Article Text

Abstract
Background Systematic reviews have suggested that time spent on computerrelated tasks increases consultation length. However, these reviews pre-date the current ubiquitous use of computers in U.K. general practice.
Objective As part of a U.K. national study of the influence of information technology (IT) on the interaction between patients and healthcare professionals during consultations, we explored how IT functions affected time allocation and styles of computer use during general practitioner (GP) consultations.
Methods We drew on multichannel video recording of consultations and measured consultation phases and the duration of computer-related tasks. We related measures of actual time to GP’s interpretation of computer use elicited in qualitative interviews.
Results Our sample included recordings of 112 consultations from 6 GPs in three practices. The computer was used for about one-third of the greater consultation. However, its use was concentrated pre- and post- the patient consultation. The workflow of consultation was exemplified through six computer use cases. Most functionality was accepted and accommodated within the consultation, though disruptive and time-consuming tasks were generally delegated to administrative staff. Recognised styles of computer use (minimal, block and conversational) were apparent, but applied very flexibly by GPs according to the nature of the consultation.
Conclusions In contrast to earlier reports, contemporary computer use does not appear to have lengthened consultations. GPs adopted different styles of computer use in different consultations, challenging classifications that seek to stereotype GP computer use. Designing systems that support this versatility require an understanding of the fluid application of computer use within consultation structure.
What is already known
Although computers have been used in U.K. general practice consultations for four decades, there are on-going concerns about the amount of time new computer functions may take.
General practitioners (GPs) adopt different styles of computer use during patient consultations.
What this paper adds
This study found no evidence that computer use increases the length of consultation.
The electronic health record is now the accepted norm in U.K. primary care, and in general, GPs do not express concerns about the time allocated to undertaking computer-related tasks within the consultation.
Implications for clinical practice
Despite some preferences in how they used the computer within the consultation, all the GPs readily adapted their style to suit the individual consultation.
Understanding of the skilful versatile strategies employed by GPs may be a useful design resource and inform clinical training.
Computer designers need to address the tension between ordered computer function and the fluid demands of a clinical consultation.
Commons license http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Systematic reviews have suggested that time spent on computer- related tasks increases the length of the consultation,1–3 though some studies have associated longer consultations with less computer use.4 Although time may be saved by functions such as computerised repeat prescribing,5 this may not be reflected in an overall improvement in time efficiency,6 as illustrated by a study of poorly designed computerised decision support. 7 Analysis of general practitioners’ (GPs’) actual computer use (clock time) and their perceived time (user experience) should enhance understanding of how computer use fits with the process and rhythm of time-managed consultations,8 and provide insights for software development, implementation and clinical training.
Classification of computer use
‘How long things take’ has been a focus of early studies of activities within the consultation. For example, TIMER (a tool for analysing tasks within the consultation) identified the number and types of problems addressed in the consultation, and rated doctor and patient activity as (a) physical (e.g. administration and examination), (b) verbal (e.g. information giving) or (c) secondary tasks (e.g. exploring patient concept and decision making) in 5-s intervals and totalled for the consultation.9 A more recent time and motion study evaluated how electronic health record (EHR) use in primary care affected time utilisation. Physician and patient behaviours were assigned to categories including: ‘major’ [e.g. computer – looking for notes (clinical records)] and ‘minor’ (e.g. checking lab result) and particular activities like looking, reading and writing (e.g. orders, emails or forms).10 As computer use is now the norm in U.K. general practice, a form of goal-oriented task analysis11 is appropriate for evaluating regular use of EHR systems in consultation practice. ‘Use Case Diagrams’, a feature of the Unified Modelling Language (UML), are commonly employed by systems analysts to describe an interaction between an actor and a system to achieve a particular goal.12 Framing computer use in the clinical consultation using this method can facilitate an interpretation of the interactions that can be shared between designers, implementers and user practitioners.13–15
Structure and order: styles of computer use
Different styles of use have been characterised.16,17 Clinicians have been classified as ‘minimal users’ who record information at the end of the consultation either from memory or transcribing handwritten notes, ‘conversational users’ who multitask and record information throughout the consultation and ‘block users’ who interrupt the consultation to use the computer.17,18 Style may be ‘systematic’ (working though forms and templates) or ‘personalised’ (e.g. recording data as it emerges naturally during the consultation).19 By 2008, there was little evidence that clinicians had learnt to multitask, instead developing strategies to ‘insert’ dedicated time for computer use into the consultation.20–22 Analysis of speech in 10-min consultations for hypertension revealed an average of 2-min silence when clinicians concentrated on the computer. 23 In contrast, GPs reduced their use of the computer during consultations of a psychosocial nature.24 A recent observational study showed that the GPs were more sparing with their use of the computer in 2008 than in 2001; however, it was not clear whether the computer was integrated better into the consultation or whether the GPs had shifted computer use outside the time with patient.4
These studies, however, pre-date the shift over the last decade towards ‘paper-light’ practice in the UK. As part of a national project, ‘Healthcare INTERACTions and the impact of Information Technology (INTERACT-IT)’, funded by the National Health Service Connecting for Health Evaluation Programme,25 we therefore sought to update the evidence on duration of computer use, the computer tasks performed and the styles adopted by GPs in the context of contemporary consultations in which computer use is the norm.
Methods
A detailed account of the methodology of the INTERACT-IT study is available in the final report.25 The methods relevant to our analysis of consultation time and computer use in general practice are described below.
Ethics
Ethical approval was obtained from Leeds East Multicentre Research Ethics Committee (MREC: 09/H1306/60) and governance approval from all NHS trusts. Informed consent was sought from all participants for: (i) recording the consultation; (ii) viewing and analysing the recorded consultation and requesting a post-consultation interview and (iii) permission to request use of images for dissemination or further research.
Practice, GP and patient recruitment
We purposively recruited GP practices representing diverse demography, size and computer software, and arranged to record complete surgeries comprising between 12 and 18 10-min appointments. Patients were advised about the research when booking an appointment in a recorded surgery, and their informed consent was obtained by researchers upon arrival.
Multichannel video recording
We used established methodology to undertake multichannel video recording of consultations.19,26 Three cameras recorded the interaction, and a video output recorder captured the computer screen. Using editing software images, audios and screen capture were synchronised and rendered into single views for analysis.
Post-consultation interviews
We purposively selected exemplar consultations from each surgery for interviews with the clinician to encompass a range of clinical scenarios, patient demographics and computer use. The GP watched the recording and provided a commentary on the consultation, specifically including a discussion of the time and efficiency of computer use.
Data production and analysis
Measuring consultation time
We used OBSWIN software, version 3 (Antam Ltd., London), to time duration of consultation activities.27 The trained rater (JH) marked the beginning and end of computer activities which was used to produce a visual ‘map’ of computer use throughout the consultation. In order to calculate ratios of computer use, we defined the stages of the greater consultation28 as: preparation, patient consultation and post-consultation (Table 1).
Computer use cases
We considered that the GP was the primary actor interacting with the system (EHR) in various use cases via the computer (an object) on behalf of or with the patient or their carers (also actors). We observed use cases in the greater consultation with UML, an industrial standard modelling language widely deployed within the healthcare system community.13–15 The use case has purpose and duration affording interpretation of different preferred styles of use.29 Following discussion with multidisciplinary advisers and participating GPs, we identified six use cases [reviewing the record, ordering tests, referring the patient, prescribing, updating record and using other/external information technology (IT)] as relevant to both clinical consultations30 and EHR designers (see Table 2 for detailed descriptions).
Mapping computer use within the consultation
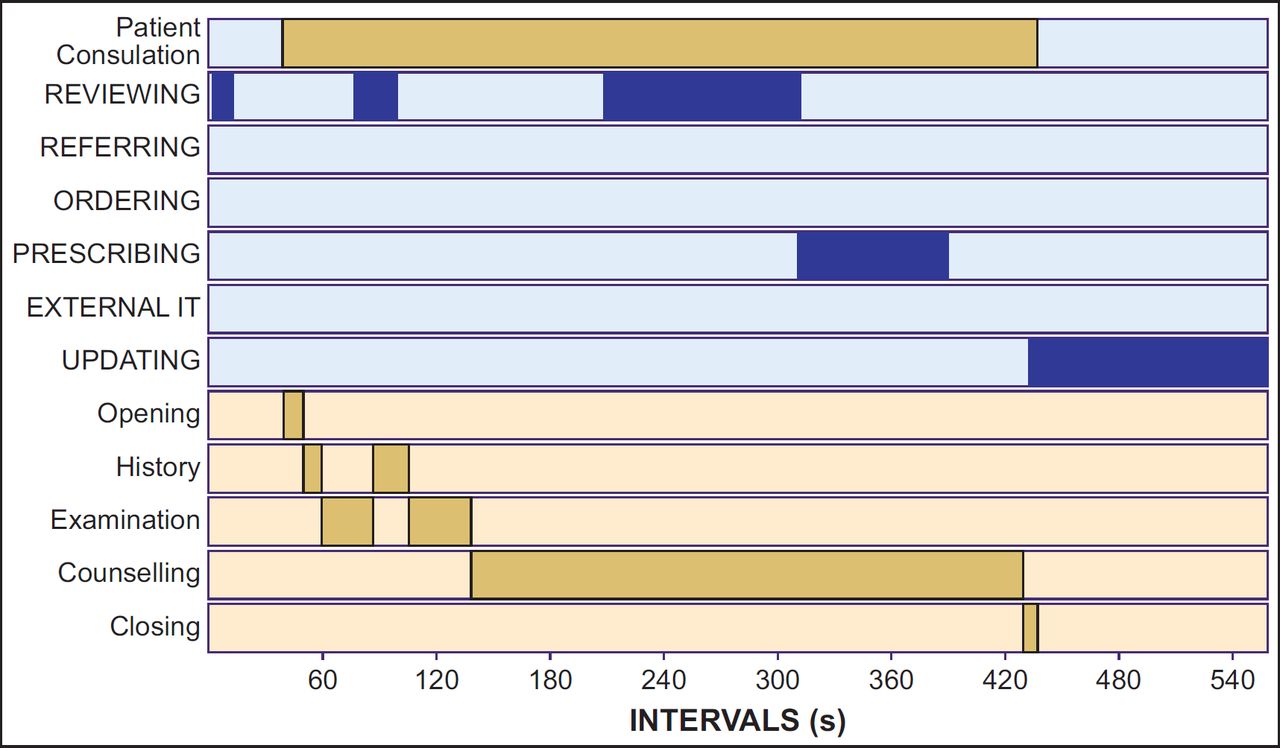
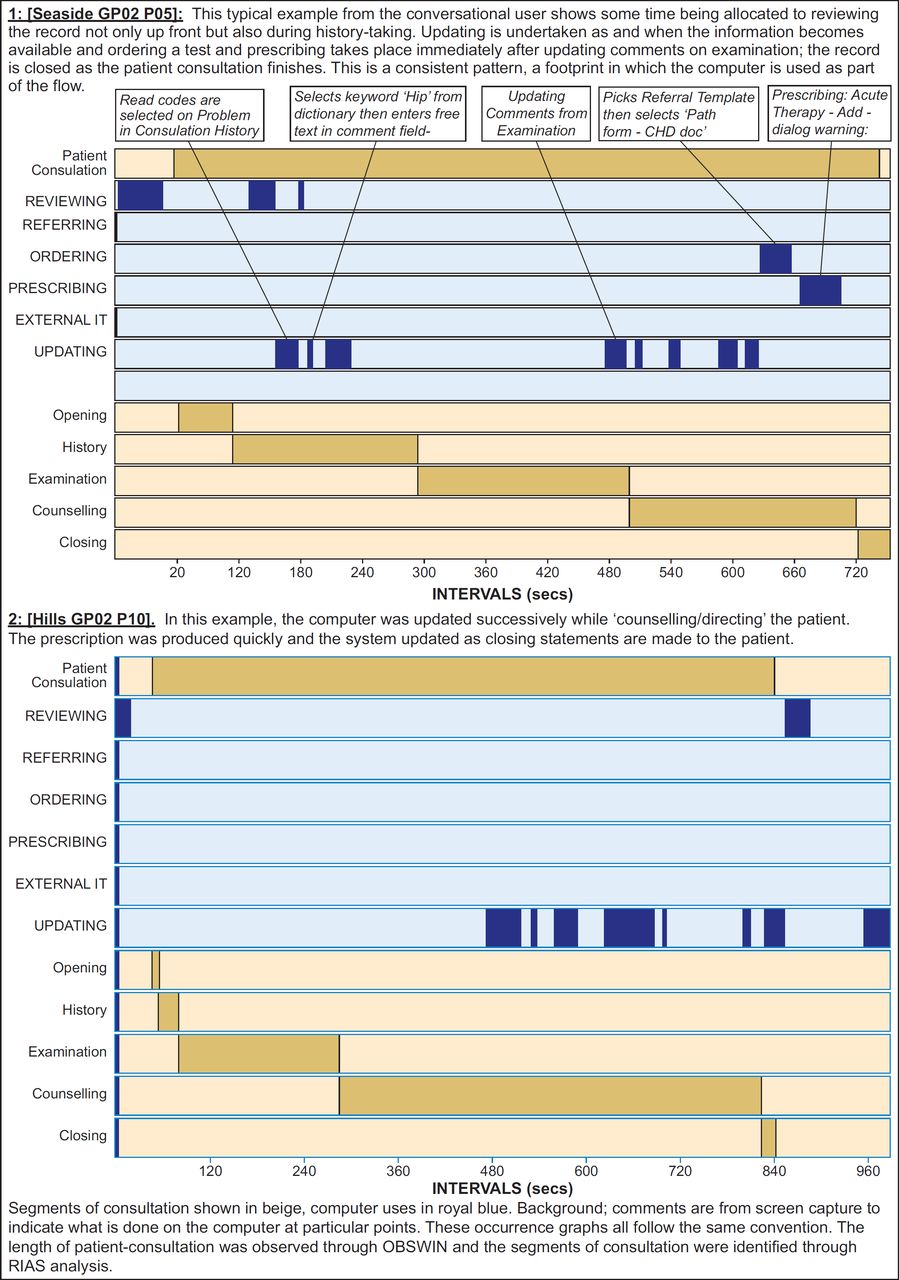
We mapped computer use to the phases of the patient consultation derived from the Roter Interaction Analysis System (RIAS) (coded by SB). RIAS is an established validated tool31 which divides the consultation into five over-arching stages (Table 1). We combined timings of these stages with computer use timings from OBSWIN within an MS-Access database to produce ‘occurrence graphs’ (visual representations of computer use cases within the stages of the consultation), to enable analysis of patterns and map the overall computer use.
Classifying consultation styles
We interpreted use styles17 as minimal, where (apart from prescribing) computer use occurred outside patient consultation, block, if the GP completed computer tasks in one bout and conversational, where updating occurred in frequent short bouts throughout patient consultation. We used number of bouts of computer use as a proxy for conversational (frequent short bouts) versus block or minimal use (few potentially longer bouts), but needed video recordings to identify block use (e.g. explicit signposting of computer by verbal or non-verbal means).
Results
Characteristics of the practices
We observed 112 GP consultations from 8 GPs in three practices (pseudonyms: Seaside, Church and Hills). The details are in Table 3. All practices were paper light using the EHR to manage consultations, administrative tasks, prescriptions, investigation results and correspondence. Seaside (three GPs) used INPS (In Practice Systems Ltd.) Vision software, and Church and Hills (five GPs) used EMIS (Egton Medical Information Systems Ltd.) PCS.
Using the time before, during and after the patient consultation
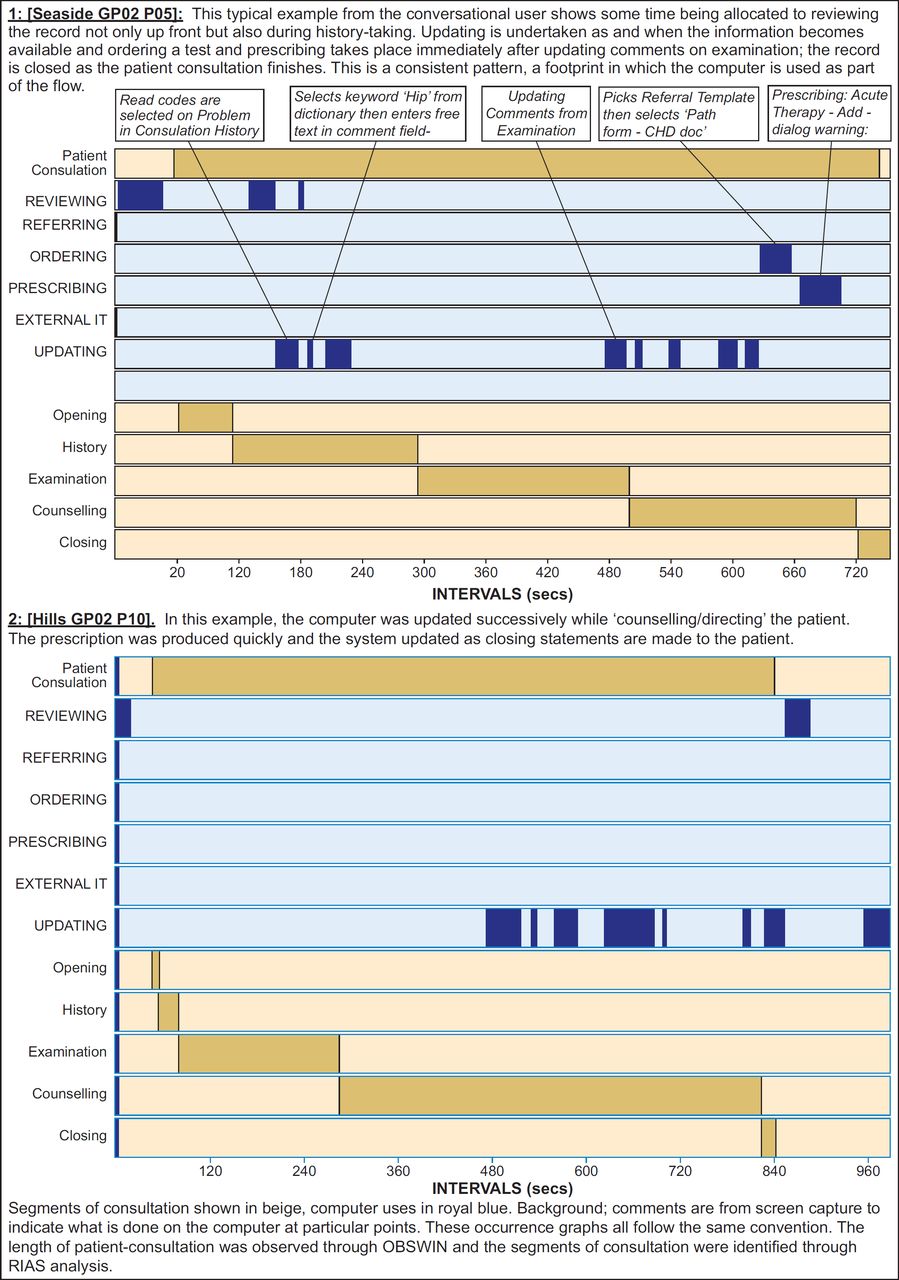
Overall, the mean duration of the greater consultation was 12 min 45 s (765 (SD 290) s) and the patient consultation 9 min 29 s (569 (SD 217) s) (see Table 1 for definitions). On average, the patient consultation occupied about threequarters of the greater consultation; however, there were differences in how this time was allocated or managed. For example, Seaside GP02 spent 87% of the greater consultation with the patient accomplishing his main computer work in that time.
Computer use took 35% of the greater consultation, but typically was concentrated before (reviewing the EHR in preparation) and after (updating the EHR) the patient consultation (Table 4). The three GPs in Church, Seaside GP01 and Hills GP01 exemplified this pattern using the computer for about half the pre-consultation preparation, 20% or less of the time within the patient consultation and around 80% of the postconsultation. The main outlier is Seaside GP02 (and to a lesser extent Hills GP02) whose computer use occupied 45% of the time with the patient with less time updating the records post-consultation. It was observed that these two GPs were adept at multitasking – updating ‘conversationally’ while interacting with the patient.
Timings and patterns of computer use throughout the greater consultation
The duration of computer use and the percentage of time in each section of the greater consultation are detailed in Table 5. Each use case is described below quantitatively and qualitatively.
(1) Reviewing the EHR
On average, reviewing took 80 (SD 64) s, occupying an average of 39 s (37% of the pre-consultation) and 55 s (7.6%) of patient-consultation time). Seaside GP01 and Hills GP01 particularly took time reviewing the past history to prepare for consultation in anticipation of complex clinical situations.
‘I feel like I probably review the records more before someone comes in but in a – consultation where I’m a bit less certain about what I’m going to do I’ll review them more during’. [Seaside GP01]
‘Yeah it depends very much on the consultation if I’ve got somebody complicated about to come in then looking at the notes beforehand can take a while’. [Hills GP01]
Screen shots and descriptions of this preparatory reviewing in EMIS and Vision are shown in Supplementary Tables 1 and 2 in the Appendix. The basic pattern, adapted for clinical circumstances, showed a four-part process:
explore recent consultation history (31 s);
check medications (4 s);
review results/correspondence (up to 29 s, if relevant);
review recent consultations (8 s).
(2) Updating the EHR
Typically, updating took 103 (SD 46) s occurring mainly after the patient had left, though two GPs showed a conversational style of use, sometimes updating continuously throughout the patient consultation. Other GPs also updated the EHR during the patient consultation, but for specific purposes:
‘Yeah, but I might put in facts ... you know, if you do a blood pressure I’d usually do that at the time but I wouldn’t write up my big bulk of notes until the patient has gone generally’. [Seaside GP01]
Reasons for avoiding updating during patient consultation included needing time to select the correct ‘read code’ or not being ‘rude’ to the patient [Seaside GP01]. In contrast, Seaside GP02, who regularly updated the EHR in the presence of the patient, felt that they could have more time with the patient and save time later.
‘You can adapt the system to whatever you want, it doesn’t have to be perfect, but the basic dichotomy is that you cannot perfect your note keeping and your computer skills on the consultations at the expense of the patient. But you can’t give all your time to a patient and rush through your note keeping because you will then get substandard note keeping or if you do both well you will overrun horribly by two hours’. [Seaside GP02]
(3) Referring patients
In total, 13 referrals were made in 12 consultations. Although the decision to refer was made during the patient consultation, the process of referral was done after the patient had left.
‘Referrals I never do with the patient there so that would always be done after they’ve gone if I was dictating a referral.... Yeah, I don’t get time during’ [Seaside GP01]
Seaside GP02 said that they would do the referral with a patient if they thought this was appropriate, but we did not observe such an event.
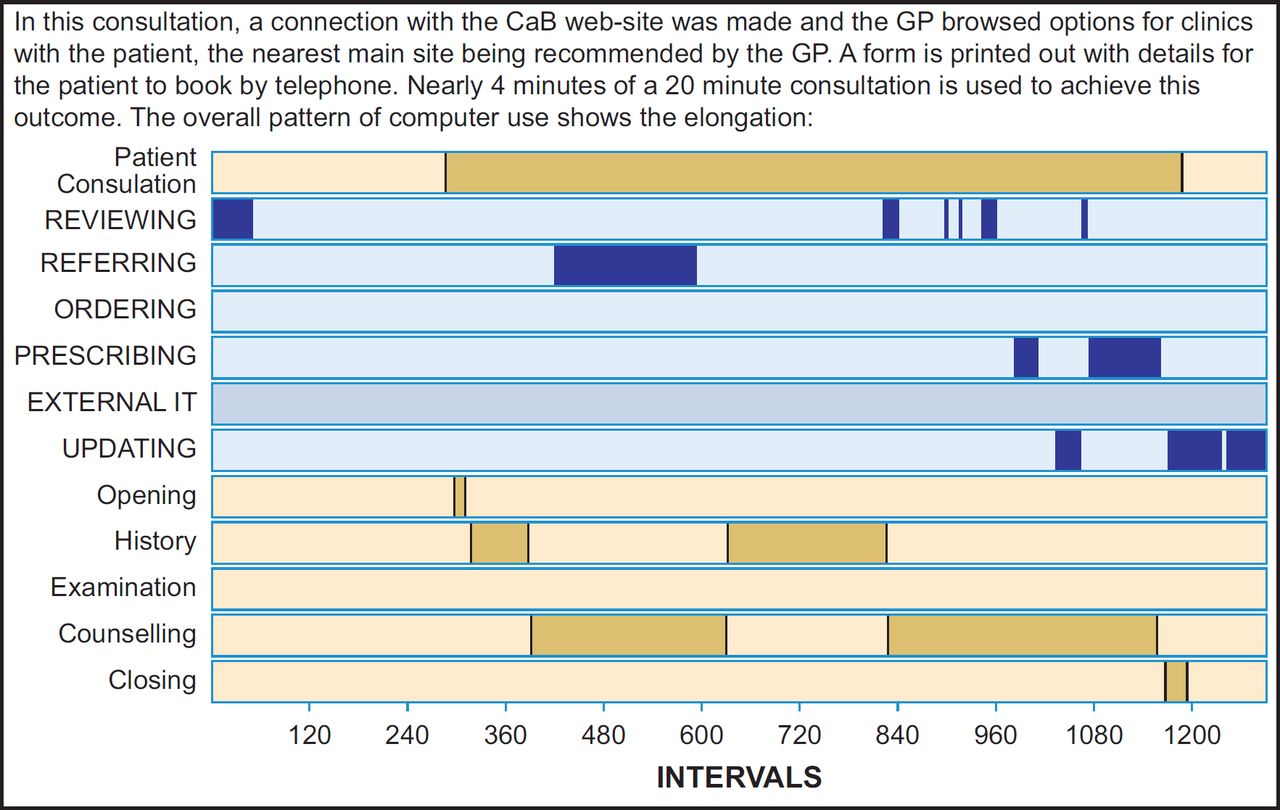
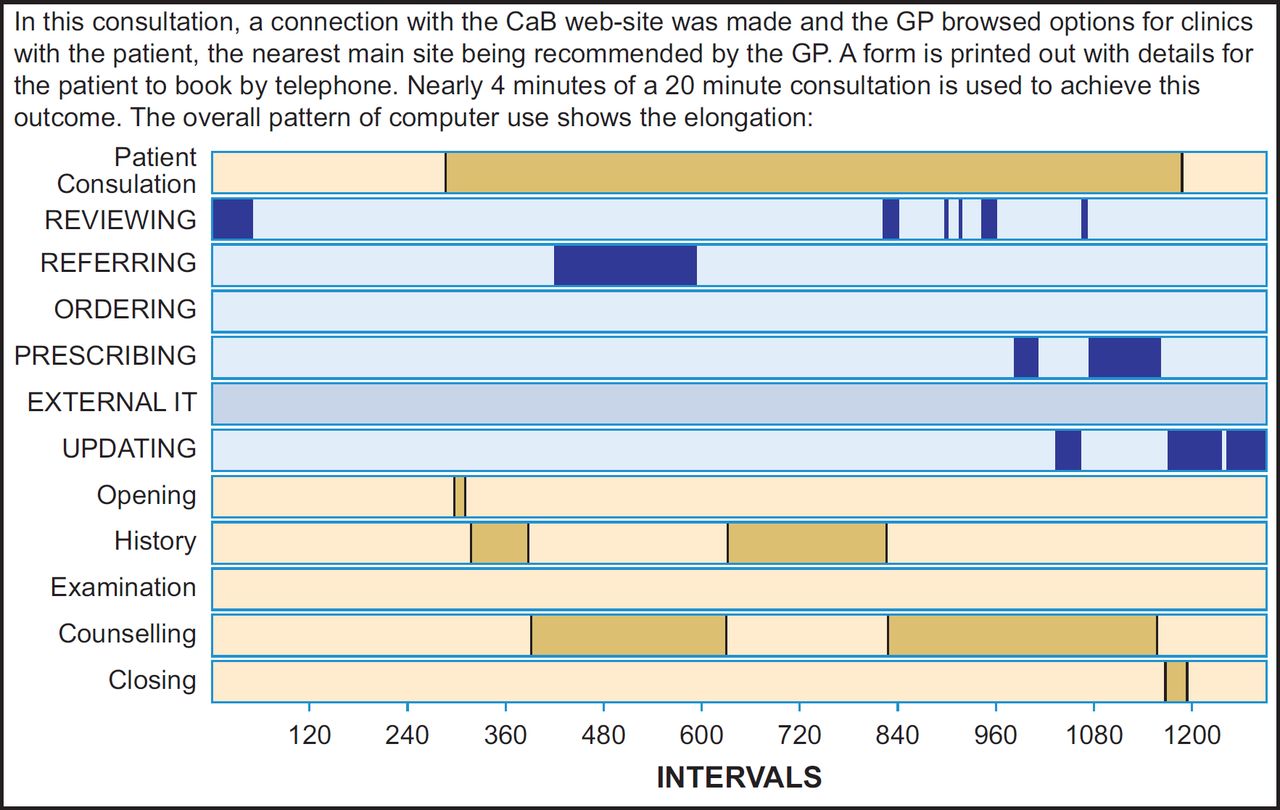
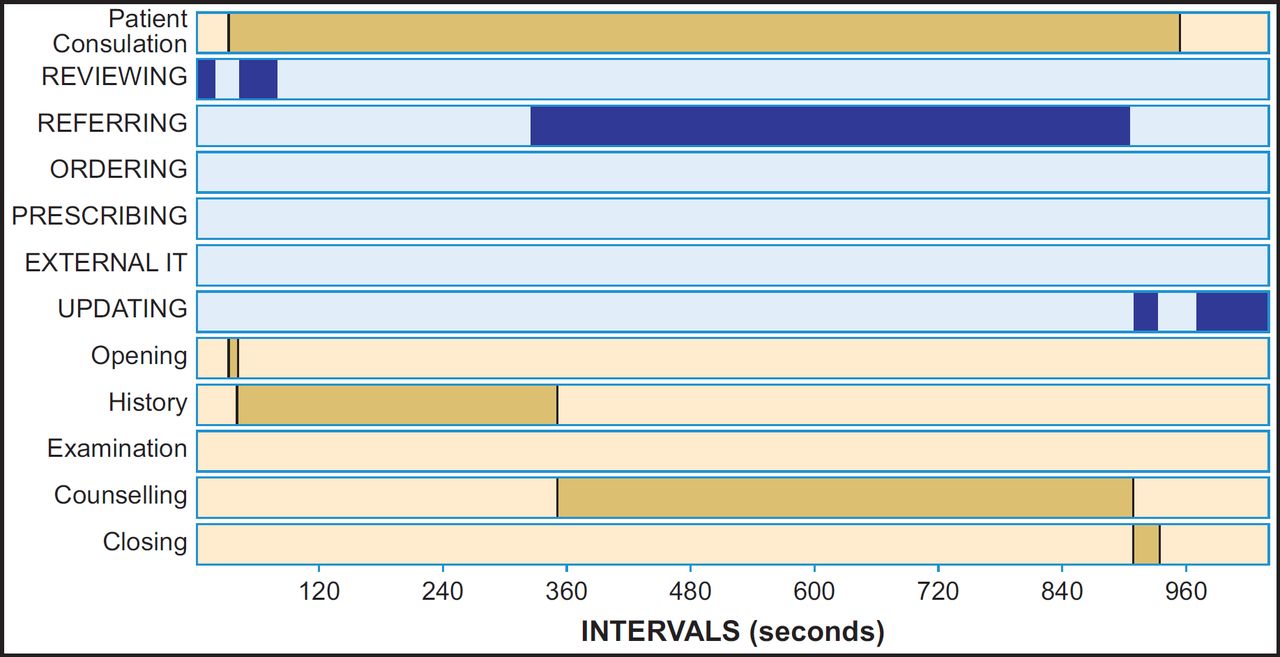
‘Choose and Book’ (CaB) was available in all the practices, but generally delegated to administrative staff. On the two occasions that we witnessed its use in the consultation, the process partially worked (only going so far as printing out forms for the patient to complete later), and on a third occasion, it failed completely, despite using up 10 min (63% of patient consultation time). (Supplementary Figures 1 and 2 in the Appendix describe these events in detail) This was not a one-off experience for the GP:
‘...every time I open Choose and Book I actually feel quite anxious it’s not going to work and 1) that’s going to not be good for the patient but secondly, actually it’s going to waste my time and I’m going to be back to square one with just dictating a letter…’ [Hills GP02]
(4) Ordering tests
The process of ordering tests differed in each practice. In Hills and Church, EMIS online integration was used usually post-consultation. In Seaside, one of the GPs had designed a computer template which self-populated with patient details. This took only about 20 s to complete and was used routinely during the patient consultation.
(5) Prescribing
Prescribing was always done within the patient consultation. The work required and the time taken varied according to the clinical context and between GPs (Table 2). Church GP02, who tended to spend longer on each prescription than the other GPs (109 s versus 64 s), explained how he used the prescribing process tactically to gain thinking time.
‘So sometimes you can use that, the computer, a little bit to just give yourself a bit of thinking time. “Oh, let me just have a look and see what we did last time,” “Let me just see what antibiotics you’re allergic to” It just gives you a few seconds of thinking time just sometimes to come to a conclusion in your own head when it’s not a clear-cut kind of “Do I treat, don’t I?” kind of decision…’ [Church GP02]
Once prescribing decisions were taken, the process of preparing the prescription required navigation through, sometimes complex, dialogue boxes involving informational and safety alerts, though this was a familiar sequence of actions often accomplished in a short period of time.32
(6) Other computer-related tasks
Less common computer uses included accessing external Web-based resources and printing of information leaflets. In Church and Hills, the GPs used Web Mentor to search and print out appropriate information leaflets on eight occasions. In Seaside, FRAX (a Web-based calculation tool to assess 10-year risk of osteoporosis fracture) was used in one consultation.
Computer use in the consultation
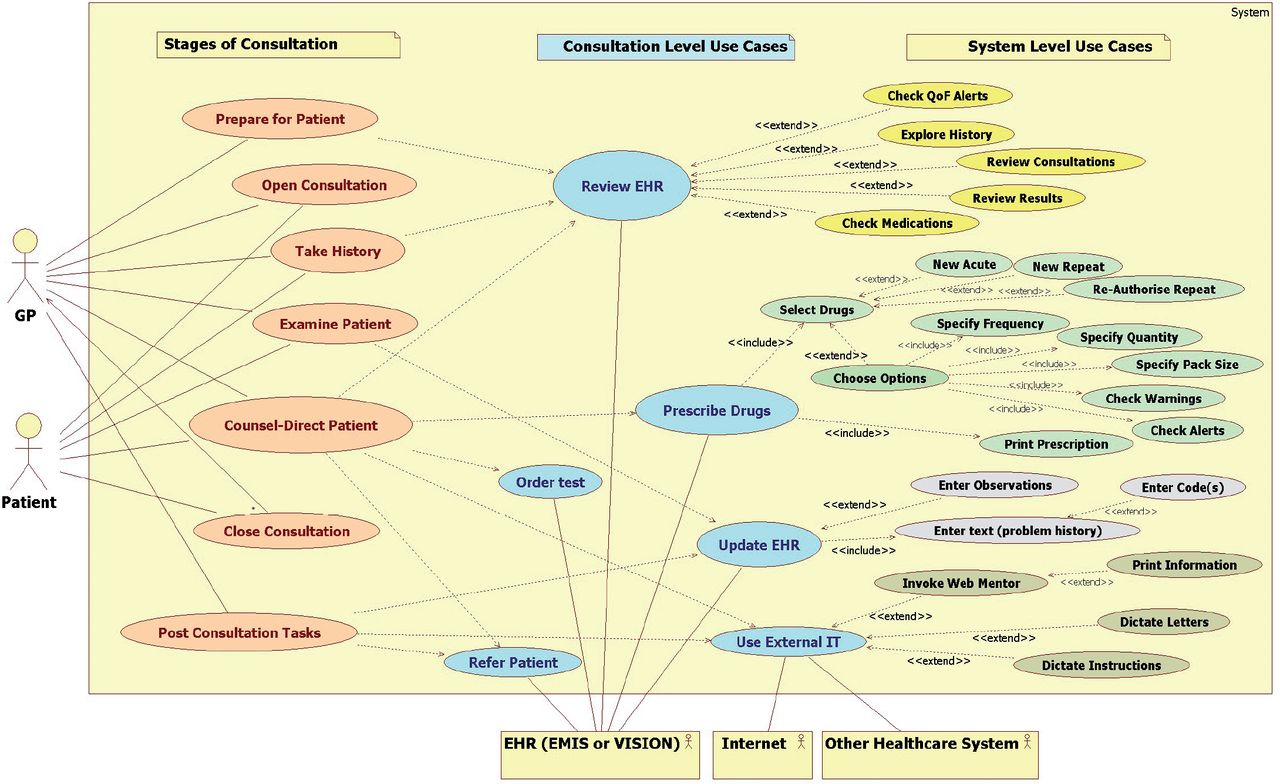
The six main use cases together with their component task structure are depicted in relation to the primary uses of time in managing the stages of the consultation in Figure 1. This holistic framework shows relationships between tasks at different levels of granularity and particular sets of system-level computer-related tasks requiring the GP’s attention. We may associate particular use cases with certain phases of the consultation, but the order in which these take place depended on clinical context and clinicians’ choice. In addition to this overview of computer use, we also looked at individual cases to see how patterns of use were constructed.

In UML, uses cases are depicted at different levels typically: ‘kite’ (high) level, ‘sea’ level and ‘fish’ level with most behavioural use cases being written at sea-level and functional use cases at system level. In this schema, use cases amenable to visual observation are defined at the sea-level of the consultation. Closer inspection of screen capture (at fish level) showed other system level uses cases being called part of the work flow; conventionally associations are marked as, <<include>> if ,mandatory or <<extend>> if optional.
Classifying the consultation: styles of computer use
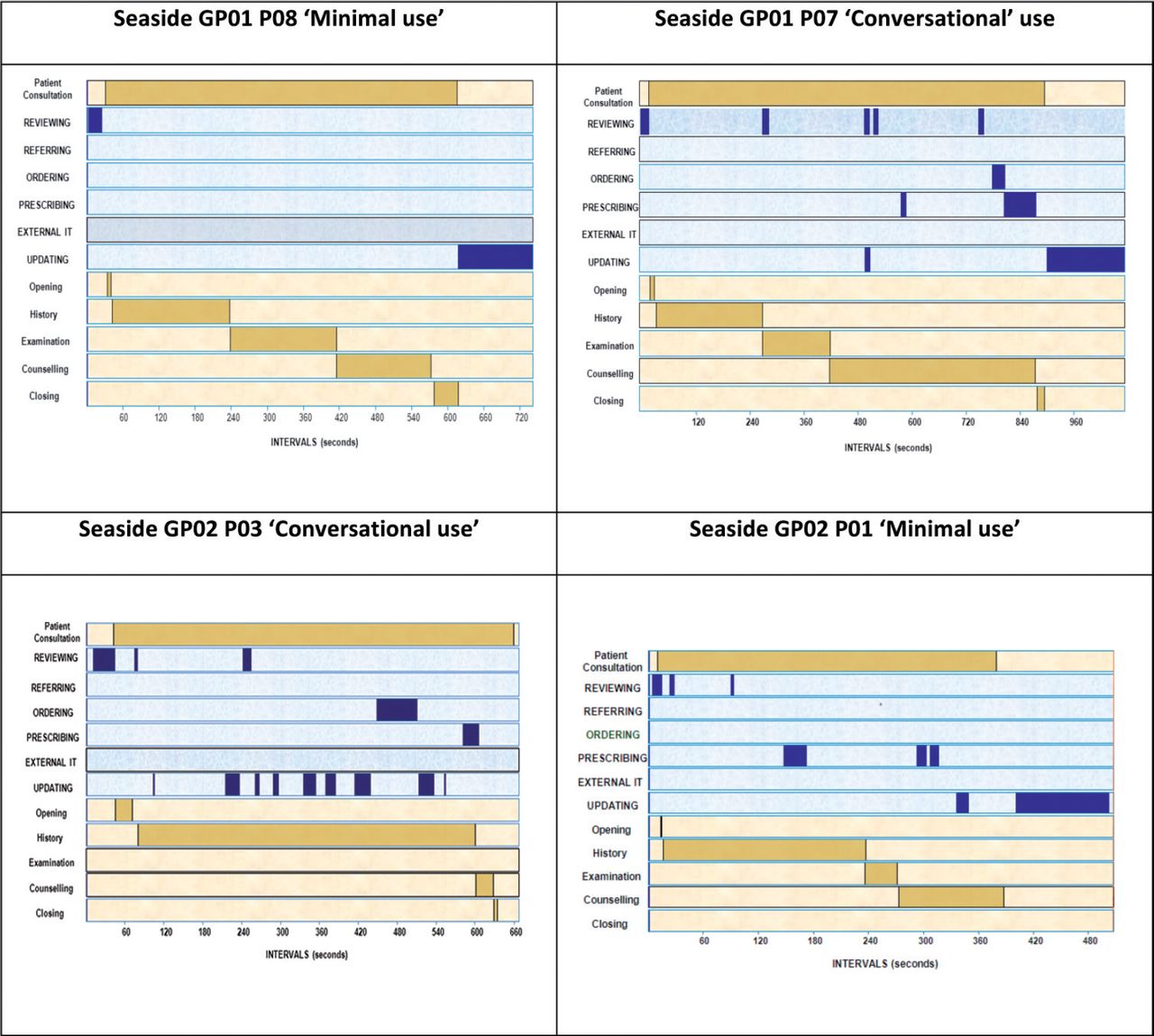
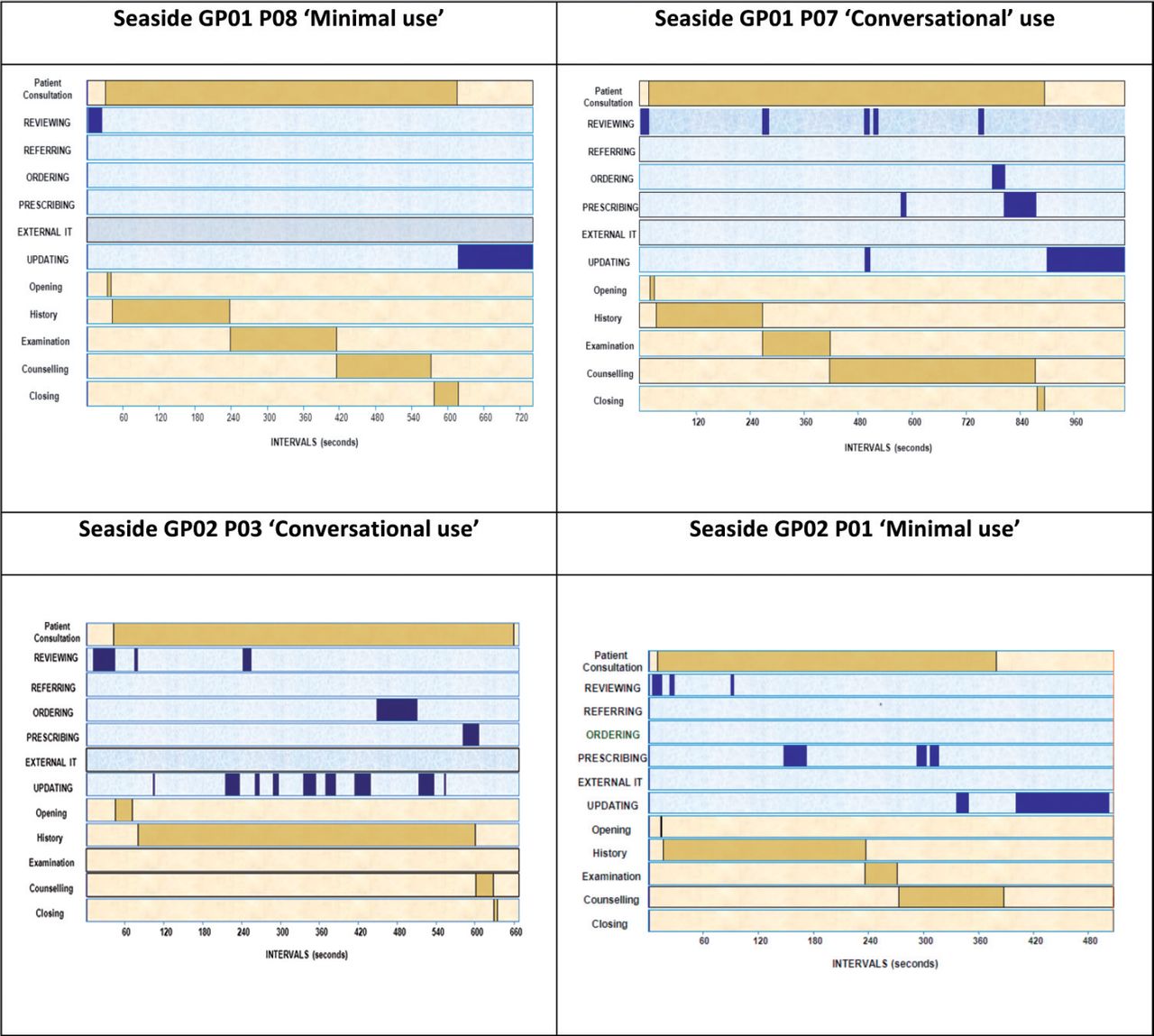
We ascertained styles of computer use for each GP, observing the following patterns or styles (illustrated in Supplementary Figures 3–5):
Minimal use
For example, Hills GP01 rarely updated the EHR during the patient consultation (mean bouts of updating = 0.4 (SD 1.1); mean time spent updating = 19 s in only 3 consultations). Both Seaside GP01 and Hills GP01 actively prepared by carefully reviewing history and results to be ready for the patient consultation and also invested time afterwards to ensure correct coding:
‘Normally I would spend a minute or two with the consultation just being me and the computer before getting them then it’s completely different because I tend to get patients from the waiting room so you then get a bit of the consultation which is not technically part of the consultation but it is part of the introductory part and the information gathering seeing how people walk down the corridor or whatever’ [Hills GP01]
Block use
Undivided attention was sometimes needed for prescribing; for example, Church GP02 actively blocked discussion as he used computer prescribing as ‘thinking time’:
‘And sometimes I say things like “I’m sorry I’m having to spend a bit of time on the computer, I’m just looking over this” so I’m sort of signposting what I’m doing rather than, erm... yeah, to try and keep them engaged, I guess, with what you’re doing whilst you’re fiddling around on the computer’. [Church GP02]
Others on occasion partially interrupted the consultation to update the record:
‘I sometimes do type, very occasionally, when the patient’s still in the room and they’re still speaking but often they’re speaking and it’s not particularly useful what they’re saying so I use it just to...’ [Church GP01]
Conversational use
Consistent with their observed conversational use of the computer, Seaside GP02 and Hills GP02 registered a mean of 11 and 8 bouts, respectively, of computer use (mainly updating the EHR) within the patient consultation. In contrast, the other GPs’ computer use was a mean 3.2 bouts per patient consultation.
Adaptation of style
Despite preferences in computer use, all GPs adapted their style to suit individual consultations and patients. Seaside GP02 specifically expressed the need for a flexible approach to use of the computer:
‘Each consultation is different for every patient, different every time, for every patient it can be different every time’. [Seaside GP02]
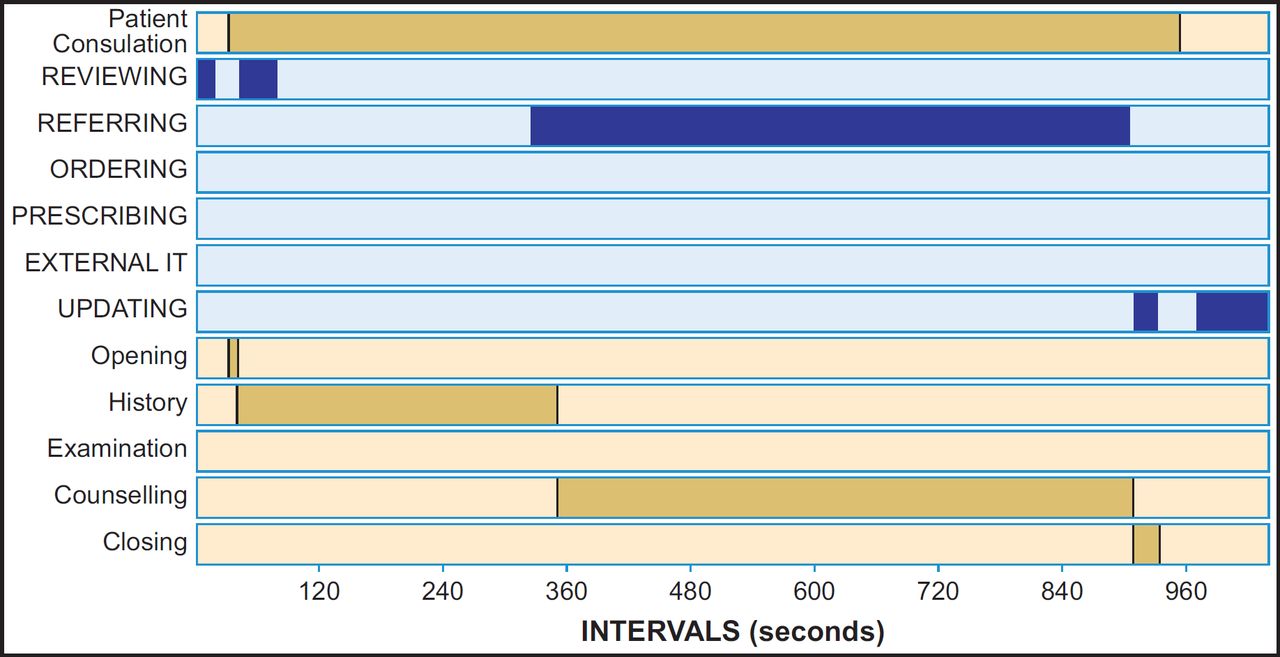
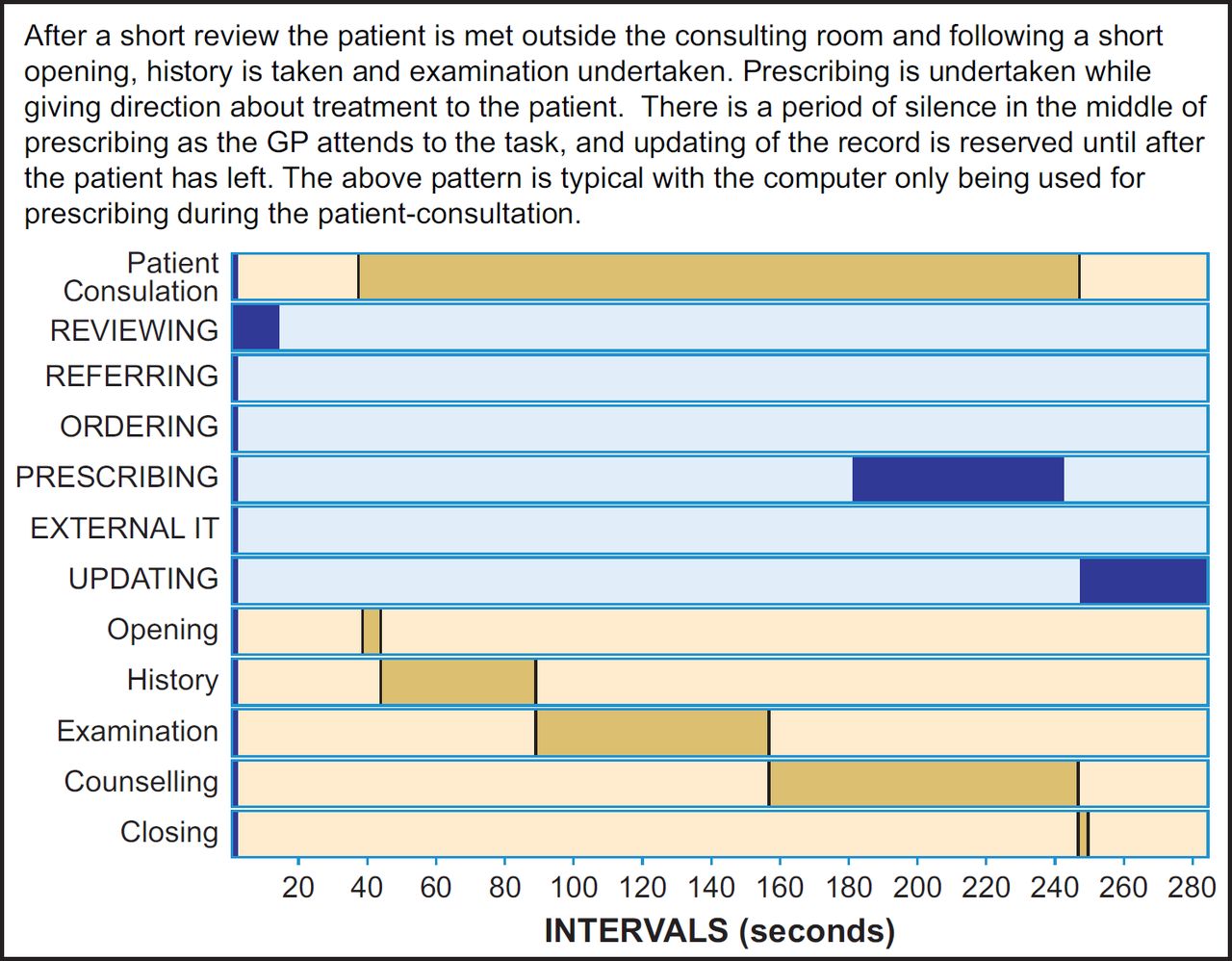
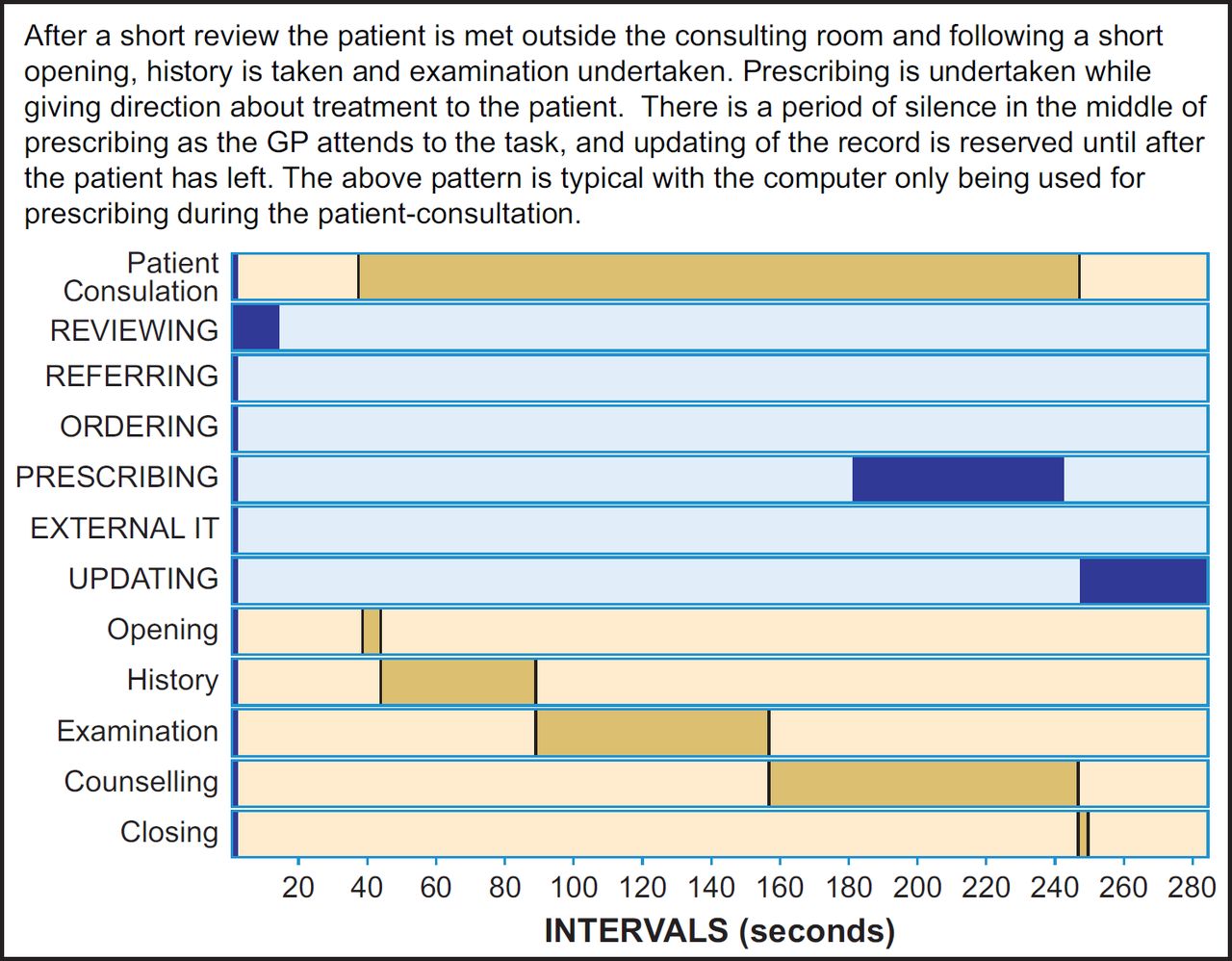
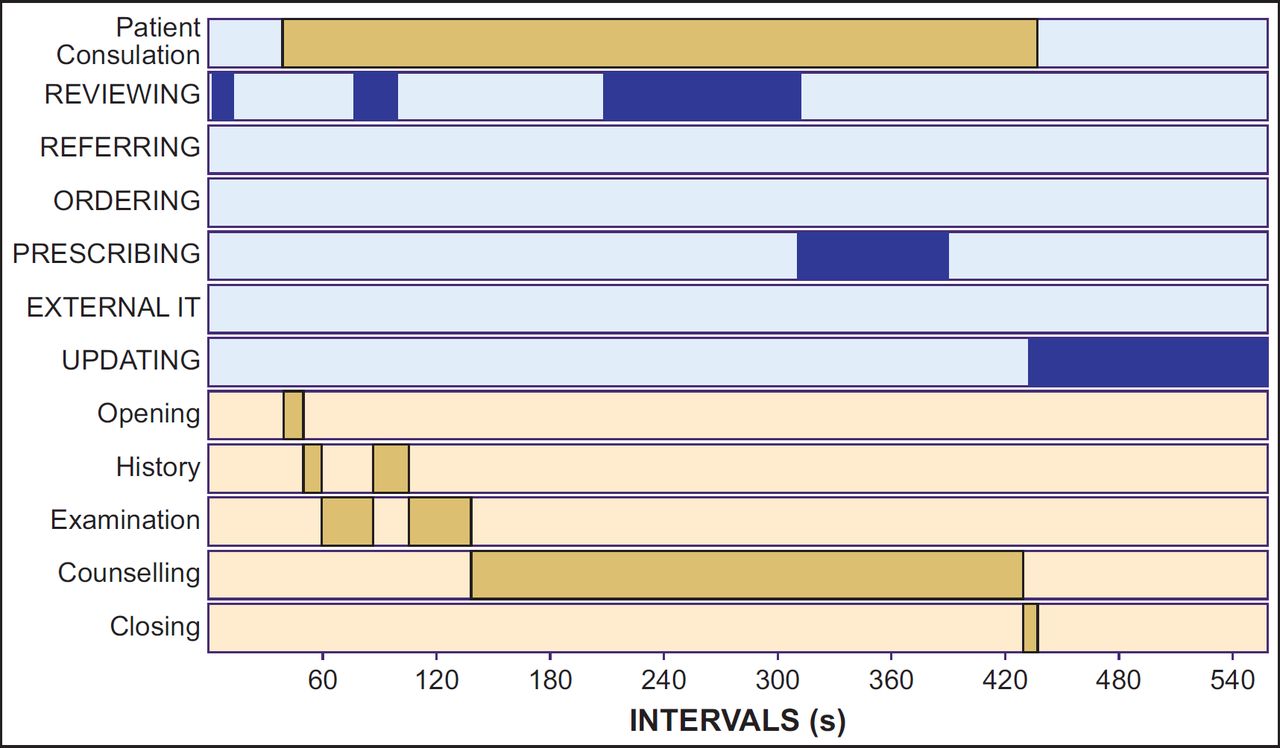
The overlap in consulting styles is illustrated in Figure 2, and contrasting consultations from Seaside GP01 and Seaside GP02 are in Figure 3.

The blue lines are the two GPs who tended to use the computer conversationally (Seaside GP02 and Hills GP02). The other six GPs, whose pattern tended to be blocking or minimal, are illustrated in grey. Although there is a difference in the patterns, there is also very considerable overlap between the two groups as the GPs adapted their style of computer use to the individual consultation.
Discussion
The GPs in our study used the computer for about onethird of the greater consultation, but much of this time was concentrated before and after the patient consultation. On average, GPs used the computer for a quarter of patient consultation time with ‘reviewing’ patient records and ‘prescribing’ being the most common use cases. The time allocated by GPs varied according to GP’s preferred styles of computer use. Minimal/block users used the computer for a mean of 1 m 56 s (20% of patient consultation time) compared to conversational users whose updating of the patient record extended computer use to a mean of 3 m 28 s (40%). Despite preferences for ‘conversational/ minimal use’ styles, GPs were very flexible in the way they worked, adapting how they used the computer to the clinical context. Potentially troublesome or time-consuming tasks were postponed or delegated in order to manage time within the consultation.
Strengths and limitations
We analysed consultations from eight GPs in three surgeries using the two most commonly deployed GP computer systems giving transferability and depth to our findings. Nevertheless, we may not have encompassed all styles or types of consultations.
Our sample size was relatively small for quantitative analysis, but this allowed detailed qualitative investigation, enhancing our understanding of quantified observations. While large-scale surveys would be needed to enumerate prevalence of different use styles, our in-depth mixed methodology meant that we could explore differences in use strategy.
One of the strengths of our approach is that we captured all computer use before, during and after patient consultations, though not any postponed or delegated tasks. The method of use case analysis is particularly suited to longitudinal studies/evaluations involving embedding of new or upgraded EHR systems in practice.
Styles of computer use
Current perceptions of computer use in general practice,33,34 and the research that underpins it,35–37 tend to represent the computer as a static object in a consultation and give stereotypical accounts of GPs styles of use. We adopted the conversational/block/minimal styles in analysing bouts of computer use17 and found that although GPs had ‘preferred styles’, they were very flexible in the way they worked, readily adapting their computer use to the clinical context. Understanding such patterns of adaptation between clinical contexts is important for professional training.34 We may consider ‘conversational use’ as a tactic rather than trait.
Time taken for computer use in the consultation
Over 25 ago, computer use took 7% of the 8-min patient consultation.18 In our study, this had increased to approximately 25% of the patient consultation. This may not, however, represent an increase in workload as many functions previously performed on paper are now computerised. The mean duration of the patient consultation was 9 min 29 s which compares with the 10-min consultations for hypertension reported in 2002 in which computer use occupied 20% of the time.23 Thus, our data do not support the widely held perception that computer use lengthens the consultation.1–3
Workarounds and disruptive technologies
CaB, designed to enable GP and patient jointly to arrange convenient outpatient appointments,38 proved to be cumbersome, unreliable and poor use of time within the consultation. Hence, most GPs worked around the problem by delegating the use of CaB to their secretaries. Prescribing alerts, delivered at the point of printing a prescription, were often over-ridden as management decisions had typically been taken and/or negotiated with the patient earlier in the course of the consultation.32 Reducing the incidence of such workarounds requires designers to understand clinical practices and processes.
Our observations suggest that far from being a new addition to a ‘normal’ consultation as it was described in 1986,9 computer use has become the norm in the GP consultation. While computer use is taken for granted in consultation, some processes (e.g. CaB or prescribing alerts) involve workarounds to ‘get the job done’, though not necessarily in the intended way. In this sense, the IT use has become ‘infrastructural’ – invisible except on breakdown.39
Implications
Our methods for differentiating style by use cases could be developed further and applied to a larger more varied sample. Understanding GPs’ versatility in clinical strategies for use of the computer and other health technologies and how they form a reliable and regular work rhythm is particularly relevant for designers and clinician leads involved in implementing usable and time-efficient changes in EHR decision support within the consultation. In this light, just as our data marks a sea change from the main categories used in TIMER,9 similar observational studies might inform design levels (e.g. for pathways of care40) in future EHR system development.
For example, future work could explore the association of parameters (such as whether the consultation was initiated by the patient or professional) on bouts and duration of computer uses cases within the consultation. Furthermore, while we privileged the GP’s perspective on the consultation, our methodology could be used by system designers or clinical trainers for third person evaluation of the efficiency of GP computer use.
Conclusions
After four decades of use, integrating the computer into the flow of the patient consultation has been achieved to a significant degree in primary care consultations without increasing the overall consultation time. GPs readily adopted different styles of computer use in different consultations, challenging classifications that seek to stereotype GP computer use.
Natural clinical workflow determines boundaries for acceptance of new IT functions. Designing systems that support the versatile working styles of clinicians require an understanding of the fluid application of computer tasks within the structure of the clinical consultation. Seeking further time efficiency and improvement through IT systems needs to be guided by a clear vision of how organisation of information for diagnosis and treatment of patients’ conditions can reduce time pressure within and around the consultation.
Funding: This work was funded by the NHS CFH Evaluation Programme (NHS CFHEP 010). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NHS CFH Evaluation Programme or the Department of Health.
HP was supported by a Primary Care Research Career Award from the Chief Scientist’s Office of the Scottish Government at the time of the research.
Acknowledgments
We are grateful to the officers of the Primary Care Research Networks in supporting practice recruitment, the practices, GPs and administrative staff for their active participation and the patients who agreed to have their consultations videoed. We thank Prof. Simon de Lusignan who chaired the ITSC supported by Antony Chuter (lay advisor), Stephen Corbett (CFH sponsor) and Lee Priest (representing the funder). We also acknowledge the contributions of Dr. Guro Huby (an investigator on the project until her retirement), Elizabeth Neill (study secretary), Dr. John Harries (researcher in the early stages of the project) and Andy Pryde (technical advice on video recording).
Appendix
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Footnotes
Competing interest: None
Contributorship: HP, AS, KC and RW conceived the idea for the study, developed the protocol and secured funding, HP was the principal investigator and with AS, KC and RW led study administration, data analysis and interpretation of results. JH, FT and HM undertook the data collection, handling of data and data analysis. SB assisted with RIAS coding and analysis. All authors had full access to all the data, and were involved in interpretation of the data. JH and HP wrote the initial draft of the paper, to which all the authors contributed. HP is the study guarantor.
Data sharing: We do not have consent to share the data.