Article Text

Abstract
Background The use of medication is at the heart of primary care, but is also the cause for major health concerns. It is therefore important to examine the prescription of medication process.
Objective This study identifies the barriers and facilitators perceived by community pharmacists and primary care physicians concerning the adoption of a nationwide electronic prescribing (e-prescribing) network in the province of Quebec, Canada.
Methods We used purposive sampling to identify the most intensive users of the e-prescribing network. We conducted phone and in-person interviews. Interviews were transcribed, and we analysed their content with NVivo, using the clinical adoption framework (CAF) for the codification of the data.
Results We interviewed 33 pharmacists, 2 pharmacy technicians, 11 physicians and 3 clinic managers. Adoption of the e-prescribing network was fairly low. The respondents underlined adaptation of their work environment, openness to change and perception of benefits as facilitators to the adoption of the network. However, important barriers were perceived, including system quality issues and paper prescriptions being the only legal document in the prescribing process. Even if respondents recognised that the e-prescribing network can offer substantial benefits to the prescribing process, issues still persisted and raised barriers to the full use of such a network, especially in a context where different local information systems are connected within a nationwide e-prescribing network.
Conclusion This study, based on the CAF, provides a better understanding of the factors related to the adoption of a nationwide e-prescribing network connecting primary care clinics and community pharmacies.
Where this study fits in?Electronic prescribing could improve the processes related to the use and dispensation of drugs in health care, but their adoption is still poor in the North American context. Research on the topic of adoption of electronic prescribing is still limited, particularly among health professionals other than physicians. This study, based on the clinical adoption framework (CAF), provides a better understanding of the factors related to the adoption of a nationwide electronic prescribing network connecting primary care clinics and community pharmacies in the province of Quebec, Canada.
- adoption factor
- clinical adoption framework
- electronic prescribing
- pharmacists
- physicians
- primary care
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
The use of medication is at the heart of primary care, but is also the cause of major concerns, notably in terms of patient safety. Indeed, medication usage is a complex process, involving multiple actors, and it is prone to errors.1 Drug-related illnesses are amongst the most common medical adverse events and are one of the leading causes of mortality.2,3 According to the O’Hagan et al.4 study on self-reported medical errors in USA, Australia, Canada, Germany, the Netherlands, New Zealand and UK, at least one respondent on ten for each country believed that he or she experienced medical or medication errors in the past two years. Yet these are often the kinds of errors that are preventable.3,5–7 Therefore, it is important to improve the processes related to the medication use in primary care, notably prescribing and processing.8,9 The computerisation of these processes, with the help of information and communication technologies, is a path that numerous countries have followed.10
The use of advanced features of electronic prescribing (e-prescribing) enables the exchange of medication data between a prescriber and a pharmacist, as opposed to first-generation e-prescribing that only allows an electronic application for entry, modification and review of prescription.11 Secondgeneration e-prescribing enables safe electronic sharing of a patient’s prescription between an authorised prescriber and a retail pharmacy through the use of an e-prescribing application or a pharmacy management software12,13 and dispensed medication data can be shared by the pharmacy management software through claims14 or a medication database.15 Thus, e-prescribing has the potential to improve the quality, safety and efficiency of care; it could also be cost effective for the health system and reduces medication errors6,14,16–19 by acting on poor handwriting and on the lack of communication between professionals.20 Even so, the implementation and adoption of e-prescribing is still poor, particularly in the North American context.16,17,21,22 Previous studies have documented the implementation and adoption of e-prescribing in primary care,23 but research on the topic is still limited, particularly among health professionals other than physicians23,24 and on the second generation of e-prescribing.11
In Canada, Health Canada announced in 2007 that there was no impediment to e-prescribing and that electronically generated and transmitted prescriptions are permissible as long as they achieve the same objectives as written prescriptions.20,25 Despite this, electronic prescribing is still not widely adopted in the country. Indeed, only 43% of Canadian family physicians routinely use electronic prescribing, 26 and of those, many solely enter their prescription electronically in their electronic medical record (EMR) in order to print or fax the prescription. Nonetheless, the use of electronic prescribing is increasing in Canada.26 This study examines the province of Quebec’s nationwide e-prescribing network, the first initiative of the kind in the country.
Quebec e-prescribing network
Quebec’s e-prescribing network is a second-generation e-prescribing system that consists of a central repository separated in two data warehouses: 1) the e-prescription warehouse and 2) the medication history warehouse. Prescribers can send their prescription data to the e-prescription warehouse from the prescription module of their EMR. The pharmacist or pharmacy technician from the pharmacy chosen by the patient can then ‘pull’ the data from the e-prescription warehouse into its pharmacy management software using the patient’s health insurance number, a unique nationwide identifier. Moreover, all the dispensed medications are added to the medication history warehouse automatically when entered in the pharmacy medication management software. This warehouse is accessible by both the prescriber and the pharmacist for viewing through their respective local information systems or by using an Internet browser. Finally, physicians can import the data from the medication history for prescription renewals or other clinical purposes. At the time of the study, every person with principal residency in the first four regions where the e-prescribing network has been deployed and who are covered by the provincial universal health insurance plan are registered in the e-prescribing network, unless they have chosen to opt out.27
The aim of this study was to identify the barriers and facilitators perceived by community pharmacists and primary care physicians with respect to the implementation and adoption of a nationwide e-prescribing network in the province of Quebec, Canada.
Materials and methods
Setting and participants
The sample was selected through purposive sampling in order to identify the most intensive users of the e-prescribing network. At the beginning of 2013, we targeted primary care clinics and community pharmacies that had the highest levels of usage of e-prescriptions through the e-prescribing network, according to the data obtained from the provincial universal health insurance board. Users were contacted by phone at their workplace. Letters of support were given by the Quebec Association of General Physicians and the Quebec Association of Pharmacists–Owners to help us contact clinic managers and pharmacists, respectively. In total, 24 medical clinics and 41 pharmacies were contacted. The study received approval from the CHU de Québec Research Centre’s ethical committee prior to the recruitment of respondents.
Data collection and analysis
We conducted semi-structured interviews in person or by phone between February and September 2013, depending on the participant’s preference. The interview guide consisted of three main themes: respondents’ experience regarding use of the e-prescribing network, issues related to the network and benefits to the use of the network. Informed consent was obtained from all the respondents, and financial compensation was offered to them for their time.
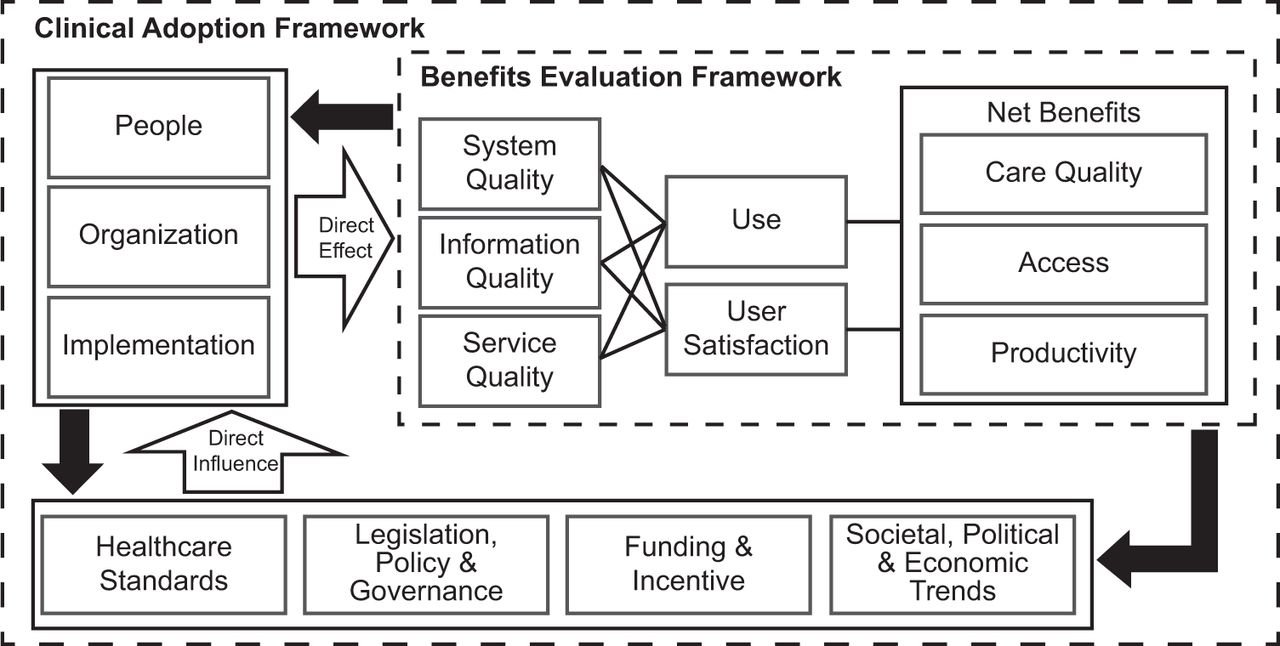
Interview content was transcribed and analysed with the support of the qualitative data analysis computer software NVivo.28 We used the CAF proposed by Lau et al.29 for the codification of interview content (see Figure 1). The CAF makes it possible to classify adoption factors of health information systems by clinicians.29 This model categorises adoption factors according to three levels: micro (net benefits; use; user satisfaction; system, information and service quality); meso (people; organisation; implementation) and macro (standards; legislation; policy and governance; funding and incentives; societal, political and economic trends).29,30 We analysed phone and in-person interviews since there was no noticeable differences between the two sets of interviews.

{kind=link}
Results
In total, we interviewed 49 persons (19 face to face and 30 by phone). Table 1 presents the socio-demographic characteristics of the respondents. Community pharmacists accounted for a majority of respondents (67%). The respondents were part of two different waves of implementation of the e-prescribing network. The first wave, represented by 20 respondents, began in 2008 and was completed in 2010. While many pharmacies were connected at the beginning of the implementation of the e-prescribing network, it took a longer time for medical clinics to come onboard and for patients to be registered in the network, leaving a gap in the medication data available in the network. The second wave, represented by 29 respondents, began at the end of 2011 and was more uniform, having both clinics and pharmacies concurrently connected, as well as having a more complete compilation of patients’ profiles upon implementation. Since the respondents came from the first establishments that adopted the e-prescribing network in the province, we can consider them as early adopters to the network.
Even if we recruited professionals from pharmacies and clinics that had the highest levels of usage of e-prescriptions, respondents reported a very low use of the e-prescribing network.31 The underutilisation of the network was caused by many barriers to adoption common to pharmacists and physicians, and these barriers are mostly related to system quality.
Issues with system quality
A recurrent and critical problem mentioned by professionals was the lack of data standardisation that led to inadequate data importation and exportation, especially concerning medication instructions. Not only did these instructions need to be modified manually, but pharmacists also had to modify medication names so that they would correspond with their inventory and patient insurance claims. Subsequently, this was also a problem for physicians. Indeed, this modified list was automatically sent to the nationwide medication history warehouse, and then retrieved by the physician who was confronted with medication names that did not match his or her initial prescription.
Respondents also reported a lack of interoperability between their local information systems as an irritant as regard the use of e-prescribing. Physicians and pharmacists had to use a second application or screen to have access to the e-prescribing network since it was not integrated in their information system. Physicians that used the network during the early stages also noted that the time lag before automatic log out from the network was too short. However, this problem was resolved before the end of our study, as pointed out by the last respondents. Physicians added that there were important delays in network transmission. Indeed, each medication on the prescription was sent one at a time to the e-prescribing network. A single transmission could take a few seconds. While a few seconds accounted for little individually, they added up at the end of a day. These interoperability problems led to an important loss of time and accentuated risks of error, which were seen as powerful barriers to the use of the e-prescribing network by respondents.
The waves of implementation of the e-prescribing network also affected system quality, to the detriment of the first wave. During the first wave of implementation, a large number of pharmacies were connected to the network, thus sending their dispensing data, but very few physicians were connected to it. This situation led to a shortage of prescriptions in the e-prescription warehouse, which often led to the underutilisation of the e-prescription warehouse by pharmacists. On the other side, it seemed that the more recent implementation and a shorter time lag in the cadence of connections of pharmacies and clinics during the second wave led to a greater perceived usefulness among professionals, which has facilitated their adoption. However, respondents from both waves underlined the importance of rapidly expand the e-prescribing network to other regions and to hospitals, so more information might become available in the network.
Nonetheless, some functions of the e-prescribing network worked well and benefited physician and pharmacists’ work. In general, respondents believed that consultation of the medication history warehouse was easy to carry out and functional. E-prescribing also made prescriptions more legible. The automatic transmission of data from pharmacies to the nationwide medication history warehouse and the streamlining of the renewal process in clinics were the functionalities most appreciated by respondents. In addition, most respondents noted that data from the nationwide medication history warehouse were useful to complete patient files and could warn the user in case of patients with potential drug abuse problems.
Effects of system quality on other factors
System quality issues had effects on other factors reported by the participants. Individually, most physicians did use the e-prescribing module included in their EMR, but few transmitted their prescription through the network or consulted the data from the medication history warehouse. Since the use of the network was an individual and voluntary act for physicians, many preferred to remain disconnected to avoid the issues related to the system. Consequently, information contained in the nationwide e-prescription warehouse was often incomplete, outdated or not available for pharmacists. By adding implementation issues to this situation, the lack of available or complete information due to few prescriptions sent through the network was a strong factor in demotivating pharmacists. However, they asserted that patient information was becoming increasingly available in the medication history warehouse, suggesting an improvement in the situation.
Reluctance from pharmacists caused by the system quality issues was less apparent. The earlier computerisation of community pharmacies’ local work environment and regular use of electronic local pharmacy software facilitated the adoption of the e-prescribing network. Moreover, the automatic exportation of data to the nationwide medication history warehouse was imposed as soon as a pharmacy was connected to the network.
Finally, we observed that openness to change was important in the adoption of e-prescribing since people who were ready to invest time and effort in the appropriation of the network were the ones who believed that it was a solution for the future. However, even if the early adopters were convinced of the potential benefits of the e-prescribing network, it seemed difficult to maintain their motivation over time because of the lack of perceived added value following the use of the network, particularly because of the numerous barriers related to system quality.
Other factors influencing e-prescribing adoption
Some other factors hindered the adoption of the e-prescribing network in clinics and pharmacies. First, pharmacists and physicians noted a lack of training in the use of the e-prescribing network. In particular, respondents mentioned training periods that were too short, lack of training following implementation and the absence of training for pharmacy technicians. This has resulted in incomprehension when using the network, a gap in the use of advanced functionalities of the transmission of prescriptions and ultimately, the underutilisation of the network. However, the training was judged sufficient by a minority of pharmacists, who even specified that it was possible for them to receive updates if needed.
Additionally, the technical support received by the pharmacies from their software provider was problematic. First, respondents perceived that technical support and followup were minimal and far from satisfactory. Most of them believed that the IT technicians lacked the expertise to fully understand the specifics related to the e-prescribing network. Moreover, delays in customer service could be very long, preventing the user from performing his or her usual tasks in the meantime.
Having a paper order as the only legal document in the e-prescribing process also appeared as a significant barrier to the use of the network since it required patients to bring their paper prescription with them to the pharmacy even if an electronic version of the prescription was available through the network. It also legitimised a hand process of prescription that remained based on the information found on the paper prescription, and then transferred manually to the local pharmacy system.
Conversely, other important factors facilitated the adoption of the network in the primary care clinics. Indeed, some clinics have successfully opted for the involvement of all their clinicians in the system implementation and for the presence of an on-site champion who could support physicians in their use of the system in order to favour a large as possible use. These two strategies seemed to greatly facilitate the implementation of the network in the clinics. Also, the provincial government offered a financial incentives program to support the computerisation of primary care clinics. It was seen as a facilitator to the adoption of the e-prescribing network by physicians since the transmission of medication information to the network was among the six functionalities that had to be used by physicians in order for them to benefit from the incentive program. Table 2 summarises the factors identified, classified by themes from the CAF, and presents selected quotes from the interviews.
Discussion
Principal findings
This study highlighted key issues concerning the barriers and facilitators perceived by community pharmacists and primary care physicians with respect to the implementation and adoption of a nationwide e-prescribing network.
Adoption of the e-prescribing network was far below the initial expectations. Even if all the participants came from clinics and pharmacies that were the highest users of the network, its use was still very low among them. For physicians, such use seems to follow the tendency of health-related technologies use in the province. Indeed, physicians from the province of Quebec are the lowest users of electronic tools for patient care in Canada.32 Respondents recognised that the e-prescribing network can offer substantial benefits to the prescribing process but issues still persist and raise barriers to the full use of such a network, especially in a context where different local information systems are connected within a nationwide e-prescribing network.
Comparisons with the literature
Many factors highlighted in our study are also present in the literature on e-prescribing adoption. Our results echo those from other studies and underline the importance of champions on the field,8 support and training,5,21,33 positive attitude toward the technology,22,33,34 improved workflow,2,35,36 information access,17,21 organisational support37 and financial incentives38 to facilitate the implementation of e-prescribing. The respondents also identified early computerisation of the work environment and automatic transmission of data as facilitators to its implementation.
A number of reasons can explain the underutilisation of the e-prescribing network. In this study, factors that were perceived as more crucial in the adoption of the network were related to system quality and were also identified in the literature: issues with interoperability between the systems,6,39,40 access to useful additional information that are not yet available in the nationwide system, such as laboratory results17,21,35,38,39,41 and lack of data standardisation. 11,17,24,34 This last issue compromises the security of the patient and may be dangerous if not properly addressed. There were also other crucial issues that were raised by the respondents but not underlined in the literature, notably the lack of legal autonomy for the e-prescription without the paper order signed by a physician and the uneven implementation of the e-prescribing network. These issues led the professionals to perceive more disadvantages than advantages in the use of the network and this ultimately led to its abandoning.
Limitations of the study
This study has some limitations. First, despite numerous efforts, it was more difficult to recruit physicians than pharmacists, even if all the connected clinics were contacted to solicit their participation. We think that data saturation was achieved42 among pharmacists, but data saturation was less evident with physicians. Nonetheless, the physicians’ comments were very consistent from one physician to another and were also in line with observations coming from pharmacists. It would be useful to complement the results of this study with more information regarding the experience of primary care physicians with the e-prescribing network.
Second, we conducted this study with the two first waves of implementation of a nationwide e-prescribing network. Perhaps, the implementation process may improve with experience, and future users will develop more realistic expectancies. Even if the first two waves showed some variations in their implementation processes, the study offers results that are in line with the evidence-based literature in the domain. So, we believe that this study provides valid findings that are representative of the experience of the network adoption all the more so that it concerned early adopters. These adopters are important because they act as opinion leaders, and their attitude toward new technologies is critical to successful implementation.
Third, our recruitment targeted clinics and pharmacies with the most frequent users and early adopters of the e-prescribing network. It would also be important to study non-users and infrequent users in order to develop a broader overview of the barriers to adoption and use of the network. However, we believe that focusing on these early users provides a significant and pertinent understanding of the issues related to the early stage of a nationwide e-prescribing network implementation and adoption.
Call for future research
There is still little research on e-prescribing systems in primary care and even less on the interoperability between a nationwide e-prescribing network and other local information systems that are present in health care facilities. Future research should look into these interoperability issues when e-prescribing and information systems are interconnected with a provincial or national level e-prescribing network.
Conclusion
The CAF used in this study was helpful in explaining the factors influencing the adoption of a nationwide e-prescribing network among physicians and pharmacists in a context where different local information systems are connected. Currently, the e-prescribing network can offer substantial benefits to health care professionals. However, significant barriers hinder the implementation and use of this network. It would be important to stimulate the interest of potential network users by working on the issues identified in this study, especially when these issues are highlighted by early adopters of the system.
References
Footnotes
Contributorship Claude Sicotte and Marie-Pierre Gagnon contributed to the study concept and design. All the authors participated in data collection and analysis, drafting of the manuscript and revision of the manuscript.
Conflict of interest The authors declare that they have no competing interest.
Funding This study is supported by a grant from Canada Health Infoway. The funding source had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the report or in the decision to submit the paper for publication.