Article Text

Abstract
Background and Objective To increase patient access to healthcare, the U.K. Government has encouraged new technology-based approaches including telephone consulting, email-consulting, short message service messaging and video consulting over the Internet. However, little is known about patient acceptance of video consulting as a consulting method. We aimed to explore primary care patients’ views on the possible utility of video consulting.
Method and Results We used semi-structured interviews to survey 270 patients in Lothian. Three diverse general practices were purposively chosen. Sequential patients attending the practice at different times of day were invited to participate. Patients were asked to indicate their level of computer proficiency and provide their views on the use of video consulting and what specific applications it might have. We found that 50% (95% Confidence Interval (CI) 43.9%–56.1%) of patients would use video consulting. Patients under 60 years were over two times more likely to use it (Odds Ratio (OR) 2.2, 95% CI 2.1–6.6) and evidence of a positive trend between increasing computer proficiency and those who would video consult was found (χ2 = 43.97, p < 0.0005, n = 270). Patients who had used commercial video services (such as Skype) were approximately six times more likely to favour video consulting than those who had not (OR 5.9, 95% CI 3.5–9.9).
Conclusions This suggests strong patient interest in video consulting in primary care. However, it is possible that in the short to medium terms, there may be access inequality favouring younger and more technically able people. Further studies are needed to determine the content, safety, efficacy and cost effectiveness of employing this medium.
What this study adds:
Novel evidence is provided for patient acceptance of video consulting as an alternative consulting technology.
Accepting patients belonged to a specific subgroup that were younger, more computer proficient and had used commercial video services before.
Patients identified video consulting as useful for minor illness and general advice, highlighting that it could save their time.
Video consulting was viewed as inappropriate for consultations where an examination is required and concern was expressed for it being less personal.
- Access to care
- consultation
- patient–physician relations
- telehealth
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Promoting fast and easy access to healthcare has been a priority over a number of years1,2, but with increasing demand on the U.K. National Health Service, new ways are being sought in which to deliver this. The U.K. Government has recently prioritised flexible access by promising that email, Skype and telephone consultations will be used to supplement face-to-face appointments with general practitioners (GPs).3 Investigations into alternative methods of contact between doctors and patients have been conducted4,5 with a focus on the use of information technologies. These have described perceived low patient demand by health-care professionals and concerns about the reliability, security and confidentiality of these technologies.5–8 Patients have described both advantages and disadvantages of telephone consulting, which is now used widely. However, there is little high quality evidence exploring the efficacy and applicability of these alternative technologies, particularly in a U.K. setting.5,9–11
Previous research into alternative technologies has mainly focused on telephone consulting6,10 and has contributed to progress in understanding its application12 and impact on the doctor–patient relationship,13–15 particularly in primary12,15 and out-of-hours care.16 The possible utility of email and short message service has also been investigated.17,18 Recently, attention has turned to video consulting, since free video communication services such as Skype, FaceTime, Jabber and Google Hangout have become increasingly popular in both social media and business sectors.6,19 Whilst in the past video consulting has been used within telemedicine to improve access for patients living remotely,19,20 the advent of free video communication services may allow viable, fast and easy alternatives to face-to-face consulting for all patients with supporting devices.9 These include smart phones, tablets, laptops and desktop computers. The views of healthcare professionals7 and practice managers in primary care8 regarding the utility and likelihood of the uptake of video consulting have previously been described although the studies were carried out prior to the large-scale adoption of these technologies by the general public. In addition, no similar survey of patient views has been undertaken.
Aims of study
This is the first study to investigate patient attitudes towards video consulting with their GP. We sought to establish how widely used video communication, for social and business reasons, is amongst primary care patients and whether there is a demand for using it as an alternative method of consulting. This included demographic evaluations to investigate access inequality, which had been highlighted as a concern for the elderly and socio-economically deprived.4,6,7
Method
We conducted semi-structured interviews. As no formal evaluation tool existed10 in this field, our interview outline was based on elements of innovation adoption theory21 (including experience and knowledge of the intervention or related technology and the perceived advantage of the proposed technology to different social groups. See Box 1 for the full description). The schedule was piloted on a convenience sample (n = 12) and subsequently adjusted. Ethical approval was through a process approved by the University of Edinburgh research committee for medical undergraduate students pursuing low-risk research.
Box 1
Diffusion of innovations theory aims to describe a mechanism as to why and how quickly ideas and novel technology are adopted by societies. Rogers21 proposes that four fundamental features influence how new ideas spread: the innovation itself, communication channels, time and the social system. This process is heavily dependent on the existing knowledge, skills, experience and training existing in the society into which the innovation is introduced. The innovation has to be adopted widely in order to become self-sustaining. The theory describes a point during the adoption at which an innovation reaches critical mass and categorises adopters into five groups: innovators, early adopters, early majority, late majority and laggards.
We approached a total of 296 patients within three general practices in the Lothian area representing different demographic backgrounds: a socio-economically deprived rural practice; an urban practice with younger patients of varied nationality; and an urban practice in a socio-economically advantaged area of Edinburgh. Data collection took place over two consecutive days in each practice and was conducted throughout the opening hours in order to gain a representative sample of the primary care population. All patients aged 18 years or older attending their practice for an appointment were approached in the waiting room and asked if they were willing to participate in a five-minute interview. Consenting patients were initially asked questions concerning their postcode, age, sex, GP attendance, access to computer devices that permitted video communication and self-rated computer proficiency. Participants were asked to describe their computer proficiency as ‘good’, ‘average’ or ‘poor’. We then asked patients about their use and enjoyment of video communication socially or at work. Finally, patients were asked to indicate whether they thought they would use video consulting with their GP. Free response questions followed to explore both their reasoning and potential applications for video consulting, with specific patient types or health problems.
The data was analysed using SPSS version 21 and Minitab version 17.0. We used the exact method for obtaining a 95% confidence interval for the proportion of patients who would use video consulting with their GP and the proportion of patients who reported having regular access to a computer device either at home or at work. The remaining analyses involved the use of odd ratios and corresponding 95% confidence intervals, the chi-square test of association and the chi-square test of linear trend. Using the Scottish Government’s Postcode Lookup,22 patient Scottish Index of Multiple Deprivation (SIMD) quintiles were determined from respondent postcodes. Patient ages were categorised into an ‘older’ group aged 60 years or over, based on the WHO recommendations,23 with the remainder forming a ‘younger’ group. We explored patient access and use of technology according to demographic factors. In addition, we tested for a monotonic trend in each of patients’ access to technology and patients’ previous video call usage according to level of affluence. Also, we analysed patient willingness to use video consulting with their GP in relation to their demographic background and previous experience of video call use.
We tested for an association between this response and each of patients’ SIMD quintile and computer proficiency. We also tested separately for evidence for an increasing monotonic trend in willingness to use video consulting according to each level of computer proficiency and the extent of previous video call usage. Furthermore, we tested for an association between willingness to use video consulting and each gender and age group. A significance level of 0.05 was assumed for all hypothesis tests. We used a thematic coding frame to analyse free text answers. This involved reading answers multiple times and coding them so that each distinct patient comment was given a separate code. This allowed multiple codes to apply to a single patient response. Code frequencies were then counted and analysed.
Results
Demographic findings
A total of 270/296 (91.2%) patients consented to being interviewed. Patients declined mostly on the grounds of feeling too unwell, anxiety about missing their appointment or poor understanding of the English language. The demography of the sample is presented in Table 1. The sample represented a range of ages, social deprivation and gender. Postcode disclosure was declined by 29 patients (11%) and year of birth by 22 (8%).
Technology access and Use
Most respondents (229/270, 84.8%, 95% CI 80.0–88.9) reported having regular access to a computer device either at home or at work; and 43% of patients rated themselves ‘good’ in terms of computer proficiency with 31.9% rating themselves ‘average’ and 25.2% rating themselves ‘poor’. A good level of computer proficiency was reported by more patients under 60 years than those 60 years or over (52.4% 18–59 years versus 19.2% ≥ 60 years: χ2 = 50.334, p < 0.0005). There was also evidence of a decreasing monotonic trend across levels of computer proficiency for older patients, with 56.4%, 24.4% and 19.2% of patients of age 60 years or over reporting poor, average and good levels of proficiency, respectively (χ2 = 50.334, p < 0.0005).
Furthermore, patients under 60 years were nearly seven times more likely to have regular access to a computer device (OR 6.8, 95% CI 3.3–14.0). There was evidence for an association between affluence and regular access to computer devices (90.1% of SIMD quintile 5 (most affluent) versus 75.0% of SIMD quintile 1, χ2 = 4.590, p = 0.032, n = 117). There was not, however, evidence of a consistent positive trend towards regular access across levels of affluence, with 75.0%, 71.7%, 83.3%, 94.3% and 90.1% of those reporting regular access falling under quintiles 1 to 5, respectively. There was an association between level of affluence and computer proficiency (51.9% from SIMD quintile 5 versus 25.0% from SIMD quintile 1, χ2 = 9.632, p = 0.008, n = 117). Video communication had been used by 51.9% (140 out of 270) of patients. Those under 60 years were approximately four times more likely to have used it than those 60 years or over (OR 3.7, 95% CI 2.1–6.6, n = 248). There was an association between level of affluence and previous video call usage (61.7% from SIMD quintile 5 versus 33.3% from SIMD quintile 1, χ2 = 8.067, p = 0.005, n = 117) with evidence for an increasing monotonic trend in previous usage according to level of affluence with 33.3%, 45.3%, 44.4%, 60.0% and 61.7% of those reporting previous access falling under SIMD quintiles 1 to 5, respectively (χ2 = 9.799, p = 0.002, n = 241).
Willingness to use video consulting
When asked whether they would use video consulting with their GP, 135/270 (50%, 95% CI 43.9%–56.1%) of patients responded ‘yes’. There was an association between willingness to use video consulting and computer proficiency (χ2 = 48.420, p <0.0005, n = 270) and evidence for an increasing monotonic trend towards this positive response according to level of computer proficiency, with 7.4%, 34.8% and 57.8% who reported ‘yes’ rather than ‘no’ falling under SIMD quintiles 1 to 5, respectively (χ2 = 43.970, p < 0.0005, n = 270). Participants who had previously used video communication were approximately six times more likely to give a ‘yes’ response (OR 5.9, 95% CI 3.5–9.9, n = 270). There was an association between the frequency of previous video communication usage and this response (χ2 = 12.696, p = 0.013, n = 134) with an increasing monotonic trend in willingness to use video consulting according to the extent of previous video communication usage (χ2 = 11.152, p = 0.001, n = 134). Patients under 60 years were more than twice as likely to be willing to video consult their GP than those 60 years or over (OR 2.2, 95% CI 1.3–3.8, n = 248). However, there was a lack of evidence for an association between the response to this question and any one of the gender (χ2 = 1.543, p = 0.214, n = 270) or the level of affluence, both on comparison across all five SIMD quintiles (χ2 = 1.543, p = 0.214, n = 270) and on comparison across SIMD quintiles 1 and 5 only (χ2 = 1.376, p = 0.241, n = 117).
Free text questions
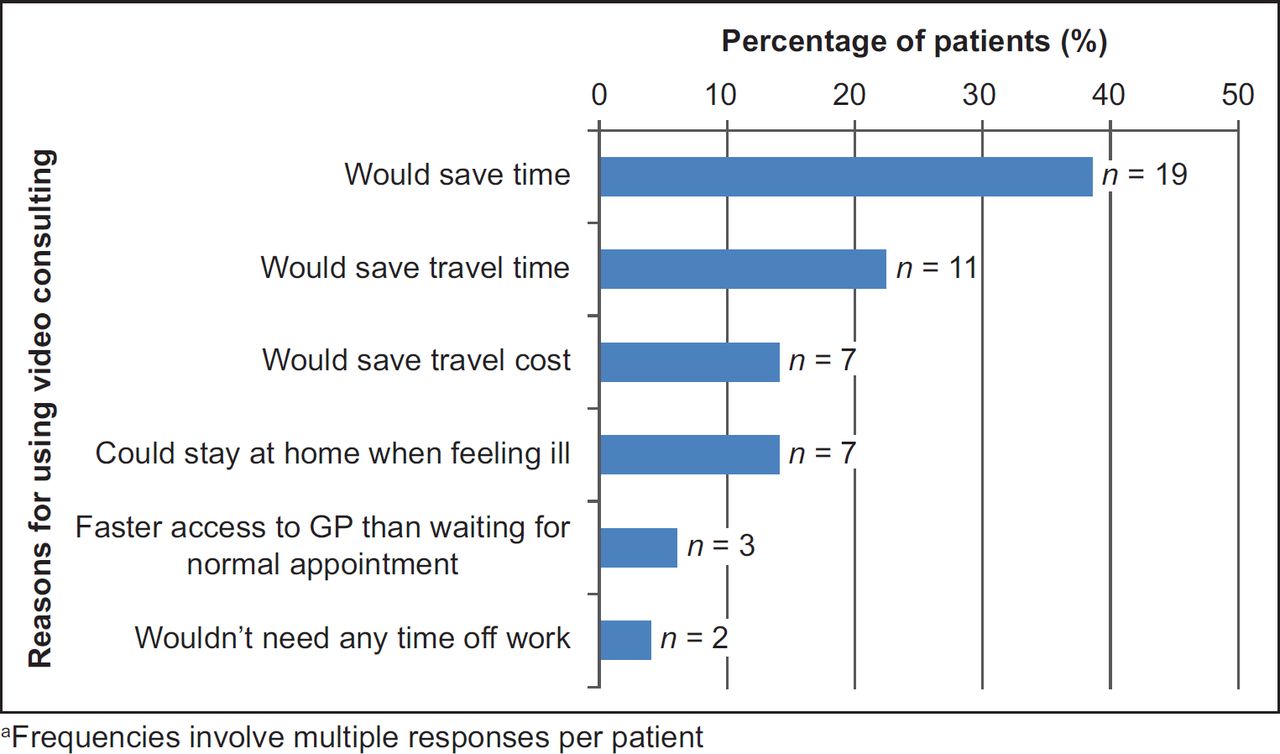
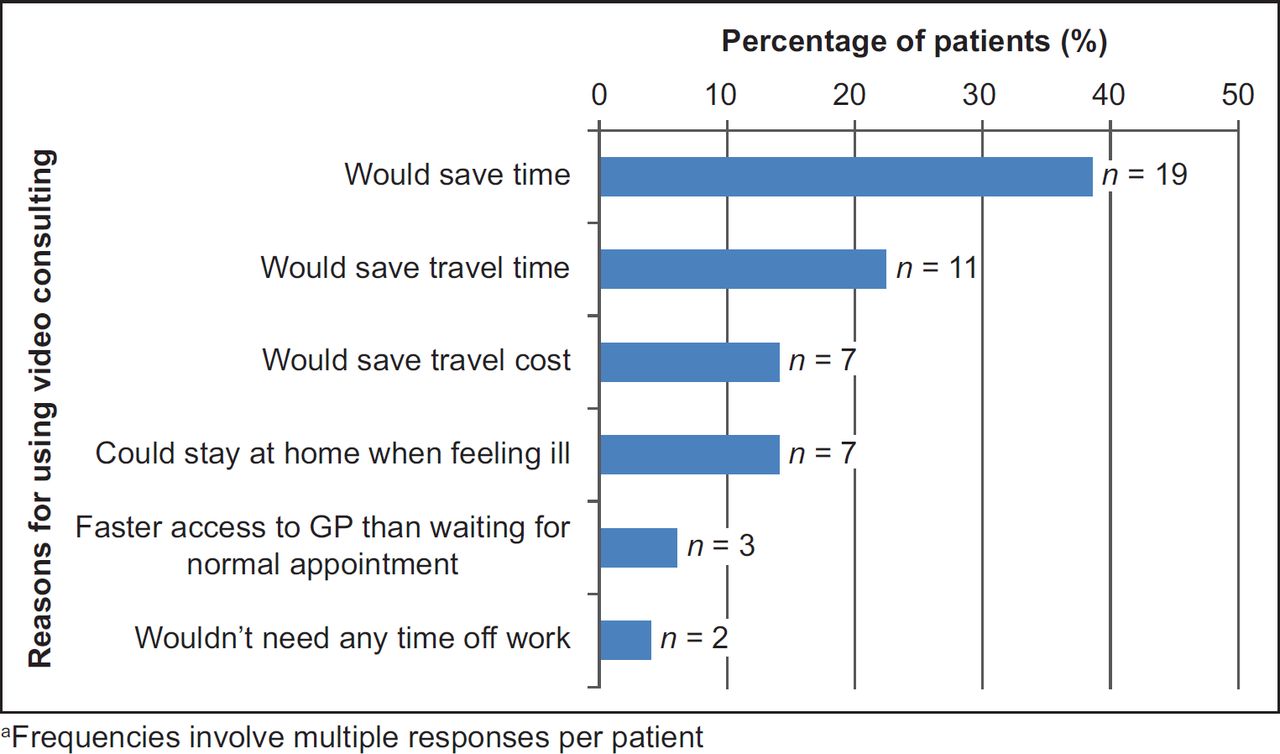
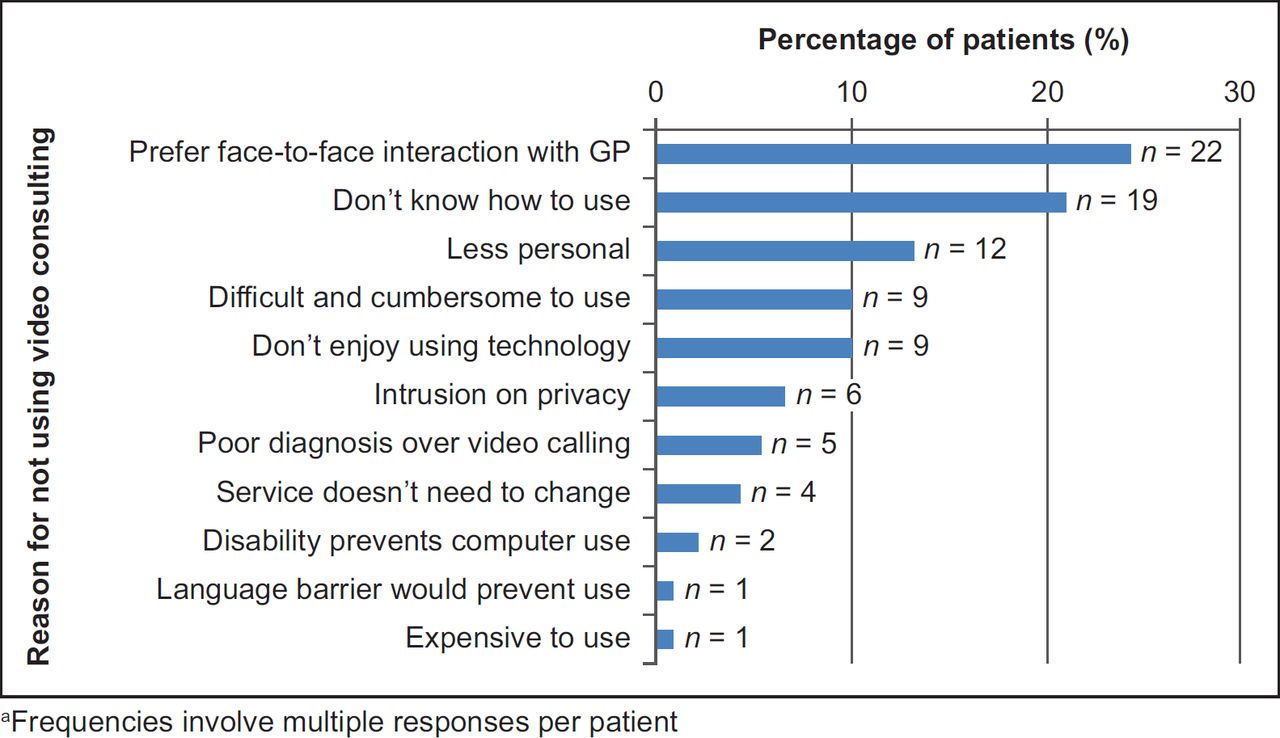
Of the 270 respondents, 139 (51.5%) gave reasons about why they would or would not video consult with their GP. Figures 1 and 2 list reasons for using and not using video consulting, respectively, with the most common positive reason mentioned being that it would save time (n = 19) and the most common reason for not using it simply that patients preferred seeing their GP face to face (n = 22).

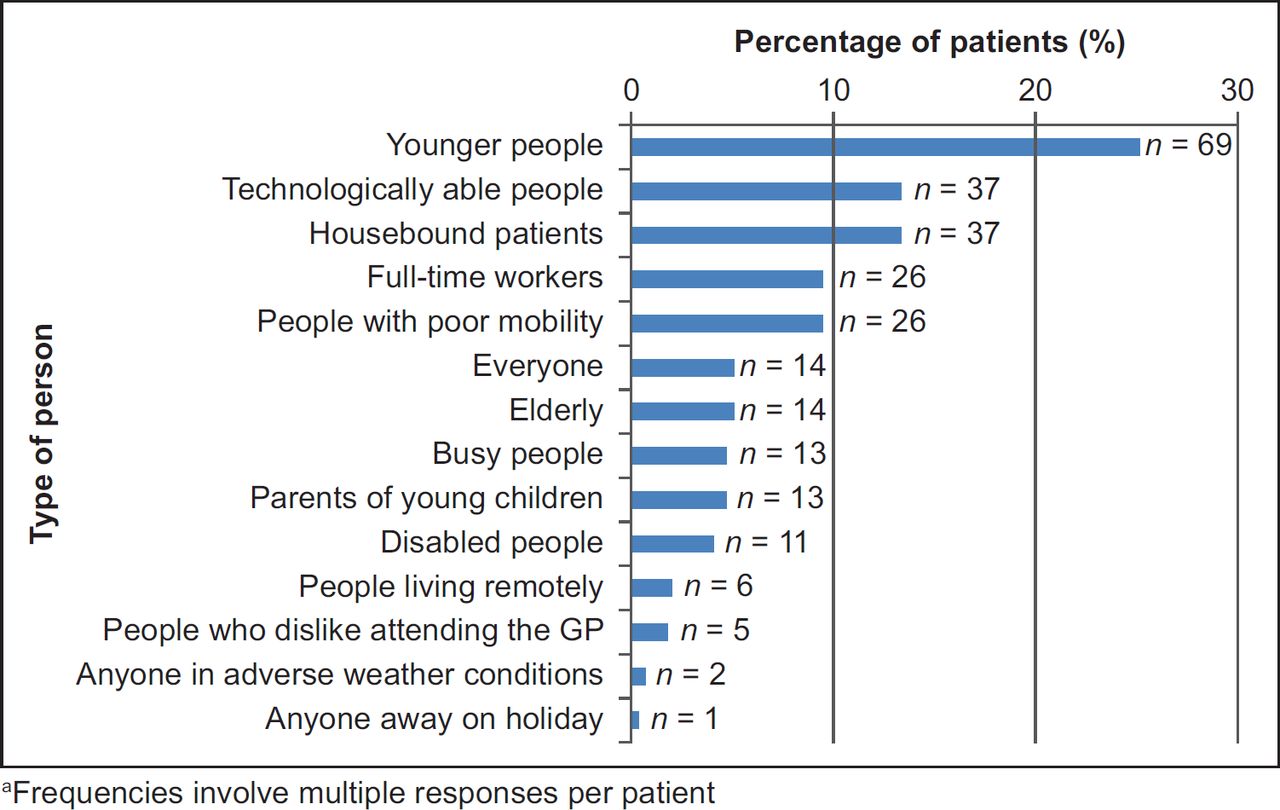
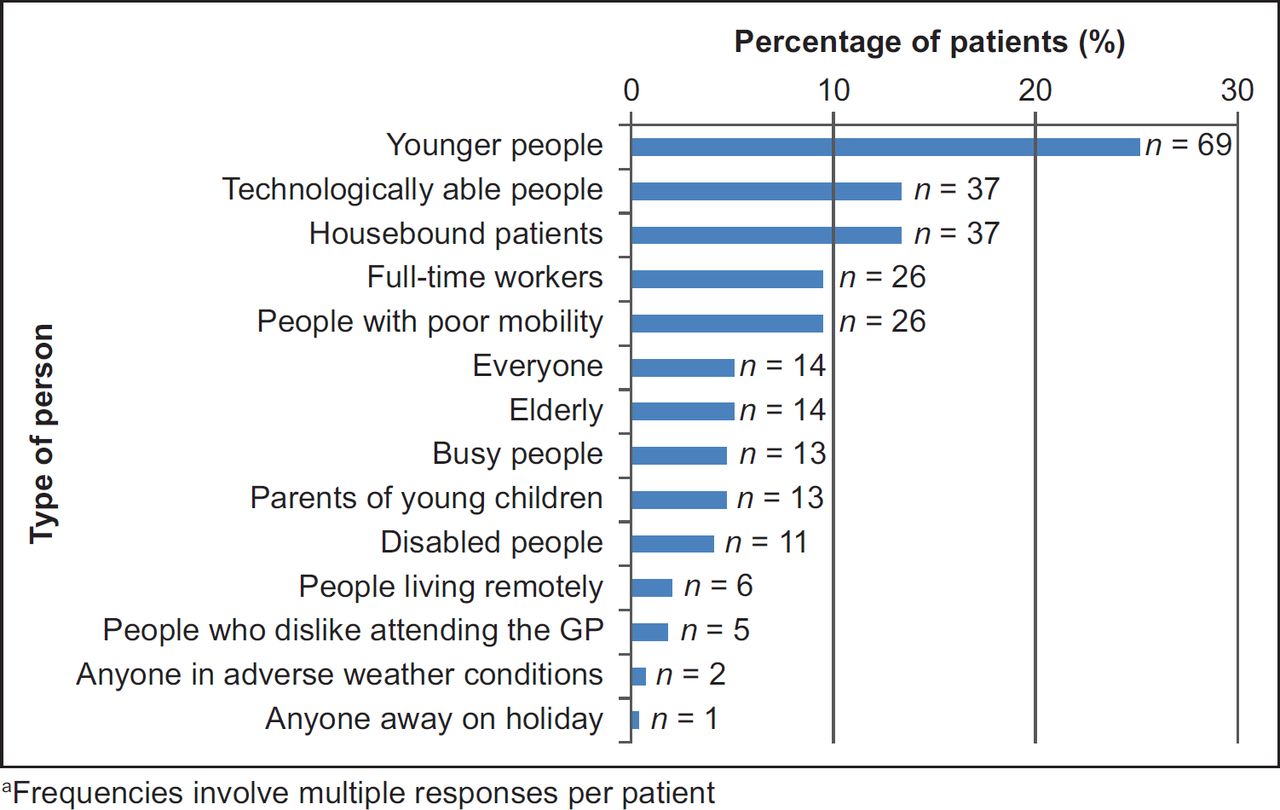
When respondents were asked to identify the types of person who, in their opinion, might find video consulting with a GP most useful, 74.8% (n = 202) patients responded. Younger (n = 69), technologically able people (n = 37) and housebound people (n = 37) were among those groups most often chosen (Figure 3).
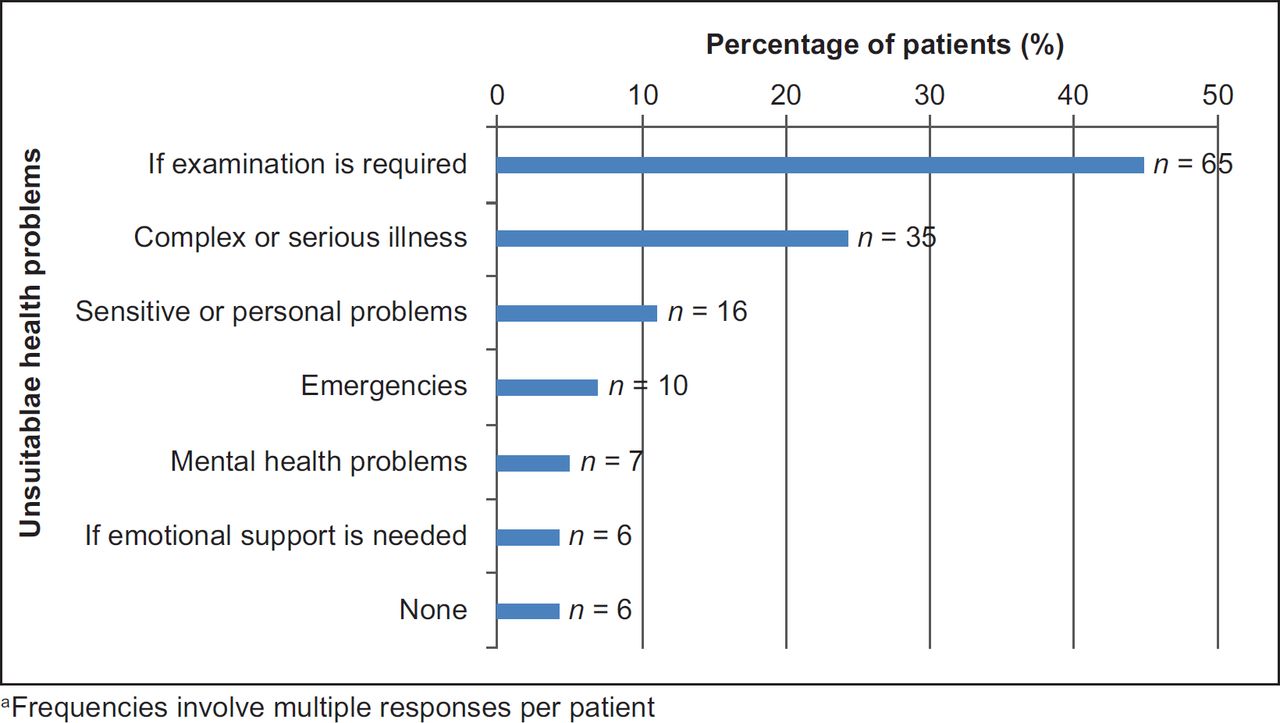
Respondents were finally asked to suggest health problems that they deemed suitable for a video call consultation with a GP and by contrast, less suitable problems. Of the 270 participants, 65.6% (n = 177) identified suitable health problems and 53.7% (n = 145) suggested unsuitable health problems. Minor illness (n = 62) was cited as the most common health problem that could be dealt with by a video call, followed by the belief that most problems seen by a GP would be suitable for a video call (n = 31) (Figure 4). The majority of respondents responded that video consulting would be less suitable for health problems requiring a physical examination (n = 65) (Figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
Principal findings
Fifty percent of patients in this study indicated that they would use video consulting with their GP. Perhaps unsurprisingly, this was associated with greater computer proficiency and experience of personal video communication use and also with the age of the participants.
Implications of findings
There is a clear desire among a relatively large proportion of the population for video consulting with their GP for a range of problems. Although 85% of respondents had regular access to appropriate technology, we also found that there was a clear socio-economic and age divide in access to this technology and ability to use it. This has been identified in other studies relating to eHealth.4,6,7 However, despite this, participants’ socioeconomic status was not a significant factor in their desire to use video consulting. The finding that non-users are significantly more likely to be older has important implications since the elderly are known to utilise GP services more frequently and are more likely to have mobility problems.24 It is not known if the use of video consulting will be associated with a shortening or lengthening of consultations, or indeed if increased convenience may increase demand for consultations. However, it is possible that if video consulting results in efficiency savings, as has been postulated for other technologies, it could increase the availability of more traditional consultations for all groups.4,17
Comparison with the literature
The considerable proportion of patients accepting of video consulting contrasts greatly with the previously held perception by healthcare professionals that there is low patient demand for alternative consulting methods.7,8 Whilst this is the first study to investigate patient acceptance of video consulting, our results are similar to the studies of other consulting technologies such as telephone and email,18,24 where participants identified time and financial savings as advantages of alternative technologies. It is worth noting, however, that research has demonstrated an increase in repeat consultations in the two weeks following a telephone consultation,25 which may negate the time saved if the same holds true for video call consultations. Participants in this study indicated that they thought video consulting would be most useful to younger and more technologically able people. People confined to home, with poor mobility, or fulltime workers were the next most commonly identified groups considered likely to benefit. Again, this parallels findings from research into telephone consulting.13,26
A discussion of minor illness and general health advice was identified as most suitable content for a video call consultation by patients. This aligns with safety concerns regarding other forms of alternative technology where both patients and doctors expect to discuss only simpler problems.13,27,28 Although patients were not forthcoming with their reasoning in this study, previous work has shown that GPs feel uneasy with alternative technologies due to perceived increased clinical uncertainty, with the absence of visual clues.6,24,29 However, previous research dealt mainly with non-visual forms of communication and it has been postulated that using video consulting may alleviate this uncertainty since a degree of visual assessment could be made.28 Patients did seem to recognise the potential benefit for ‘visually obvious’ illness in their comments, but further evidence will be needed to ensure that video consulting is clinically safe for this purpose. Among the other identified suitable problems, follow-up for chronic disease and prescription reviews have also featured in previous research,10,30 which may indicate an opportunity for video consulting to meet this particular need. Another area where video consulting has been found to be particularly appropriate is in the management of mental health problems,31 where telephone consulting has been considered in previous qualitative research to fall short due to the loss of visual cues.28
Patients identified the need for examination as a barrier to video consulting, which has also been highlighted as a concern by GPs24,28,29 using telephone consulting. This may be why patients also perceived the discussion of complex or serious illness to be unsuitable for video call consultations.
Strengths and limitations
The high response rate (91.2%) ensured that responses were representative of those attending the practices. However, the majority of participants fell into the under 60 years category and the most common SIMD quintile for participants was quintile 5. This may have allowed sample bias in favour of using newer technologies since patients from these categories were also found to be more computer proficient and have better access to technologies. Likewise, it is possible that differences between age groups may reflect access to the appropriate technology and training, rather than any bias against it. The practices sampled also already used telephone consulting extensively, which may have strengthened patient predisposition towards video consulting.12,19 In addition there was missing data, mainly due to declined postcodes (11%) and ages (8%), but we feel that this is unlikely to affect our conclusions. Our study was conducted in three practices in one U.K. region, which may limit its generalizability. Interpreters were not used in the study and so people who did not have a good command of spoken English were excluded. This group has difficulty with telephone consultation28 and the same may be true of video consulting. The brief interview technique perhaps limited the comments from participants and conducting further in-depth interviews and focus groups may have yielded further information regarding the exact place video consulting has within general practice.
Conclusions
This project has found evidence that video consulting is accepted as an alternative consultation method by many primary care patients. These patients were younger, more computer proficient and had more experience of video communication socially or in business. However, before full-scale implementation of such a service can be considered, further research is required to determine how such consultations differ from more traditional consultations in terms of complexity of problems; content; safety; impact on equity; and both patient and clinician resource use.