in many of the sites they frequented. They accepted this as a possibility for PHRs, especially free PHRs, and felt conflicted about it. Concerns with security and confidentiality were mitigated by who was sponsoring the PHR: ‘Certainly I wouldn’t trust a private institution to do it. The government I have a little more faith in’. Data integrity was also a concern, as well as what would happen should the information be changed, lost or deleted. Despite apparent misgivings about security and privacy, these issues did not appear insurmountable. Several participants cited Internet or online banking as an example of how things could change: ‘I say [I’m worried but] I know full well that I bank on the Internet and I use it for a lot of other things. So I say, yeah, I’m worried about it, but would that stop me? Well, I don’t know, that’s another question’. (Participant #3, Group #1, male)
Young people’s Expectations in regard to the Use of PHR
Theme 4: Desirable PHR characteristics
When it came to how they personally envisioned themselves using PHRs, participants had strong expectations about the characteristics they felt it should have. For one, they repeatedly expressed the importance of making the PHR easy to use. They referenced websites or systems that have persisted as benchmarks, such as Google and Facebook, and stressed the value of having a simple, user-friendly interface. For them, a PHR that was difficult to navigate or use would represent a major barrier to adoption; conversely, a welldesigned interface could actually motivate them to use it.
‘If it’s slightly challenging, or people don’t feel that it’s simple to use, or what the information they’re putting in easily describes what they have, than that will certainly deter people.’ (Participant #3, Group #1, male)
‘It sounds silly, but I’m sure that it’s really important. Just make it attractive.’(Participant #5, Group #1, male)
Since participants believed that using a PHR required an initial, if not regular, investment of their time and effort, they wanted the interface for entering data to be simple to use and streamlined.
‘One thing for me that would be really important would be the ease of entering data. Because if it’s like, if I have to go through a lot of checkboxes, and dropdown menus, and stuff like that… like auto-completion – I think on Google they had something like that? That would be really useful for here. …really make it easy, and really user-friendly.’ (Participant #17, Group #2, male)
Since many believed that the value of the PHR lies in its ability to connect with other information systems, common data standards were identified as an extension of usability. Participants wanted to be able to easily transfer their medical record into their PHR and did not relish the possibility of having to reinput their health information into new systems, should the need arise. Participants also felt that the PHR should be customizable to suit the personal preferences and needs of the specific user. As one participant justified, they wanted to be able to tailor the PHR interface in order to display only what information or tools were relevant to them and wanted to have control over certain features of the PHR, such as frequency of reminders. The need to customize or control elements of the PHR extended to the information itself. Participants wanted to be able to decide what information they shared and with whom. Most viewed control and customization as a way to address and ensure that there was a fit between the PHR and different user needs and preferences.
‘It should definitely be designed from the perspective of the patient, and the patient’s mental model… it would have to be designed for what they’re looking for.’ (Participant #14, Group #2, male)
‘I’d be surprised if someone could design one tool that could solve everyone’s needs. I think it would have to be customizable. ’(Participant #18, Group #3, male)
Also, the majority of participants did not feel that they should have to pay for a PHR. Participants wanted their PHR to have interactive elements or give them feedback. They wanted to see visual representations of the data, whether it be graphs and charts, and believed that it could help them gain a better understanding of their health. They also wanted their PHR to provide feedback in the form of reminders or even encouragement. Participants went so far as to desire a sense of reward for using the system. However, they were only interested in using the system so long as the feedback was positive; if the PHR reminded them that were not in good health, or were not making good lifestyle choices, they would be less motivated to use it, as it would discourage them. Many participants proposed that notion that introducing games or applying game psychology to preventative health within the PHR could be an effective way to motivate them to use it while avoiding possible discouragement.
‘If I can monitor my food, my exercise, and it can all be presented in a game, like a video game format, I could definitely get into it… [because] the idea of game psychology, is that it’s set up so that you’re not discouraged at any point. It’s addictive. You’re only rewarded. And you’re rewarded at specific intervals to keep you interested, you know. But it’s never hard enough that you’re just going to want to turn it off?’ (Participant #8, Group #2, male)
Theme 5: Using the PHR for preventative health
Since participants considered themselves healthy, they primarily saw themselves using the PHR, at least at this point in their lives, for preventative health. One key theme and expectation was the idea that the act of tracking could create awareness and help identify patterns in their life, and in turn help them make healthier lifestyle decisions. Tracking health with the PHR was a way to help them recognize patterns in their life, and see the associations between things like diet, exercise and the effect they might have on their health.
‘I think someone who starts this process can be more conscious about his own health. If you start entering how much you slept, how much you weigh, it may be that you’re going to find out things you have things you’re going to have to change in your life.’ (Participant #4, Group #1, male)
Participants expressed a desire to use the PHR to compare or rank themselves against the ‘average’ or a norm. By having a standard to compare themselves against, they could also set targets.
‘You compare yourself with a standard… here’s the average for 20-whatever year old. It would be cool if you also could maybe set some targets… I think it would help motivate me a little bit if I said – oh, there’s my target.’ (Participant #18, Group #3, male)
Some participants expressed the desire to use a PHR to gain a better understanding of their own family history. Becoming aware and informed of genetic susceptibilities was expected to help guide better choices to prevent future illness, for themselves and future generations. Despite the potential benefits offered by the PHR, some viewed tracking and using the PHR as a waste of their time, and did not consider it to be worth the payoff unless they were actually sick.
‘I don’t feel any need yet. I don’t see a doctor regularly or anything, so I would just be spending useless hours filling in things at this level. I probably wouldn’t use it, until I have some kind of condition.’ (Participant #5, Group #1, male)
Many participants expressed concern that maintaining their data in a PHR would be too time consuming as they felt there were already too many demands on their time. However, some felt that they would be more willing to invest the time if it interacted with their physician and offered the possibility of getting an answer.
‘Maybe if you have more advanced [PHRs], where you can get feedback from a physician or something, then you would have an incentive to track, because then you know that you’ll get a possible answer.’ (Participant #1, Group #1, female)
Furthermore, since time was considered a valuable commodity, the majority agreed they would likely use features of the PHR that would save them time.
Theme 6: Taking more control of their health
Another theme was how PHRs could help them take more control of their health. Some participants expected that using a PHR would enable them to take more responsibility and control of their own health and health information.
‘A lot of people that go to doctors or utilize medical services totally rely on the physician and their opinion and their information. But having that knowledge and awareness, you won’t have to rely on them so much.’ (Participant #28, Group #4, male)
In contrast to how they viewed PHRs in a more general sense, when it came to how they expected to personally use the PHR, participants mainly focused on the idea of avoiding care, rather than improving care. The majority wanted to be able to avoid going to see the doctor, unless deemed absolutely necessary – largely due to the time and effort they felt it required to do so. Many expressed frustration in their experiences trying to access care, whether it was the difficulty making appointments with a doctor or waiting hours to see a doctor. As a result, many felt it was best to circumvent seeing the doctor altogether, and looked to the PHR as a way to facilitate that largely through self-diagnosis. Many already used the Internet to self-diagnose their symptoms or conditions.
‘I would do that before I would bother going and waiting in a clinic for four or five hours, which I think is ridiculous. I would always check things online first, before I go to a doctor.’ (Participant #21, Group #4, female)
They did acknowledge that there were risks with assessing or taking action without proper medical judgment. Despite these risks, most participants wanted to find alternatives to having to go in to see a doctor, so it was also thought the PHR could potentially provide more relevant or authoritative health information resources for patients.
‘Providers could probably put information there that’s more reliable than whatever you find on the Internet. It’s hard if you want to educate yourself, but you don’t know which websites are better, so that could be a way to help patients go, for some that don’t know it – more efficient.’ (Participant #9, Group #2, female)
Discussion
Results revealed that when discussing their views on PHRs, young adults identified benefits previously voiced by older patients and other stakeholders. Participants emphasized accessibility of personal information as a priority - unsurprising given that within this age group, relocation is common and they are accustomed to easy and immediate access to information through smartphones. They also stressed the value of an integrated system–to them, the act of putting information online necessarily implied and required greater connectivity to people and information systems. They believed that it was their generation that would be more likely to adopt this type of technology, and suggested that healthier and more educated individuals might be more likely to use it, echoing the findings from Weingart et al.40 Though their generation is apt to share many personal details of their lives on the Internet, the self-described ‘Facebook generation’, participants expressed concerns about privacy and security similar to what has been previously reported in other, older populations.23,41–47 However, they demonstrated an awareness and concern about how their information could be sold and exploited for commercial use. Despite their concerns about how information could be collected, compromised, they suggested that it could be mitigated by convenience (using the example of online banking), though it was not conclusive.
What was striking was how the focus and motivations changed when participants considered how they would personally interact with the PHR. Their prior experiences with technology, the health care system and their perception of their health played a big role in determining their individual expectations about using a PHR. Participants stressed the importance of usability, or ease-of-use, which has long been considered a crucial element for adoption of information technology. 48–50 Moreover, since PHRs are user-driven, having a system that is easy to use becomes even more essential for uptake. However, what contributes to ease-of-use may vary between populations. While in a report on PHR usability, Marchioni49 believes that customization is important for older users and people with specific chronic health conditions, our findings suggest that customization is equally if not more important for younger and healthier users. Since they are not using it to actively manage a condition but looking to use it for preventative health, they want the PHR to require a minimum of effort and be tailored to their needs. Their expectations of a new or prospective technology like the PHR were grounded in their experiences with existing technologies, especially ones that they used on a day-to-day basis. For example, the need to have control over exactly what elements they shared and who they shared it with was compared repeatedly to Facebook’s privacy settings. Google was used as an example of clean interface design, but also as an example of how information can be mined or used for more directed advertising. Young adults expected to be able to do, at a minimum, the same things if not more with a PHR as they do with existing tools.
As young healthy adults, participants primarily considered the PHR in the context of preventative health. They expected to use the PHR to play a role in maintaining good health, and exhibited an awareness and recognition of the role of lifestyle choices, such as diet and physical activity, in preventing illness. They saw the PHR as a way to help keep track and become aware of these choices and how they impacted their health. They expected that the PHR could help them learn or understand what they should be doing, by providing reputable and up-to-date health information resources, guidelines, targets and facilitating the ability to compare themselves to their peers or the average. Participants also expected and stressed the ability of the PHR to help them become aware of what they were actually doing, to become more conscious of choices that they might be making in their everyday life that needed to be changed. Lastly, they spoke considerably of the PHR providing reinforcement or reward in such a way that it would not only encourage them to continue tracking, but also encourage them to keep making positive lifestyle choices. This sense of ongoing achievement and motivation was considered crucial in having the PHR be used to encourage preventative health behaviours. In the particular subpopulation of young adults, our study corroborates what the scarce evidence on this topic seems to point out, namely that PHRs may support and promote preventative care.51,52
The literature has promoted the idea that one of the major benefits of PHRs is its potential to increase the involvement of patients in their own care.4,7–10 Our results support the idea that young adult users similarly expect the PHR to increase self-management in their own care. However, young adults not only envisioned the PHR as a way to have more ownership in their health but also as a means to become increasingly independent of the health care system. The majority of participants expressed considerable frustration with the health care system and issues with access to care or quality of care. Though they simultaneously recognized that it was due to the limited resources of the health care system, participants were discouraged by long waits and difficulties seeing a doctor. In fact, only one-third had a regular physician in Montreal, and one-third did not have a regular doctor whatsoever. Issues with access to care motivated them to look to the PHR to address these issues by either improving the efficiency of existing services or largely as a way to avoid care altogether. Many young adults already used Internet to seek out health information, or to ‘Google’ symptoms, and as a way to self-diagnose as opposed to seeking out the opinion of a medical professional. In fact, some considered it a preferable first step, before investing hours in a waiting room. Even though they recognized potential dangers and pitfalls of Internet self-diagnosis, they preferred it as an alternative to scheduling a medical visit, and therefore wanted the PHR to serve as a source of more authoritative health information.
Another concern was the challenge and suggestions as to how to make the PHR worthwhile to users. While the perceived burden on time and effort has been discussed as a barrier to HIT adoption in the professional and organizational context,53,54 these results suggest that it is equally important in systems geared towards the patient or consumer as the end-user. Having grown up in the information age, young adults are faced with the increasingly fast-paced demands of modern life. Many participants spoke of already feeling pressured or burdened by existing commitments, and had no interest in adding another obligation. They only saw it as being useful if it in turn provided some discernable advantage, either through convenient timesaving features or through instantaneous feedback. The importance of interactivity and reward has not yet been explored in existing PHR literature, though has since been seen increasingly in consumer health and wellness technologies, such as fitness trackers and weight loss apps. Young adults are used to interacting with technology and using it beyond a functional pragmatic level. Technology is part of their leisure and games were repeatedly stressed as a benchmark for how PHRs for prevention could be made more appealing. It suggested that a sufficiently motivating system might be able to provide the impetus to encourage better health decisions.Though the need for interactivity and reinforcement is particularly important when PHRs are used for prevention in healthy individuals, this finding suggests exploring ways to make the PHR more satisfying or ‘rewarding’ in order to encourage lasting, long-term adoption.
Based on these results, we are proposing a conceptual framework that may help explain the influence of three major driving forces on the expectations of use of PHR in young adults (see Figure 1): experience with existing technology, experience with the health care system, and perception of health and health risks. Participants referenced systems they already knew as indications as to what they could and did expect from PHRs. Secondly, the individual’s experience with the health care system shaped their expectations about using a PHR as well. Frustrations and difficulties with access and getting care led them to see the PHR largely as an alternative to care. Lastly, the individual’s perception of their health and health risks influenced their personal needs for managing their own health. In the case of young adults, this led to the primary expectation that PHRs would be used for preventative health, rather than disease management.
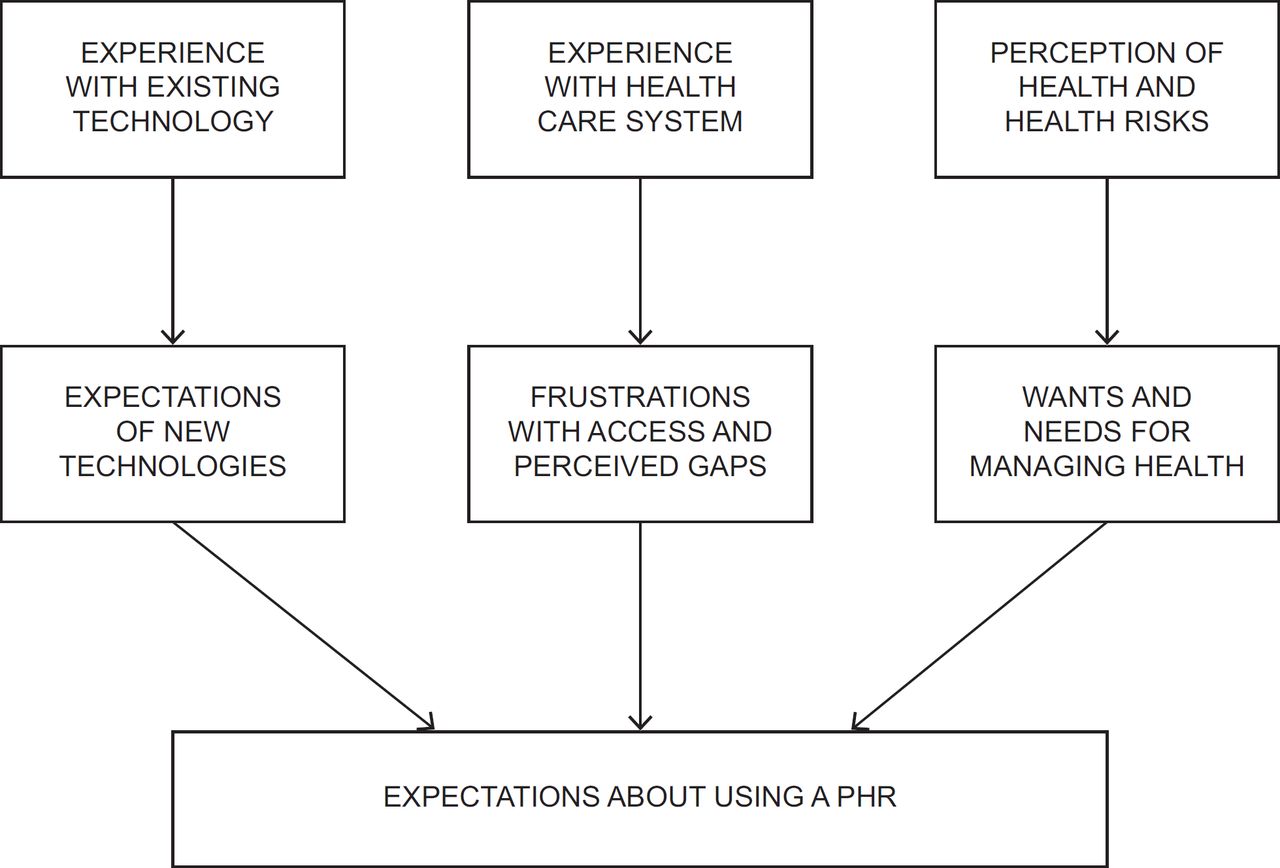
{kind=link}
This framework, derived from our inductive analysis of the empirical data on young adults and PHRs specifically, is coherent with other broader models of technology acceptance, such as the TAM. The expectations of using a PHR encompass both perceived usefulness and perceived ease-of-use. Perceived usefulness of a PHR is influenced by young adults’ experience with the health care system and the perception of their health, while their experience with existing technology helps constitute what they consider to be ease-of-use. Moreover, in a preventative context, ease-of-use is even more crucial to ensure uptake. In fact, Venkatesh and Bala55 suggested a theoretical framework synthesizing prior research on TAM, with four different types of determinants on perceived usefulness and perceived ease of use: 1) individual differences, including personality and/or demographics; 2) system characteristics, or ‘features of a system that can help individuals develop favourable (or unfavourable) perceptions regarding the usefulness or ease-of-use of a system’; 3) social influence, or social processes that guide individuals to formulate perceptions of an IT; and 4) facilitating conditions, or organizational support that facilitates the use of an IT.55 In this view, our framework focuses on individual differences, namely the users’ experience with technology, experience with the health care system and motivations with regard to taking control of their health. These individual characteristics warrant further exploration and research when targeting PHRs towards specific populations. Given the spectrum of differences in individuals and health care contexts, this supports the idea that PHRs will absolutely need to be customizable, in order to meet what could be a broad range of subtle, yet important differences between potential users – an idea that was stressed by participants themselves. However, this framework only considers user expectations, so an exploration of what will deter users from adopting PHRs warrants further study.
This study suggests that there is potential for PHRs to be a tool in preventative health, but that to do this, we should look at PHRs more generally as ‘user-centered’, rather than ‘patient-centered’. More research is needed to understand what can influence user expectations or perceived usefulness, and how to arguably not only make PHRs easy to use, but inherently satisfying, in order to ensure lasting uptake. As our framework also suggests that experience with existing technology is important in determining perceived ease-of-use, future research could analyze characteristics of technologies widely adopted in specific user populations, such as young adults, to provide a better grounding in designing what should be incorporated into PHRs. In using PHRs not only for managing disease, but also for managing wellness and health, there is a better possibility for this technology to become broadly adopted.
Limitations
Limitations include the fact that eligibility was restricted to English-speaking participants. Participants were also tended to have a high level of education and their awareness of technological and theoretical issues may not be representative of their age group as a whole, and the majority (79.3%) were between 25–34 years old. Also, though sampling aimed to maximize variability, participation in the focus groups was voluntary, so there may have been an element of self-selection.
Conclusion
In this research, we explored the views and expectations of young healthy adults about using a PHR, and revealed that what they perceived as benefits when considering the system as a whole did not necessarily equate to what would motivate them personally to use it. These differences may be precisely because this population is young and mostly healthy. Their primary motivation is not to manage or track an existing health condition or illness. Since the consequences of not tracking or using a PHR is less severe, and with time as a valued commodity, it suggests that a more significant barrier to adoption in this group is the time and effort required to maintain information in the PHR. Therefore, a greater sense of inherent reward and motivation has to be provided by the PHR to encourage initial uptake and ensure long-term usage. Based on these results, a conceptual framework was proposed that outlined factors influencing expectations in this population. These findings provide new insight into how issues may vary in different populations, and point to possible causes of low adoption rates. Adoption may hinge more on the fit between the PHR and the individual’s personal expectations and anticipated use, rather than on the perceived benefits of such a system. Much of current enthusiasm about PHRs has focused on its anticipated benefits. This study suggests that more research is needed on how users anticipate using the PHR, and how to make the PHR easy to use for those populations. Moreover, while this study made some initial theorizations about the expectations of PHR use in young adults, more critical exploration is needed to understand what would deter them from using it, aside from usability and relevance issues. Regardless of potential benefits expounded by policymakers and stakeholders, adoption may rely on having a better fit between the technology and user expectations and anticipated use of that system, especially with a user-driven system such as the PHR.
Authors Contributions
The manuscript has been read and approved by all the authors. The requirements for authorship have been met and that each author believes that the manuscript represents honest work. The list of the authors and their specific roles in the preparation of the manuscript are: (1) Quynh Nguyen who is the first author who drafted the study protocol, obtained ethics approval and conducted the focus groups. In collaboration with the other authors, she contributed the majority of the writing of the manuscript. (2) Gillian Bartlett is the corresponding author and supervised the development of the protocol, the conceptualization of the manuscript, some writing and detailed supervision in the preparation of the manuscript. (3) Charo Rodriguez and Pierre-Paul Tellier approved the final version of the study protocol, assisted in the conceptualization of the paper, supervised the analysis of the data and participated in multiple revisions of the manuscript.
Acknowledgments
The support for this project was provided through the grant ‘Empowering Patients: Making the PHR accessible and relevant for primary care’ awarded to G. Bartlett by the Canadian Institutes of Health Research through Primary Care Catalyst competition (2010).
The authors have no conflicts of interest to declare.