Article Text

Abstract
Background The symptom of fatigue is one of the top five most frequently presented health complaints in primary care, yet it remains underexplored in the Canadian primary care context.
Objective The objective of this study was to examine the prevalence and impact of patients presenting with fatigue in primary care, using the only known electronic database in Canada to capture patient-reported symptoms.
Methods Data were extracted from the Deliver Primary Healthcare Information (DELPHI) database, an electronic medical record database located in Ontario, Canada. Patients were identified using the International Classification of Primary Care, Revised Second Edition coding system. Two groups of patients (fatigue or non-fatigue symptom) were followed for one year and compared. Both descriptive and multivariable analyses were conducted.
Results A total of 103 fatigue symptom patients, and 103 non-fatigue symptom patients, were identified in the DELPHI database. The period prevalence of fatigue presentation was 8.2%, with the majority of patients being female and over 60 years of age. These patients experienced numerous co-occurring morbidities, in addition to the fatigue itself. During the one year follow-up period, fatigue symptom patients had significantly higher rates of subsequent visits (IRR = 1.19, p = 0.038) and investigations (IRR = 1.68, p < 0.001), and markedly high levels of referrals following their index visit.
Conclusions This research used an electronic database to examine the symptom, fatigue. Using these data, fatigue symptom patients were found to have higher rates of health care utilisation, compared to non-fatigue symptom patients.
Where This Study Fits In
The symptom of fatigue is a common complaint in primary care practices, reported in approximately 5%–7% of primary care encounters.
Using the International Classification of Primary Care, Revised Second Edition (ICPC-2-R) coding system, fatigue symptom presentation was found among 8.2% of patients presenting to 10 primary care practices in Ontario, Canada.
With an average age of 63.1 years, the majority of these fatigue symptom patients were female (68.0%) and had co-occurring chronic and psychosocial conditions (88% and 52%, respectively).
Compared to a non-fatigue symptom patient group, patients presenting with fatigue experienced significantly higher levels of subsequent visits and investigations during the one year period following an index visit.
Future research using electronic medical records should continue to examine amorphous and complex symptoms, such as fatigue, to inform more effective and appropriate clinical management in the primary care context.
- computerised medical records
- computerised medical record system
- electronic health records
- electronic medical records (EMRs)
- family medicine
- fatigue
- general practice
- ICPC
- International Classification of Primary Care
- primary care
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
- computerised medical records
- computerised medical record system
- electronic health records
- electronic medical records (EMRs)
- family medicine
- fatigue
- general practice
- ICPC
- International Classification of Primary Care
- primary care
INTRODUCTION
Fatigue is one of the most frequently presented symptoms in primary care.1,2 The prevalence of fatigue symptoms among primary care encounters has been estimated to be between 5% and 7%, depending on the definition of fatigue, with substantial associated health system costs.2–10 This common, yet complex, complaint represents a challenge for the primary care provider.3–5 Often, fatigue symptoms can be a non-specific indicator of underlying physiological pathology, psychosocial distress or a combination of causes.11 Regardless of the origin, patients experiencing fatigue symptoms tend to report a lack of energy, feeling weak or being too tired to participate in family, work or leisure activities.9 These subjective feelings of fatigue are what patients report when seeking medical treatment and the provider must then utilise their clinical judgement and investigation skills to deliver the appropriate care. However, the delivery of this care can vary due to differences in practice behaviours, provider characteristics, patient-provider relationships or the perceived burden of the fatigue symptom by the provider and the patient.5,6,12,13 This potentially disruptive and disabling symptom is often regarded as a serious symptom by patients.8 However, its presence in the context of Canadian primary care continues to be underexplored.
The objectives of this study were threefold. First, we aimed to describe the prevalence and characteristics of patients who presented to their primary care provider with the symptom of fatigue. Second, we compared these patterns of health care use to a non-fatigue symptom patient sample, from the same primary care setting. Finally, we explored the determinants of their health care utilisation patterns over a one year follow-up period. This work was conducted using the only known electronic medical record database that holds patient-reported symptom data in Canada.
METHODS
Data sources
Data were derived from the Deliver Primary Healthcare Information (DELPHI) database. The DELPHI database is housed at the Centre for Studies in Family Medicine at Western University, and contains electronic medical records (EMRs) from about 30,000 patients and more than 550,000 patientlevel encounters from 10 primary care practices throughout Ontario, Canada. Established in 2005, this EMR database also contains the only known researchable Canadian primary care data recorded using the International Classification of Primary Care, Revised Second Edition (ICPC-2-R) coding system.14,15 This coding system has notable advantages for use in primary care, particularly its ability to categorize undifferentiated problems, which comprise the majority of a primary care provider’s workload.13,15 A randomly selected sample of patients had their encounters coded using this system (approximately 10% of the total patient population). As of 30 June 2010, there were 3341 ICPC patients contributing to more than 50,000 ICPCcoded visits in the DELPHI database. The ICPC-2-R is structured into two components: the reason for encounter (RFE) codes that are recorded from the patient’s perspective prior to the encounter, and the end of visit codes that are recorded from the provider’s perspective following the visit.16 Here, the terms ‘encounter’ and ‘visit’ are used interchangeably to represent an in-office interaction between the patient and the primary care provider. As shown in Figure 1, the electronic RFE codes capture the patient-reported symptoms, processes or interventions, or previously diagnosed conditions that are the reason for the encounter. The end of visit codes correspond to the symptoms or diagnosed conditions that were actually managed during the visit, from the provider’s perspective. Both sets of codes are recorded by the administrative staff, the nurse or the primary care provider themselves. Ethics approval was obtained from the Research Ethics Board of Western University (Study No. 11151E).

Patient samples
The symptom RFE codes were explicitly used to identify patients for this study, representing symptom presentation from the patient’s perspective. Patients were identified using the RFE code specific to the symptom of fatigue, ‘A04’. This RFE code, entitled ‘Weakness/Tiredness General’ captured various fatigue conditions including fatigue, exhaustion, lassitude, lethargy and post-viral fatigue.14,15 Indeed, this code represented a wide spectrum of subjective fatigue experiences. However, as noted by Lewis (1992), fatigue is best viewed on a continuum within primary care. The comparison patients were identified using any of the remaining symptom RFE codes. That is, the sample of comparison patients came from the same primary care setting and could have presented with any non-fatigue RFE symptom. The fatigue symptom patients became the ‘case’ patient group, while non-fatigue symptom patients were the ‘comparison’ group.
Index visit
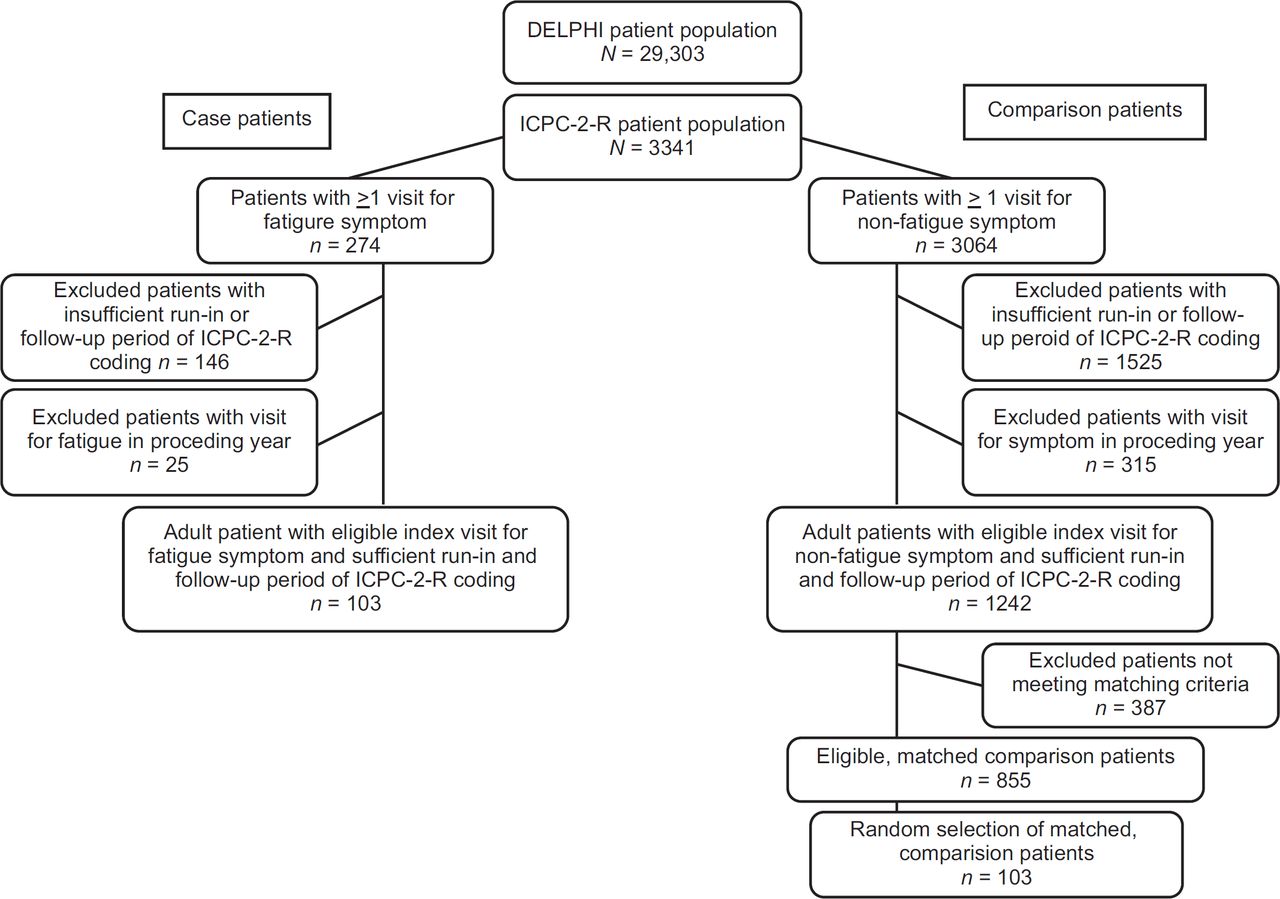
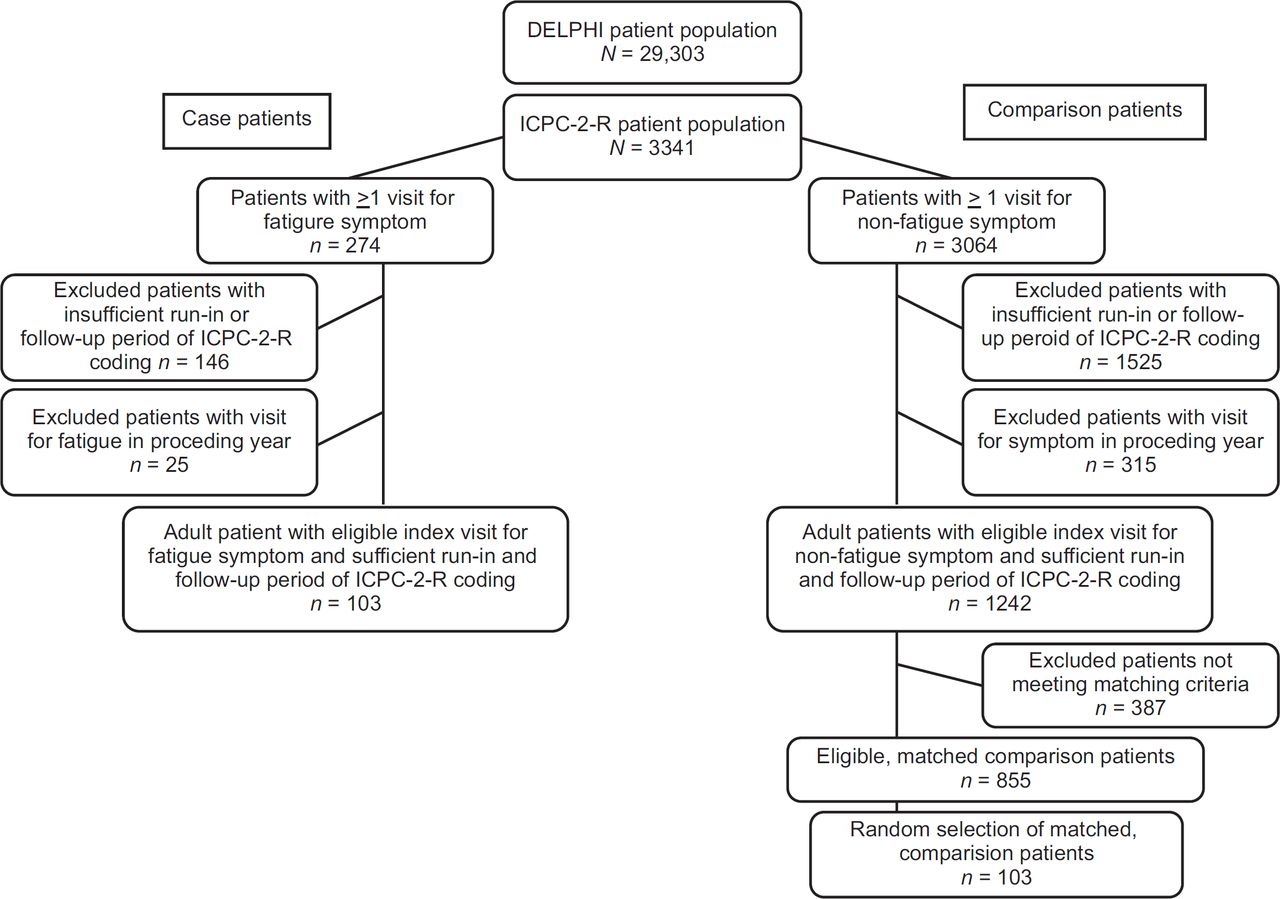
To establish that the symptom presentations were ‘incident’ symptoms, an index visit was identified for each included patient. An eligible index visit for both the case and comparison patients required three components: 1) a complete one year run-in period of ICPC-2-R coding preceding the visit date; 2) a complete one year follow-up period of ICPC-2-R coding following the visit date and 3) the fact that the symptom RFE code presented at the visit date was not presented at any other in-office visit in the preceding year. Only one index visit was identified per patient, and each patient was included only once. A total of 103 eligible case patients were identified, and subsequently matched using a 1:1 matching ratio to 103 eligible comparison patients. Comparison patients who were identified with an acceptable index visit (following the same three components described previously) were matched to case patients on five key variables: 1) patient sex, 2) patient age (age window of ±5 years), 3) practice number, 4) provider number and 5) the quarter (season) of the index visit date. Based on these criteria, the inclusion and exclusion of the case and comparison patients is shown in Figure 2.
Conceptual framework
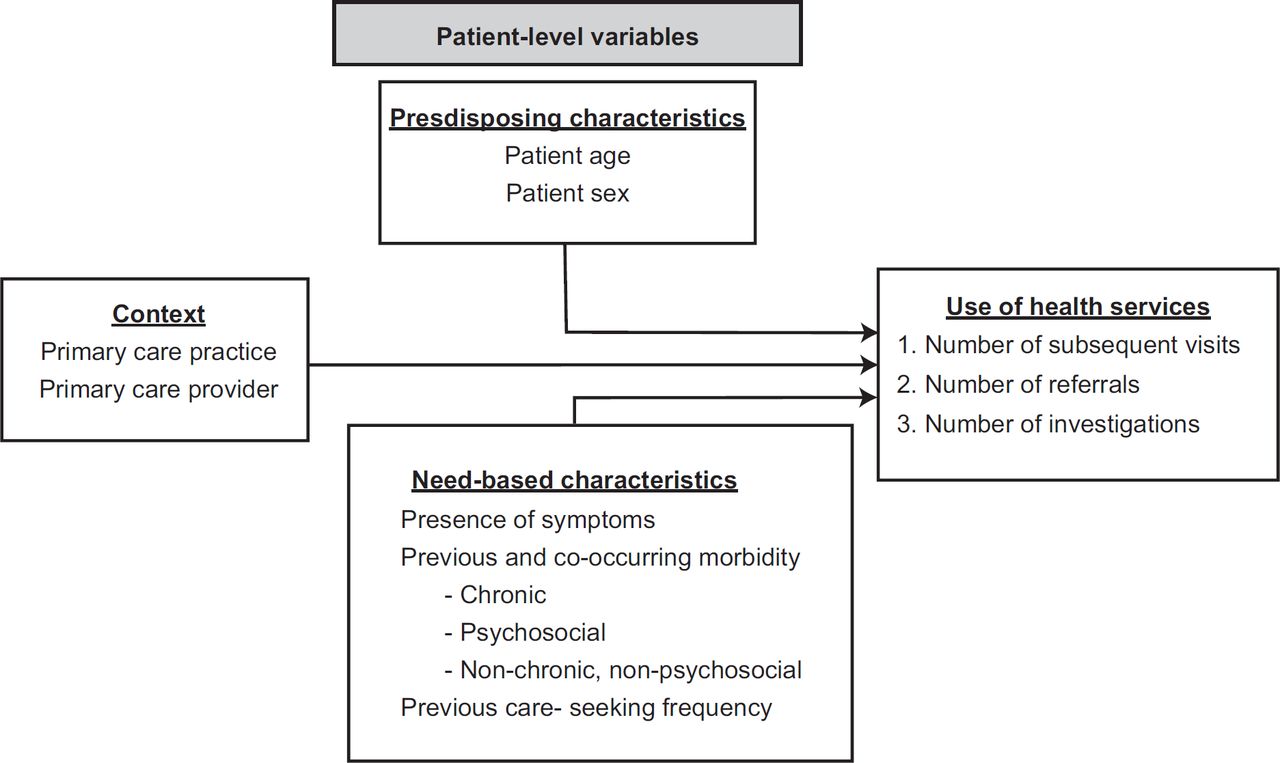
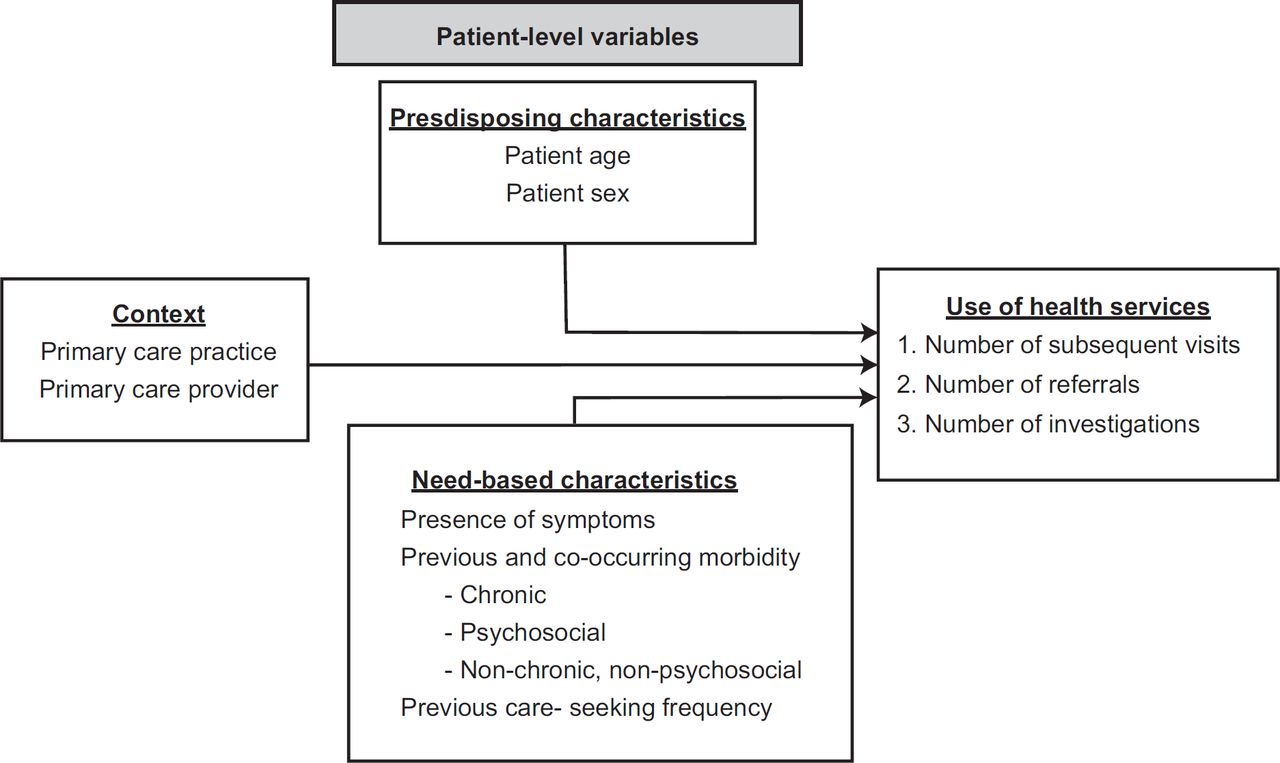
Accounting for the potential determinants of health care use identified in previous literature, as well as the variables that were accessible within the electronic medical record data, an adapted Andersen’s behavioural model of health services use17,18 was created and can be observed in Figure 3. The patient-level predisposing factors included age and sex, while the need-based factors included the presence of the symptom, the number of previous and cooccurring morbidity and the previous care-seeking behaviour of the patient. The overarching context determinants account for practice- and provider-level characteristics that have been shown to influence health care utilisation.19,20 The final component of the adapted conceptual framework was the use of health services, which captured the three main outcome variables.
{kind=link}
{kind=link}
{kind=link}
Outcome measures
Health care utilisation was measured over a one year followup period for both the case and comparison patients. The three main outcome measures were: 1) the number of subsequent in-office visits to the primary care provider, 2) the number of medical referrals received and 3) the number of diagnostic investigations ordered. Each of these count outcome variables were captured using distinct areas of the patient’s EMR, following the index visit date. While the number of subsequent visits did not include the index visit itself, any referrals or investigations that were requested at the index visit were included. If a patient did not have a visit, referral or investigation recorded during the following year, the number of subsequent visits, referrals or investigations was coded as zero, respectively.
Statistical analysis
The statistical analyses were carried out in three phases. First, descriptive analyses were used to examine the baseline characteristics of the patient groups, as well as their baseline levels of health services utilisation. Second, multivariable analyses examined the factors that significantly impacted the health care use patterns of the fatigue symptom patients. Finally, a comparative analysis was used to compare the health care utilisation patterns of the fatigue symptom patients to the matched, non-fatigue patients. As the count data were over-dispersed, a negative binomial regression model was created for each of the three outcome variables,21 adjusting for the necessary covariates (including practice and provider number, patient age, patient sex, previous and co-occurring morbidity and previous care-seeking frequency). A chunk-wise regression was used for analyses. Each incidence rate ratio (IRR) was reported, with all covariates in the model held constant. The significance level was set at 0.05 and all data analyses were conducted using Stata 10.0.22
RESULTS
This study found that 8.2% of the ICPC-2-R-coded patients over a one year period had at least one in-office visit in which the reason for their encounter was fatigue. The majority of these patients were female and over 60 years of age. The baseline characteristics of both the case and comparison patient groups are presented in Table 1. After the matching process was conducted, these patients were of similar age (mean of 63.1 years, median of 64.0 years) and sex composition. However, the fatigue symptom patients had significantly higher previous care-seeking frequency than the non-fatigue symptom group, with 12.1 visits and 9.2 visits in the preceding year, respectively (p = 0.032). The fatigue symptom patients also experienced a large number of previous and co-occurring morbidity, with an average of 7.7 chronic conditions, 2.9 psychosocial conditions and 10.5 non-chronic, nonpsychosocial conditions recorded per patient. Previous and co-occurring chronic conditions were present among 88% of the fatigue symptom patients. ‘Hypertension uncomplicated’ was the most commonly experienced chronic morbidity (19.7%); while ‘diabetes non-insulin dependent’ (12.6%), ‘depressive disorder’ (10.9%) and ‘ischaemic heart disease with angina’ (5.9%) were the next most prevalent chronic conditions. Previous and co-occurring psychosocial conditions were common among approximately 52% of the fatigue symptom patients. ‘Anxiety disorder/anxiety state’ (28.1%) was the most prevalent psychosocial condition. The other most frequent psychosocial conditions among the fatigue patients were ‘relationship problem with partner’ (8.3%), ‘sleep disturbance’ (7.3%) and ‘partner illness problem’ (6.3%). The number of non-chronic, non-psychosocial conditions among the fatigue symptom patients was also significantly higher than the comparison group (p = 0.033).
After adjusting for key covariates in the multivariable analyses (including practice and provider number, patient age, patient sex, previous and co-occurring morbidity, and previous care-seeking frequency), patient-level factors were found to significantly influence the fatigue patients’ use of health care services (Table 2). Previous care seeking was associated with more subsequent visits (IRR = 1.04, p <0.001), fewer referrals (IRR = 0.96, p = 0.002) and fewer investigations (IRR = 0.96, p = 0.006). In addition, female fatigue symptom patients experienced fewer referrals, as compared to male patients (IRR = 0.41, p < 0.001), whereas patients with more non-chronic, non-psychosocial conditions were referred more often (IRR = 1.05, p < 0.001). The results of the comparative analyses are found in Table 3. Overall, the fatigue symptom patients experienced 19% more subsequent visits (IRR = 1.19, p = 0.038) and 68% more investigations (IRR = 1.68, p < 0.001) in comparison to the non-fatigue symptom patients over the year following the index visit. In contrast, the case and comparison patient groups were not significantly different in the number of referrals received from their primary care provider during the one year follow-up period (IRR = 0.97, p = 0.845).
DISCUSSION
Principal findings
This study examined the period prevalence, demographic characteristics, co-occurring morbidity and health care use patterns of patients who presented to their primary care provider with the symptom of fatigue. Overall, this study found a one-year prevalence of 8.2% among ICPC-2-Rcoded patients who had at least one in-office visit to their primary care provider. This prevalence was comparable to a previously conducted Canadian study examining fatigue in primary care patients, which reported a prevalence estimate of 13.6%.4 Over a one year follow-up period, the fatigue symptom patients experienced significantly higher rates of subsequent visits and investigations, as compared to the non-fatigue symptom patients. This study also found that a number of patient-level predictors were statistically significant in their relationship with the outcome variables of interest.
Implications of the findings
Two elements of our findings warrant further interpretation. The first was the fatigue symptom patients’ patterns of health care use. These patients had a substantial level of referral, with almost 65% receiving at least one medical referral during the one year follow-up period, and had characteristics that were significantly related to the outcome. Fatigue symptom patients with previous and co-occurring non-chronic, non-psychosocial conditions were significantly more likely to be referred for specialized care. In comparison, patients with higher care-seeking frequency and patients who were female were less likely to be referred. In fact, male fatigue symptom patients were almost 60% more likely to receive a referral, as compared to female fatigue symptom patients. Both the high rate of referral, and the varying rates of referral based on patient characteristics were surprising. Perhaps these high rates of referral are necessary due to the complexity of the co-occurring conditions (in addition to the fatigue itself); the providers may receive pressure from the patient to provide a referral; or the natural history of the patient’s health simply required a referral to specialized care. Furthermore, female patients and those patients who present more frequently to their primary care provider may have a more established relationship with their primary care provider, therefore requiring fewer referrals. However, as this work did not explore the quality or effectiveness of the care, future research is required to determine if fatigue symptom patients are satisfied with the care delivered in the primary care setting. The second key finding, comparing fatigue and non-fatigue symptom patient groups, was that investigations were ordered 68% more frequently in the following year for the fatigue symptom patients, as compared to the non-fatigue symptom patients and after controlling for all other covariates. This finding may highlight the possibility that fatigue, either new or ongoing, is a symptom of ill health that both providers and patients want to explain and investigate, instead of using the ‘wait and see’ approach. The higher frequency of subsequent visits in fatigue symptom patients further lends support to this interpretation.
Comparisons with the literature
The observed period prevalence of 8.2%, as well as the age and sex characteristics of patients presenting with the symptom of fatigue, was comparable to previous studies that examined a similar patient sample.4–7,12,23 Following their index visit, the fatigue symptom patients had an average of 12.1 visits in the one year follow-up period. This rate was higher than that found by a study conducted among primary care patients in England, which reported an average of 6.2 visits per year among fatigue visitors 23 and a Canadian study, where the fatigue symptom patients visited an average of 3.4 times but were not statistically different from a nonfatigue group.4 Nonetheless, the fatigue patients experienced a substantial burden of previous and co-occurring morbidity, which is consistent with previous literature examining patients suffering from symptoms of fatigue, as well as primary care patients more broadly.24–27
Limitations
When conducting health services research with EMRderived data, a common limitation is the inability to capture patient visits to alternative or allied health professionals. Previous research says that fatigue symptom patients tend to use a large amount of complementary and alternative therapies to manage or treat their symptoms.28 However, the EMR database used in this study was unable to account for these visits. As well, socioeconomic factors (such as income level, education level or employment status) were not available in our database. These predictors may have been important contributors to the patients’ presentation of fatigue or subsequent health care utilisation. The inclusion of these factors could have provided more information of the burden of fatigue on the patient’s life and should therefore be considered in future symptom research. It is also important to consider that fatigue symptom presentation was not confirmed to be the direct cause of subsequent health care utilisation. Instead, this study examined the association between incident fatigue symptom presentation and use of health care services. Finally, the quality of EMR data must be carefully assessed when conducting epidemiological research. More work is needed to definitively measure the validity, completeness, accuracy and comparability of these EMR-derived data.30–33 As the use of these secondary sources of data becomes more routine in both clinical and research settings, its ‘fitness for purpose’ will become an increasingly crucial issue.34
Strengths
Still, a notable strength of regularly recorded EMR data is that they limit other sources of bias. For example, since the data are recorded at the point of care, the potential issues of patient self-report or recall bias are eliminated, avoiding common over- or under-estimates associated with health services research using self-reported follow-up questionnaires or national surveys.4 As noted previously, the use of the ICPC-2-R coding system within the EMR database allowed for the precise identification of reason for encounter data, which is an important perspective in primary care.24 Indeed, this research provides insight into how patients presenting with the symptom of fatigue may be managed by their primary care provider.
Call for further research
Further research in this area is important to better understand the burden of complex and amorphous symptoms, like fatigue. Patient-centered recording systems, including the ICPC-2-R, will help to create more appropriate management and more effective use of health care services. While this work represents the first study in Canada to identify fatigue symptoms from the patient’s perspective, further research could also assess both the direct and indirect costs of fatigue symptom among patients.
CONCLUSIONS
Our study demonstrated that almost one in 10 primary care patient visits were for the symptom of fatigue. The fatigue symptom patients experienced significantly higher rates of subsequent visits (19% more) and investigations (68% more) when compared to non-fatigue symptom patients, as well as high levels of co-occurring morbidity. Although the DELPHI database was not able to capture important variables, such as socioeconomic status or visits to alternative or allied health professionals, a number of patient-level covariates were accounted for in the analyses. Overall, this research presents a novel approach to examining the burden of fatigue among Canadian primary care patients, from a health system perspective, using an EMR database.
Contributions
Kathryn Nicholson, Moira Stewart and Amardeep Thind contributed to study concept and design. Kathryn Nicholson completed data analyses and drafting of the manuscript. All authors contributed to the interpretation of the data and the critical revision of the final manuscript. All authors approved the final version of the manuscript submitted for publication.
Conflict of interest
The authors have no conflict of interest to report.