Article Text

Abstract
Background Recording concerns about child maltreatment, including minor concerns, is recommended by the General Medical Council (GMC) and National Institute for Health and Clinical Excellence (NICE) but there is evidence of substantial under-recording.
Aim To determine whether a simple coding strategy improved recording of maltreatment-related concerns in electronic primary care records.
Design and Setting Clinical audit of rates of maltreatment-related coding before January 2010–December 2011 and after January–December 2012 implementation of a simple coding strategy in 11 English family practices. The strategy included encouraging general practitioners to use, always and as a minimum, the Read code ‘Child is cause for concern’. A total of 25,106 children aged 0–18 years were registered with these practices. We also undertook a qualitative service evaluation to investigate barriers to recording.
Method Outcomes were recording of 1) any maltreatment-related codes, 2) child protection proceedings and 3) child was a cause for concern.
Results We found increased recording of any maltreatment-related code (rate ratio 1.4; 95% CI 1.1–1.6), child protection procedures (RR 1.4; 95% CI 1.1–1.6) and cause for concern (RR 2.5; 95% CI 1.8–3.4) after implementation of the coding strategy. Clinicians cited the simplicity of the coding strategy as the most important factor assisting implementation.
Conclusion This simple coding strategy improved clinician’s recording of maltreatment-related concerns in a small sample of practices with some ‘buy-in’. Further research should investigate how recording can best support the doctor–patient relationship.
How this fits in Recording concerns about child maltreatment, including minor concerns, is recommended by the General Medical Council (GMC) and National Institute for Health and Clinical Excellence (NICE), but there is evidence of substantial underrecording. We describe a simple clinical coding strategy that helped general practitioners to improve recording of maltreatment-related concerns. These improvements could improve case finding of children at risk and information sharing.
- child abuse
- clinical audit
- clinical coding
- informatics
- interdisciplinary communication
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
INTRODUCTION
Child safeguarding (Box 1) includes the recording of concerns and information about vulnerable children in the child’s medical record.1 There is substantial under-recording of child maltreatment and maltreatment-related concerns in primary care records,2,3 which places children at increased risk of harm.4–6 Recording of concerns underpins sharing of information between practitioners, failure of which is highlighted repeatedly as an important factor contributing to serious adverse outcomes.7 The NICE8 and the GMC9 recognise that there is a spectrum of concerns that includes minor concerns. Their guidelines emphasise recording the whole spectrum of concerns. However, clinicians are apprehensive about how recording is perceived by parents and children and the impact of this on the patient–doctor relationship.3
Definition of child safeguarding
In England, child safeguarding is defined by statutory guidance10 as comprising:
protecting children from maltreatment;
preventing impairment of children’s health or development;
ensuring that children grow up in circumstances consistent with the provision of safe and effective care, and
taking action to enable all children to have the best outcomes.
England has a registration-based system for primary care with patients permanently registered with just one practice. Primary care notes are universally computerised with records made at the time a patient is seen,11 although other information from test results and letters is often added to the computerised record outside the consultation. Data entered into the patient record are either coded (a process of assigning a clinical code to the patient record with associated values) or entered as free-text. In current clinical systems only coded data are searchable. Therefore, careful clinical coding of maltreatment concerns is essential to allow a cumulative picture of concerns to emerge and for any kind of proactive management of patients who prompt concern. Good record keeping is also key for effective sharing of child maltreatment concerns.12
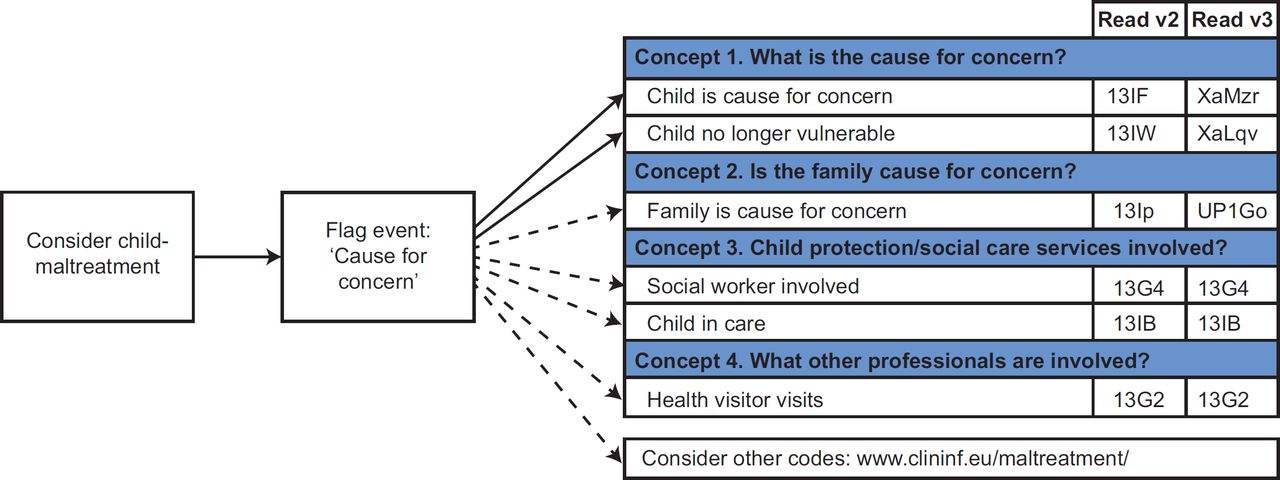
With the aim of improving coding of maltreatment-related concerns in general practice as recommended in NICE guidance, 8 we developed a simple coding strategy (Figure 1) using consensus methods with general practitioners (GPs) from 11 practices in England.3 Here, we report the results of an audit comparing the rate of coding of concerns before and after implementation of the coding strategy in these practices. We also conducted a process evaluation that elicited feedback from practitioners on the potential barriers and facilitators for implementing the change in recording practice.
METHODS
The characteristics of the 11 English practices instigating the intervention have been reported previously;3 importantly, selection of these practices was based on identifying a ‘GP lead’ with known interest in either child protection or other relevant expertise, who could lead the implementation in their primary care practice.
Implementing the coding strategy
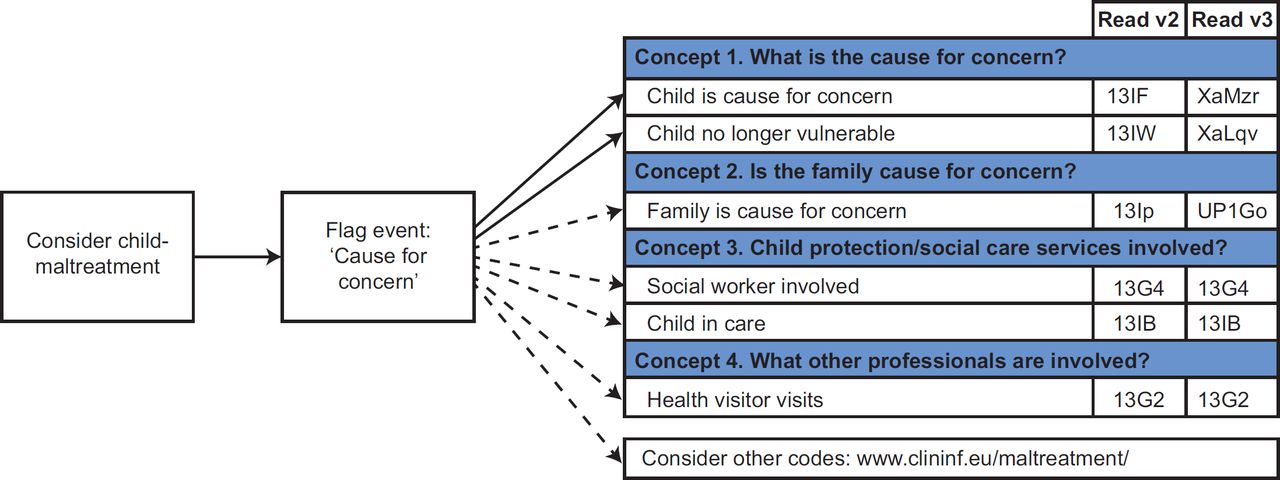
The consensus developed coding strategy was implemented in January 2012 (Figure 2). Participating practices were sent implementation packs in mid-November 2011 to enable preimplementation training and dissemination to members of the practice by GP leads. The implementation pack contained a letter summarising the study progress, a feedback form, a short presentation explaining the coding strategy and detailing the baseline rate of recording maltreatment-related codes.

{kind=link}
{kind=link}
As part of the coding strategy GPs were asked to use, always and as a minimum, the ‘Child is cause for concern’ Read code to document all maltreatment related concerns.
Measuring rates of coded maltreatmentrelated concern
We calculated the average rate of coded maltreatmentrelated concerns per year before implementation in the 11 practices, based on rates in each of two years (January 2010–December 2011). The ‘before implementation’ rates were compared with the rate of coded concerns in the 12 months following implementation (January–December 2012).
In England, most primary care data are recorded using the hierarchical Read coding system version 2, though a substantial minority of practices use read Clinical Terms version 3.13 For our analysis we mapped all the codes to their read two equivalent (mappings available from http://www.clininf.eu/maltreatment/). A total of 350 relevant read codes were identified for extraction and analysis. The complete code list is provided in supplementary file 1 (SF1). The three outcome measures were recording as follows.
Any maltreatment-related code including the subgroups described below; a total of 350 relevant Read codes [SF1 and Table 1(a) and (b)].
Any child protection procedure; a total of 24 codes [SF 1 and Table 2(a) and (b)].
Any cause for concern code (SF 1 and Table 3); 1 code entitled ‘Child is cause for concern’ (SF1 and Table 3).
We calculated the rate of maltreatment-related code recording per 1000 person years of risk, and an adjusted rate standardised for age and gender with 95% confidence intervals. A child could only be counted once in the numerator for each calendar year. Coding rates were, therefore, defined as the number of children with one or more maltreatment-related codes recorded per 1000 person years at risk in one calendar year. We took the mean rate for 2010 and 2011 as the rate for the period before the intervention.
We calculated adjusted rate ratios based on the rate after implementation divided by the rate before implementation. Where rate ratio 95% confidence intervals do not cross parity, we assume the rate difference to be statistically significant.
Process evaluation
Understanding the extent to which practices were exposed to the coding strategy and the extent to which the audit ran as intended (programme fidelity) are important elements of clinical audit and evaluation. Feedback on the approach used to implement the change was collected from GP leads via a teleconference in Feb 2012 and a questionnaire sent out by email in July 2012.
RESULTS
Of the original 11 practices invited to participate one practice was excluded from the final analysis because there was no lead to implement the coding strategy after the GP lead left the practice. The included practices were geographically spread across England, but there was a majority in the major population centres of London and the South East (Table 1). The complete characteristics of these practices have been described in detail elsewhere.3 The included practices used a range of primary care software: three practices used EMIS LV; one practice EMISWEB, three practices INPS Vision, one practice Isoft Synergy and two practices TPP SystmOne.
A total of 25,106 children were included; 20,975 children (36,140 person years) before the intervention and 21,783 children (19,560 person years) after the intervention. The age–gender profile of the population of children included were similar for the before and after intervention periods.
Quantitative findings
During the two years before the intervention 309 children had one or more maltreatment-related event recorded in their records (adjusted mean rate per year 9.1 events per 1000 person years at risk; 95% CI 8.0–10.2; Table 2). In the year, following the intervention 226 children had one or more maltreatment-related event recorded (adjusted rate 12.3 events per 1000 person years at risk; 95% CI 10.7–14.2; Table 1). Rates of any maltreatment-related code increased by almost 40% (rate ratio: 1.4, 95% CI 1.1, 1.6; Table 3). The greatest increase was seen in the ‘cause for concern’ code, especially for the older children (Table 3), although there were also increases in codes relating to child protection procedures following the intervention (Table 3).
Process evaluation
Nine GP leads responded to the process evaluation questionnaire. Seven of these reported disseminating the guidance at a practice meeting. Other methods of dissemination included holding a specific training session, emailing guidance, distributing the information packs and through peer discussion. Six of the lead GPs reported that the majority of the GP within their practice were using the ‘Child is cause for concern’ read code following the intervention.
The simplicity of the coding strategy was cited as the most important factor in assisting implementation by five of the GP leads. Time pressures in general practice, including lack of dedicated time for coding and changing IT systems, were cited as barriers to coding.
In teleconference feedback one GP lead felt education around coding safeguarding concerns had improved overall awareness of safeguarding. Other clinicians stated it was difficult to code this type of issue during the consultation because computer screens are generally visible to patients. There was clinician fear of damaging the patient–doctor relationship and fear of possible legal consequences if patients were aware of these codes being entered into the electronic record. Clinicians who did use these clinical codes stated they tended to code when patient or family had left the consultation room.
Some practices utilised safeguarding data entry templates to facilitate coding but found that free text entry was still used to record safeguarding concerns. Two of the practices reported that local policy and other local drivers meant that they had to use the code list selected by their locality. One local safeguarding board had imposed its own safeguarding template with different codes.
Administrative staff with specific responsibility for recording safeguarding data ‘Safeguarding Clerks’ already existed in one practice. They were responsible for coding data from clinical correspondence under the instruction of the GP clinical lead. They reported using the clinical codes listed. Another practice reported that coding in the consultation was left to the family physician, although a health visitor did have access to the notes and sometimes code cases in the practice computerised medical records. Other practices reported how health visitors are no longer based in the practice, and there was only sporadic sharing of information about children they considered to be a cause for concern.
DISCUSSION
Despite time pressures and competing priorities within general practice, the simple coding strategy increased coding of maltreatment-related problems in children registered at 10 general practices in England. There were increases in codes relating to child protection procedures as well as in the ‘cause for concern’ code, which was the target of the coding strategy.
Comparison with the literature
There is an estimated 4%–16% of children who are subject to abuse annually.5 Despite improvements the coding rates seen here are much lower than this estimate. This gap may be explained by a continued reluctance by GPs to code maltreatment-related problems in the child’s records (14), suboptimal recognition and/or sub-optimal use of health services use by maltreated and vulnerable children.
Limitations of the method
The study is limited by the lack of a control group of practices. We are therefore unable to conclusively demonstrate that the improvements observed were caused by the intervention and not by external factors, such as changes in safeguarding GP training, high profile safe guarding cases and other factors. Because the actual numbers of maltreatment-related codes in each practice are relatively small, the data are particularly sensitive to changes in case-mix within the practice. For example if a vulnerable family with several children were to register during the ‘after’ time period, that may result in a rise in maltreatment-related codes. However, such changes in case mix were unlikely to have occurred in all 10 practices and the increase that we saw exceeded the 10% per year increase which has been reported in analyses of large and representative sample of UK primary care data.2
Generalisability may be limited. GP practices involved were volunteer practices with GP leads that had an interest in child safeguarding or other relevant area of expertise who had been involved in the consensus development of the coding strategy. Implementation of this coding strategy in practices without the same buy-in may prove less effective. However, all UK practice are now required to have a child safeguarding lead, who could act as the ‘lead GP’ for implementation within their practice. Conversely, the impact of this coding strategy may be greater in non-expert practices as their baseline coding rate may be lower; three of the 10 practices in our sample already had coding strategies in place.
Implications of the findings
There is no nationally agreed strategy for coding child maltreatment concerns in primary care. A national guideline would help guide local safeguarding boards and GP computer groups in each locality and facilitate improved recording. Application of the simple coding strategy improved coding of maltreatment-related problems and this approach could underpin any such national strategy. GPs can also adopt this coding strategy to improve their recording of maltreatmentrelated concerns.
Further research
Continuity of care is important in establishing a therapeutic relationship in primary care and has many dimensions from good record keeping to personal continuity.15 As the primary care workforce becomes more mobile, clinical record continuity becomes ever more important. Whilst national guidelines recommend coding the entire spectrum of maltreatment concerns8,9 clinicians are very sensitive to the implications of putting codes into records that may affect their relationship with the patients.16 Although there has been has been little analysis of whether GP concerns about recording safeguarding data are reflected in patient’s attitudes and beliefs, indirect evidence suggests that at least some parents are deterred from seeking care from a GP due to fears about their surveillance role and potential for a long-lasting and stigmatising label to be given to the child or family.17,18 Further analysis is required into how acceptable it is to patient’s to have a ‘cause for concern’ code in their child’s record. This is particularly important as patients have increasing access to their own records and especially as the UK’s Department of Health has mandated that all family practices should offer online access to the records of their patients; effective in 2015.19
Given the policy emphasis from NICE guidance and GMC recommendations on recording, the use of read codes is a surrogate marker for the quality of child safeguarding in general practice. It is likely that recording of concerns is a necessary but not sufficient part of responding to child maltreatment and related problems. Whilst recording and coding concerns is the first step in responding we do not know how coding changes subsequent management of the child and family or what the impact of improving coding is on child or family outcomes. A quality improvement trial involving larger number of practices would enable exploration of whether care benefits for vulnerable children resulting from improving data recording outweigh the risks and concerns surrounding coding.
CONCLUSION
A simple coding strategy can improve the coding of maltreatment-related concerns by GPs. Further research should investigate how recording can best support the doctor–patient relationship.
Acknowledgments
The authors would like to thank the participating practices and GP leads.
References
Footnotes
Funding The study of 11 practices was designed, registered and funded as an audit. The audit was coordinated by the RCGP-Clinical Innovation and Research Centre and funded by the Health Care Quality Improvement Partnership. Jenny Woodman was funded by a Medical Research Council/Economic and Social Research Council interdisciplinary Ph.D. studentship. Ruth Gilbert is an investigator with the Department of Health funded Policy Research Unit for Children, young people and families.
Ethical considerations This study observed the quality of recording of safeguarding concerns and the simple intervention was educating clinicians about how to implement a nationally agreed standard for recording. It is therefore defined as a clinical audit and as such did not require ethics committee review.20 All practices consented to the extraction of anonymised data for audit purposes.
Competing interests The authors have declared no competing interests.